
Abstract
Abstract
Background:
Endoscopic thyroidectomy (ET) precludes the long cervical incision of the open procedure. Although endoscopy is an essential tool taught to almost every surgeon, its effective use with regard to thyroidectomy requires understanding its limitations pertaining to trauma and cancer, as well as an understanding of the advantages and disadvantages of the different endoscopic approaches. The development of an ET center in China is discussed here.
Methods:
Overall, 235 patients who had undergone attempted ET in Qilu Hospital of Shandong University in China from August 2001 to September 2010 were evaluated.
Results:
Of the 11 men and 224 women on whom the procedure had been attempted, all but seven successfully underwent ET, 145 (63.6%) via a modified anterior chest approach, and 83 (36.4%) via a breast approach. Age ranged from 17 to 52 years, with a mean of 34.5 years. Surgery was limited, in the case of masses, to lesions smaller than 6 cm ultrasonographically. All patients were followed for at least 3 months. The 24 and 48 hours Visual Analog Scale postoperative measurements were low. Complications included four cases of cutaneous emphysema, five seromas, four episodes of anterior chest discomfort, three transient laryngeal nerve palsies, and four episodes of hypocalcemia. The seven procedures that had been converted to an open procedure comprised two patients discovered at frozen section to have poorly differentiated thyroid carcinoma, two with tumors larger than 5 cm, and three with thyroiditis.
Conclusions:
ET is readily learned, provided the surgeon is competent at both laparoscopic technique and open thyroidectomy. Procedural advantages of an endoscopic approach include superior cosmesis and decreased invasiveness.
Introduction
Patients and Methods
The institutional review board approved this retrospective review. The study was conducted on patients undergoing ET at the Department of general surgery in Qilu Hospital of Shandong University in China from August 2001 to September 2010. A team comprising individuals experienced at laparoscopy and open thyroidectomy performed all ET's. Sex, age, tumor location, tumor size, type of operation, operative time, intraoperative blood loss, postoperative complications, pathology, time of hospitalization, postoperative pain evaluated by Visual Analog Scale (0–10) 24 hours and 48 hours after operation, and cosmetic result for each patient was recorded in a database. Patients with thyroid nodules were considered for ET if they had not undergone previous neck surgery, received radiotherapy, and had thyroiditis diagnosed by preoperative biochemistry. Patients with known cancer who had been operated on had a single tumor no larger than 2 cm, an age between 15 and 45 years, no evidence of lymph node metastases or extrathyroidal extension, and a nonaggressive histologic diagnosis. Welch's two-tailed t test compared means; whereas Fisher's two-tailed exact test compared proportions.
Surgical instruments included a 10 mm 30-degree fiber optic endoscope, 5 mm and 10 mm trocars, an ultrasonic scalpel (Johnson-Johnson Medical, Cincinnati, OH), a separating stick, 5 mm dissectors, scissors, an aspiration cannula, a 5 mm clip applicator, and hemostats. All ET's used general anesthesia with endotracheal intubation, and placed the patient supine with neck extended and chin midline.
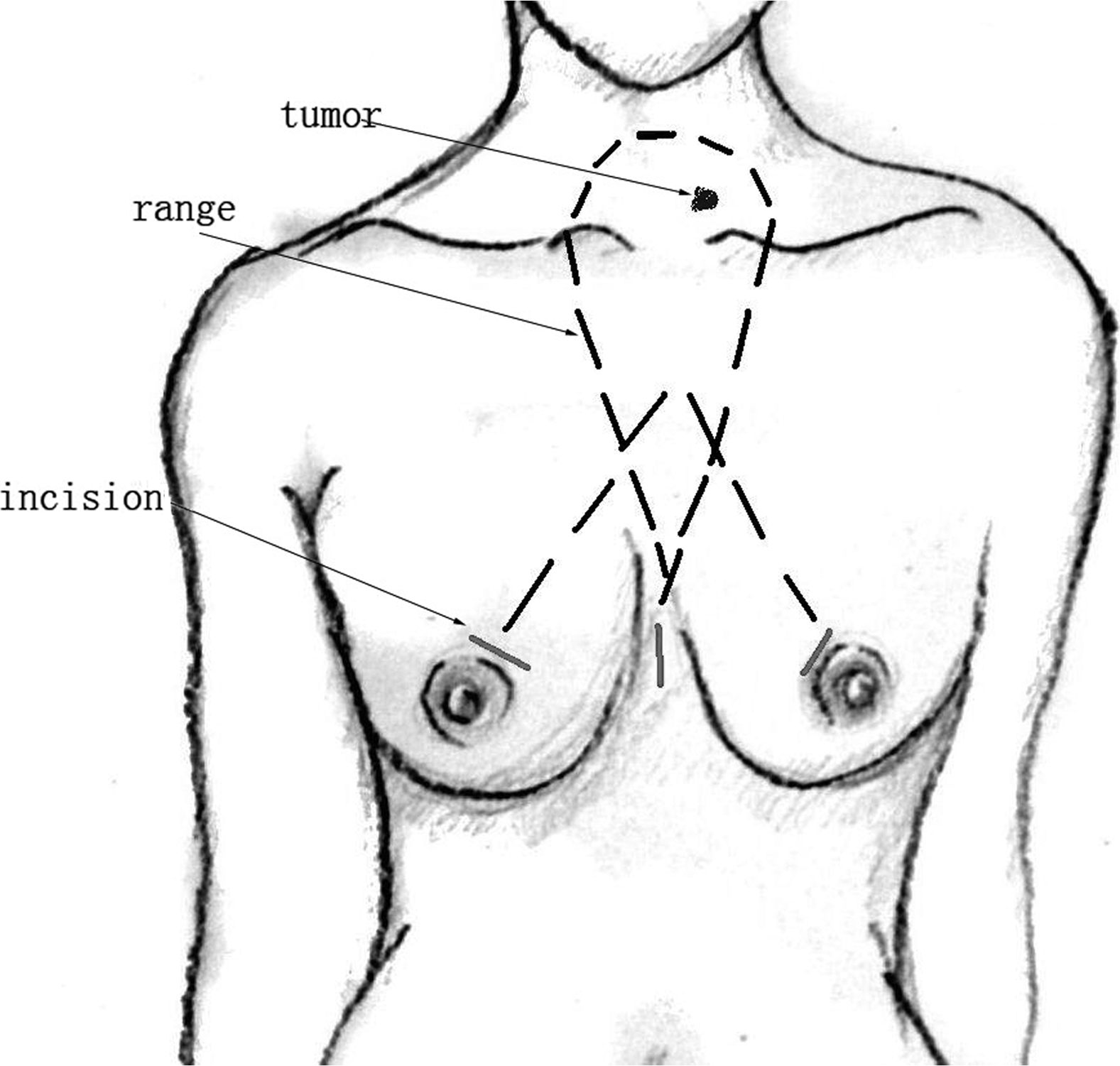
