
Abstract
Abstract
Background:
The aim of this article is to standardize the laparoscopic technique to treat direct inguinal hernia in pediatric patients.
Patients and Methods:
In the last 3 years we treated laparoscopically 163 patients with a diagnosis of inguinal hernia. In 7 patients we discovered laparoscopically a direct inguinal hernia. This study is focused on the management of these 7 cases (4 girls and 3 boys; median age 4.6 years). They presented a right defect in 4 cases and a left defect in 3 cases. Six of 7 patients had been already operated for an inguinal hernia and presented a recurrence of the hernia. We used three trocars, 5-mm 0 degree optic, and two 3-mm instruments. In each case, after the resection of the lipoma using the hook cautery, the defect was closed by means of separated stitches. In every case we used the vesical ligament as an autologous patch to reinforce the closure of the defect.
Results:
The average operative time was 35 minutes. All the procedures were performed in a day-hospital setting. We had neither conversions nor complications in our series. With a minimum follow-up of 1 year, we had no recurrence.
Conclusions:
Laparoscopic identification and repair of direct inguinal hernia in children is a safe and effective procedure to adopt. The key points of the technique are the resection of the lipoma, the closure of the defect using separated, nonabsorbable sutures, and the use of the vesical ligament to reinforce the suture. We believe that in case of recurrence of inguinal hernias after inguinal approach, laparoscopy is the gold standard technique to identify and treat the cause of the recurrence itself.
Introduction
Patients and Methods
In the last 3 years we treated laparoscopically 163 patients with a diagnosis of inguinal hernia. In 7 patients we discovered laparoscopically a direct inguinal hernia. This study is focused on the management of these 7 cases. These 7 patients (4 girls and 3 boys) with an age variable between 3 and 9 years (median 4.6 years) presented a right defect in 4 cases and a left defect in 3 cases. Six of 7 patients had been already operated for an inguinal hernia in another institute via inguinal approach and presented a recurrence of the hernia on the same side. The seventh patient had a general diagnosis of inguinal hernia preoperatively and we discovered the presence of the direct defect during the laparoscopic procedure. All the patients were operated in general anesthesia with an orotracheal intubation. In each case the bladder was emptied using a Nelaton catheter to prevent the full bladder from covering a medial defect as direct or femoral hernias. Pneumoperitoneum pressure varied between 8 and 11 mm of Hg. We always used three trocars, an optic of 5- or 10-mm 0 degree and two 3-mm instruments. The 20-mm needle (3/8 of circle) was always introduced transparietally with a suture length of 15–18 cm. All the direct defects were larger than 10 mm and in each case we found a big lipoma adherent to the hernia sac (Figs. 1 and 2). The internal inguinal ring was closed bilaterally in all the patients. As for the technical point of view, in every case after the resection of the lipoma using the hook cautery (Fig. 3), the defect was closed by means of separated stitches, using nonabsorbable 2 or 3/0 suture. In each case we used the vesical ligament as an autologous patch to reinforce the closure of the defect (Fig. 4). The use of vesical ligament allows an easy closure of the defect without tension on the defect's borders.
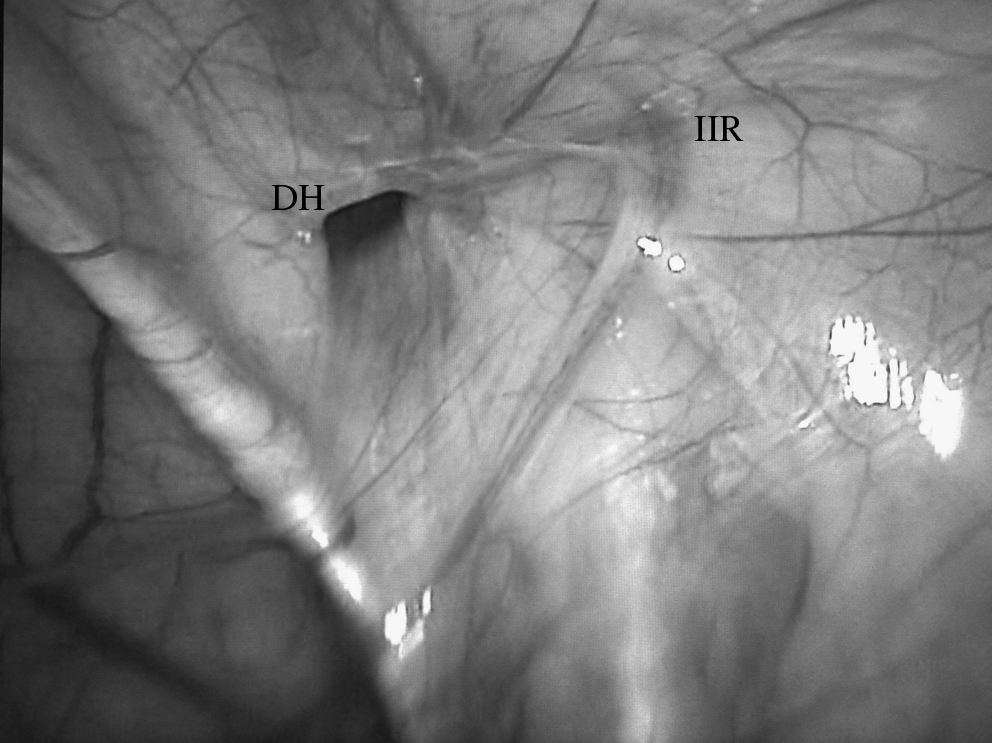
Laparoscopic appearance of a right DH. DH, direct hernia; IIR, internal inguinal ring.
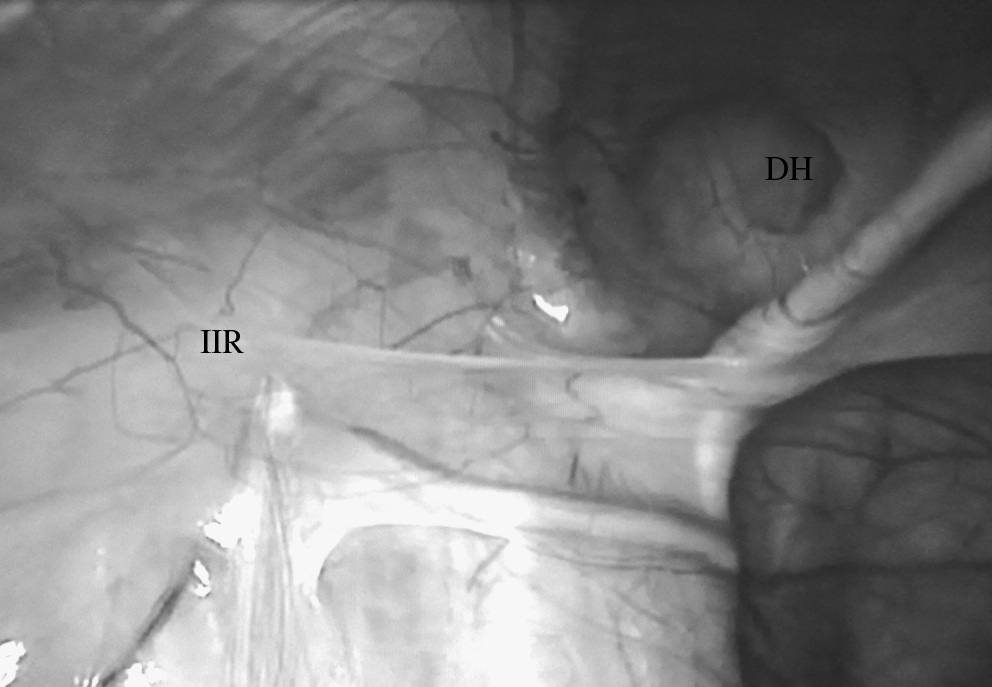
Laparoscopic appearance of a left DH.
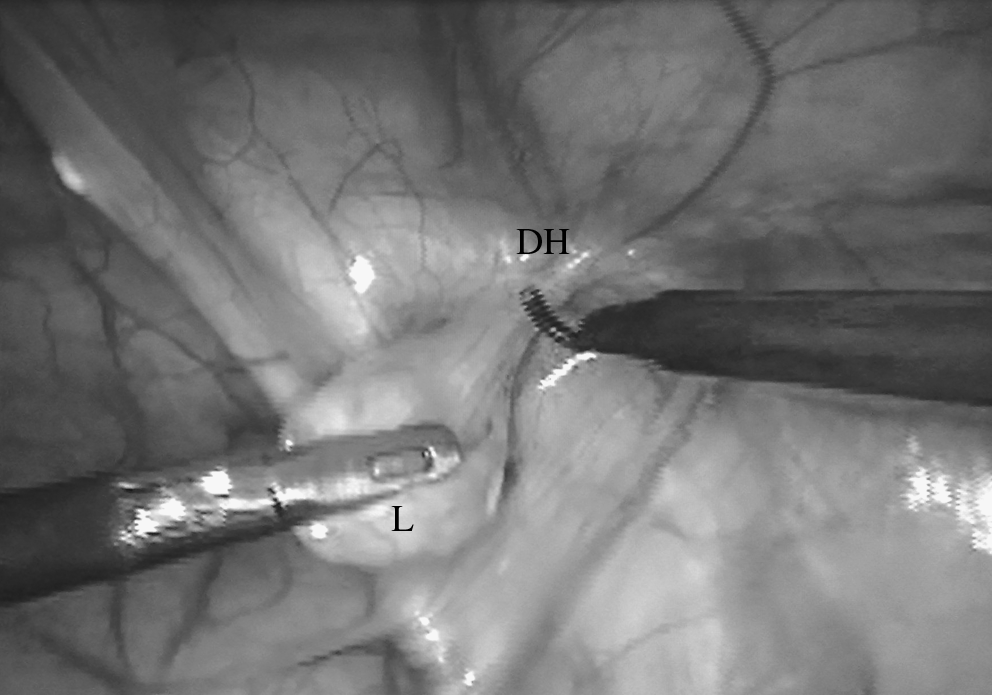
A key point of the technique is the section of the lipoma (L) using the hook cautery.