Two approaches were used. The modified anterior chest approach, previously described, 13 began with a 1 cm longitudinal incision one-fourth the distance from the xiphoid to the sternal notch. A separating stick performed a blunt dissection of the subcutis though this incision before the insertion of a 10 mm trocar. CO2 insufflations at a gas pressure of 6–8 mmHg maintained working space. A 10 mm 30° endoscope was then inserted. After bilateral transversal incisions had been created one-third the distance from the nipple to the sternoclavicular joint, 5 and 10 mm trocars were inserted under endoscopic guidance (incisions and routes described by Fig. 1). The ultrasonic scalpel dissected soft tissue until the working space reached the level of the thyroid cartilage cranially and to the medial edge of each of the sternocleidomastoid muscles laterally.

The incisions and dissection range of ET for modified anterior chest approach. ET, endoscopic thyroidectomy.
The breast approach was similar, except for (1) the location of the incision (Fig. 2), where a midpoint, longitudinal 1 cm incision was made at the nipple level, and (2) two additional skin incisions were made at the upper margin of mammary areolae, followed by the insertion of one 5-mm trocar and another 10 mm trocar through the incisions.
The incisions and dissection range of ET for breast approach.
Thyroidectomy was accomplished by first endoscopically dissecting the linea alba cervicalis before separating the ipsilateral strap muscles from the thyroid lobe. Retracting strap muscles laterally with two subcutaneous silk threads ensured adequate visualization. For subtotal thyroidectomy for Graves' disease or large thyroid lobes, strap muscles were partly transected along the thyroid, beginning at the lower pole of the thyroid gland, during which time, the inferior thyroid pedicle was identified, and the recurrent laryngeal nerve (RLN) was identified and protected. After ligating inferior and middle thyroid vessels, the lobe was inferiorly retracted to expose the superior thyroid arteries, which were dissected by the ultrasonic scalpel. The lobe was then superiorly excised from the inferior pole, with particular attention being paid to ensure sufficient distance of the heated ultrasonic scalpel from the RLN and visible parathyroids. Resected tissue was placed in a specimen bag that had been inserted via the 10-mm incision. The filled bag was removed via the middle or left 10 mm incision, which were enlarged as needed to accommodate larger specimens. Frozen section examination was then undertaken; if high-grade carcinoma was found, then cervicotomy and lymphadenectomy were performed; this operative procedure had been disclosed in the consent form and discussed with the patient preoperatively. After suturing transected strap muscles and linea alba cervicalis, a 5-mm suction drain was placed in the operative field and brought out through the 5 mm incision. The procedure concluded with subcutaneous suturing of incisions with absorbable thread and approximation of skin with adhesive tape.
Results
The 235 patients analyzed had a mean age of 34.5 years, with a range of 17 to 52 years. Of these patients, 11 (4.7%) were men, and 224 (95.3%) were women. The ultrasonographic nodule size was a mean 31.2 mm, with a range of 15–58 mm. Nodules were in the left lobe in 101 (43.0%), the right lobe in 93 (38.3%), the isthmus in 9 (3.8%), and bilaterally in 32 (13.6%) patients. Of these patients, 228 (97%) underwent ET, whereas 7 (3%) were converted to open thyroidectomy.
Of the 228 ET's, 145 (63.6%) were accomplished via the modified anterior chest approach; 83 (36.4%) via the breast approach. As displayed in Table 1, the modified anterior chest approach had better cosmesis and 2 mL less blood loss (P<.05), but the approaches did not differ in a fashion that could not be explained by chance. The twenty complications included five seromas, four cases each of cutaneous emphysema, anterior chest discomfort, and transient hypocalcemia, and three transient RLN palsies. No deaths ensued. Of the seven patients who required conversion to open thyroidectomy, five were likely inappropriate candidates, two with large tumors (>50 mm) and three with thyroiditis, who had poor visualization of the operative field; the remaining two patients showed on frozen section one case of poorly differentiated follicular carcinoma and one case of poorly differentiated papillary carcinoma.
VAS, visual analogue scale.
Discussion
Endoscopy has altered the face of surgery. Laparoscopic techniques have been used by our hospital in biliary tract and colorectal surgery for decades. The ET team had abundant experience with both conventional thyroidectomy and laparoscopic technique before this study had commenced; the results of this group are similar to those of other international centers with high volume.8,9 At our hospital, an intraoperative frozen section is performed, because fine-needle aspiration cytology has, for us, an unacceptably high false negative rate. 14
That ET has been proclaimed a “maximally invasive operation”8–11 may in part have hampered the use of this surgical procedure. Minimally invasive therapy, in general, aims at minimizing trauma while still achieving a satisfactory therapeutic result. 15 In the case of ET, it is the decreased aesthetic burden that is paramount; only one out of 228 (0.4%) had an unacceptable cosmetic result. Since pre-existing planes of dissection are used in ET, trauma is minimized6,16; levels of inflammatory factors (e.g., interleukin [IL]-6, IL-1β, tumor necrosis factor [TNF]-α, C-reactive protein (CRP), and immunoglobulin-G [IgG]) are lower for patients with ET than for those who undergo open thyroidectomy.17,18 Our patients have low visual analogue scale (VAS) scores without analgesic drugs. The low VAS scores and good cosmoses satisfaction prove ET to be a minimally invasive cosmetic procedure. Another point to be noted is a mean hospital stay of greater than 3 days, which let some people consider ET as a nonminimally invasive operation. In fact, the relatively long hospitalization is because inpatients' expense can be reimbursed, and outpatient thyroidectomy is very dangerous because of postoperative bleeding and asphyxia.
ET should not be used as a first-choice procedure for thyroid cancer until the technique is further refined, such that lymph nodes about the carotid sheath can be dissected. 12 For the current study, patients with cancer were carefully selected to avoid those with risk factors for metastatic disease or extrathyroidal extension; two patients with frozen sections that showed poorly differentiated carcinoma were converted to open procedures. This restriction permitted the performance of ET without cervical lymph node dissection. The most important issue is implantation of cancerous cells into the operative space; until such time as this issue is resolved, ET will largely be used for benign diseases and low risk cancers.
For adequate visualization of anatomical structures and proper instrument manipulation, a comfortable working space is vital. For our patients, this space was subcutaneously created via separating sticks or elastic separating pliers; it was maintained via CO2 insufflation, 6–8 mmHg, the recommended pressure. 19 When augmentation was required, either suture silk was used to pull infrahyoid muscles or, on occasion, muscles were transected.
Since the axillary approach requires a longer route to the operating space from the skin incision and was technically demanding and time consuming for bilateral lesions, 20 ET was performed at our institution via either the modified anterior chest approach or the breast approach, each being facile to master by surgeons in centers with low or medium surgical case loads. We modified the anterior chest approach by moving down the incisions with an intention to achieve satisfying cosmetic results while reducing physical invasion. This modified approach is suitable for Asians based on their own style of clothing and desired amount of skin exposure. As shown, it produces superior results cosmetically to those obtained via the breast approach.
The ultrasonic scalpel is preferred because of its known lower operative time, lower blood loss, better early cosmetic result, and reduced rate of conversion, factors that outweigh the slight increment in cost.21,22 Since the ultrasonic scalpel has been reported in ET to yield tracheal thermal injury and transient RLN paralysis, 23 dissection of the RLN should be undertaken with great care. 24 A study of ET in rabbits yielded a recommendation that, at a power level of 3, the activated ultrasonic scalpel tip be kept at least 2 mm away from the RLN, and the duration of any incision be kept at or below 3 seconds. 25 For our patients, functional US blades were turned upward and kept at least 5 mm away from the RLN, parathyroid gland, and trachea. Incision times were maximally decreased, in part by adopting fractionation during coagulation. No immediate RLN or tracheal injury developed, but three cases of delayed, transient RLN palsy developed, most likely because of soft tissue edema.
The ET is easily mastered by learners facile at laparoscopy and conventional thyroidectomy. Both the modified anterior chest and breast approaches are suitable, although the former yields more satisfactory cosmesis. In fact, ET should be considered not only cosmetic, but also minimally invasive.
Footnotes
Disclosure Statement
No competing financial interests exist.