Laparoscopy view after the closure of the defect.
Results
All the procedures were completed in laparoscopy without recurring to conversion. The average operative time was 35 minutes (20–60 minutes). All the procedures were performed in a day-hospital setting with an overnight hospitalization. We had neither pre- nor postoperative complications in our series. With a minimum follow-up of 1 year, we had no recurrence in our series, and cosmetic result was excellent in all the patients.
Discussion
Direct inguinal hernia is a rare condition in children. 1 In general, direct groin hernias appear as a recurrence after previous inguinal operations for congenital indirect inguinal hernias.10,11 Therefore, direct hernias are often missed during the first operation (6/7 cases in our series).1,2,12 A correct preoperative diagnosis may be difficult and it can be misleading when an inguinal bulge is observed again.5,7 Recently, articles which focus on laparoscopic inguinal hernia repair are more often published in the international literature and the so-called “rare hernias” are more often identified and treated.6,7,13,14 We believe, on the basis of our series, that in case of hernia recurrence after open repair, the cause of recurrence can be a misdiagnosed direct hernia and laparoscopy is the most effective technique to identify and to treat it. We agree that laparoscopic treatment is a safe and valid technique to diagnose and treat recurrent inguinal hernias. It allows an accurate diagnosis of the potential coexistence of direct and indirect inguinal hernias, and it helps to distinguish a true recurrence of an indirect inguinal hernia from a missed direct inguinal hernia (like in 6/7 cases in our series). 7 Further, it avoids an unnecessary exploration of the inguinal canal and the consequent possible risk of iatrogenic injuries to the vas deferens or the spermatic vessels. 2 Based on our 15-year experience on laparoscopic hernia repair, considering that the technique of indirect hernia repair is well-established and standardized, the aim of this article is to standardize the technique of direct inguinal hernia repair. 13 First of all, it is important to remember, for each patient, to empty the bladder before surgery to prevent the full bladder from covering a medial defect as direct or femoral hernias; in our series the bladder was emptied using a Nelaton catheter also if Credè maneuver is as effective as Nelaton use. As for the oblique external hernia, the technique is simple to perform; the first step is the section of the peritoneal vaginal duct distally to the internal inguinal ring circumferentially, and then the closure of the periorificial peritoneum using either a purse string suture or an N-shape suture. 15 As for the direct hernia repair, the technique is different. In fact, first of all in all hernias we found a huge lipoma adherent to the hernia sac; it is wrong to leave the lipoma because it can cause a recurrence of the hernia. For this reason, the reduction of the lipoma into the abdominal cavity and its resection using a hook cautery is fundamental and also easy to perform. As for the defect, the periorificial peritoneum of a direct hernia is more adherent to the defect and it is difficult to perform a purse string suture or an N-shape suture as in the case of oblique external hernia. For this reason it is safer to close the defect using separated stitches. Considering that direct defects, as it happens in our series, are often larger than 10 mm, to avoid tension on the defect's borders after closure, we used the vesical ligament to reinforce the closure. This technique, already described by Lima et al. in 2002, allows to perform a safer closure of the direct defect. 16 In our series, laparoscopy represented a peculiar surgical solution to correct direct inguinal hernia. Another interesting aspect about our study is that all 7 patients were referred to our hospital to be operated in laparoscopy and their parents specifically requested to our group to adopt the minimally invasive technique. It means that laparoscopy techniques are now widespread, also thanks to the Internet, which gives everyone the chance of looking for medical infos. We think that laparoscopy has the advantage of using a uniform, standardized approach for all hernia forms—indirect, direct, femoral, or combinations. This provides, for the first time in surgical history, an objective and reproducible picture/video that is accessible and clear to everyone in the operating room.6,7 The pictures are easy to interpret for all pediatric surgeons.6,7 In the previous studies, direct inguinal and femoral hernias had been found less frequently in the open approach than in the laparoscopic approach. Probably some pediatric surgeons had never seen a direct inguinal hernia or a femoral hernia, among hundreds of hernia repairs in the prelaparoscopy era.6,7,13 Due to the laparoscopic magnification, direct inguinal hernias are easily identifiable and now it is possible to standardize their treatment.4,6,7
We believe that direct hernia repair is more demanding, technically, than indirect defect repair; for this reason it is better to treat this pathology only after developing a good skill in intracorporeal knoting. In conclusion, the laparoscopic approach allows for the first time an objective picture of the anatomy and the true incidence of unusual hernias in children.3,6,7,13 Direct hernias, as our series shows, can be sutured laparoscopically in a safe and efficient manner without recurrence. The key points of laparoscopic direct hernia repair are the resection of the lipoma, the closure of the defect using separated, nonabsorbable sutures, and the use of the vesical ligament to reinforce the suture. We believe that in case of recurrence of inguinal hernias after an inguinal approach, laparoscopy is the gold standard technique to identify and treat the cause of the recurrence itself, which is represented by a direct hernia in a high percentage of cases.
Footnotes
Disclosure Statement
No competing financial interests exist.