
Abstract
Abstract
Aim:
The purpose of this study was to evaluate the effect of saline washout under the diaphragm on postoperative shoulder tip pain (STP) and β-endorphin (βE) levels in patients who had undergone laparoscopic cholecystectomy (LC).
Methods:
Between December 2010 and March 2011, 50 patients requiring cholecystectomy for benign gallbladder disease were enrolled in this study. Twenty-five patients (Group 1) underwent LC without saline irrigation, whereas the other 25 were operated on with saline irrigation (30 mL/kg) under the diaphragm (Group 2). Plasma levels of βE were measured before and after the operation. The degree of STP following LC was assessed using a visual analog pain scale (VAS) at 6, 12, and 24 hours postoperatively.
Results:
Eight patients in Group 1 (32.0%) and seven patients in Group 2 (28.0%) complained of STP. There was no significant difference between the two groups in operation time, postoperative hospital length, postoperative βE, dose of analgesics, or VAS at 6, 12, and 24 hours after surgery. The intensity of abdominal pain (AP) was significantly higher than that of STP. Significantly elevated levels (11.3±5.1 pg/mL) of βE were observed postoperatively when compared with preoperative levels (9.7±5.2 pg/mL) (P=.02).
Conclusions:
Normal saline irrigation under the diaphragm does not reduce postoperative STP after LC. Ancillary techniques to reduce AP and STP should be considered.
Introduction
There are several methods for quantifying the severity of postoperative pain. A visual analog pain scale (VAS) is a simple and widely accepted method for assessing postoperative pain in most hospitals. β-Endorphin (βE), an endogenous opioid derived from proopiomelanocortin, is a neurohormone secreted by the pituitary gland. Although the role of plasma βE in responses to pain is unclear, plasma βE levels have been reported to correlate with severity of postoperative pain. 13
In addition to subjective assessment of VAS and objective measurement of plasma βE, the purpose of this study was to evaluate the benefit of normal saline washout under the diaphragm for alleviating the incidence and severity of postoperative STP after LC.
Materials and Methods
Patients
A 40% absolute reduction in STP was considered clinically relevant; it required approximately 22 patients in each arm, with 80% power at the 5% significance level. Therefore, we planned to enroll approximately 25 patients in each group.
This study was approved (Number HYUH IRB 2010-R-08) by the institutional review board of Hanyang University Hospital, Seoul, Korea. Informed consent was obtained from all participants before inclusion in the study. From November 2010 to March 2011, 75 patients were admitted to our hospital for treatment of cholelithiasis. Of these patients, 25 patients were excluded. The criteria for exclusion were as follows: an American Society of Anesthesiology physical status of 3 or more, planned emergency LC, acute calculous cholecystitis, age below 20 years or above 70 years, previous extensive abdominal surgery, and disease causing shoulder pain for other reasons. Altogether, 50 patients with chronic calculous cholecystitis to be treated by cholecystectomy were enrolled in the study.
The patients were randomized blindly into two groups based on computer-generated numbers. Group 1 underwent laparoscopic cholecystectomy without normal saline washout; Group 2 were given normal saline irrigation under the diaphragm.
Surgical procedure
All the procedures were performed by one experienced hepatobiliary surgeon. The standard four-port technique was used. Two venous blood samples (3 mL) for measuring βE levels were drawn from the antecubital vein immediately after induction of anesthesia and at the end of the operation.
All surgery was performed with the patient under general anesthesia, and, for premedication, all patients received intramuscular midazolam (2.5 mg) and atropine sulfate (0.5 mg) half an hour before induction of anesthesia. Anesthesia was with 1 mg/kg lidocaine, 1.5 mg/kg propofol, and 0.6 mg/kg of rocuronium and was maintained with sevoflurane (1.8%–2.2% vol/vol) and remifentanil (0.05–0.1 μg/kg/minute).
The pneumoperitoneum was established by the open access (Hasson) technique with blunt-tipped 12-mm trocars in both groups. The insufflation pressure was set at 12 mm Hg, and the patients were placed in the reverse Trendelenberg position after insertion of the four ports. In Group 2, the space between the right diaphragm and liver was washed out by a 3-minute irrigation with normal saline (30 mL/kg, 1953.7±333.8 mL) at the end of the surgery followed by immediate removal of the saline.
Assessment of pain
Each patient was instructed to describe the severity of STP and abdominal pain (AP) just after awakening from anesthesia, and the intensities of STP and AP were assessed with self-report questionnaires using a VAS from 0 to 10 at 6, 12, and 24 hours after surgery. No routine postoperative analgesics were administered; they were only given when requested by patients and consisted of 30 mg of intravenous ketorolac or 100 mg of intravenous diclofenac. The numbers of patients who complained of STP were recorded.
Plasma levels of βE were estimated with a commercially available radioimmunoassay kit following the standard published procedure (Phoenix Pharmaceuticals, Inc., USA). The detection limit was 5 pg/mL. All the data were recorded directly into a dedicated spreadsheet (Microsoft Excel 2007).
Results
Patients' characteristics
The characteristics of the patients in the two groups were similar in terms of age, sex, and body mass index. There were no differences in duration of operation and length of postoperative hospital stay, and no intraoperative bile spillage occurred in any patient (Table 1).
Data are mean±standard deviation values.
None of the differences between the groups was significant by the unpaired t test.
BMI, body mass index.
Postoperative pain
Postoperative STP occurred during the first 24 hours after surgery in 15 patients: 8 (32%) in Group 1 and 7 (28%) in Group 2. The mean postoperative STP scores of the 50 patients were 3.0, 2.3, and 1.0 at 6, 12, and 24 hours, respectively. There were no significant differences in severity of STP between the two groups (Fig. 1). AP was significantly more intense than STP in both groups at all three times after surgery (Fig. 2). The intensity of STP gradually decreased and declined enough to make it unnecessary for analgesics to be given to all the patients.
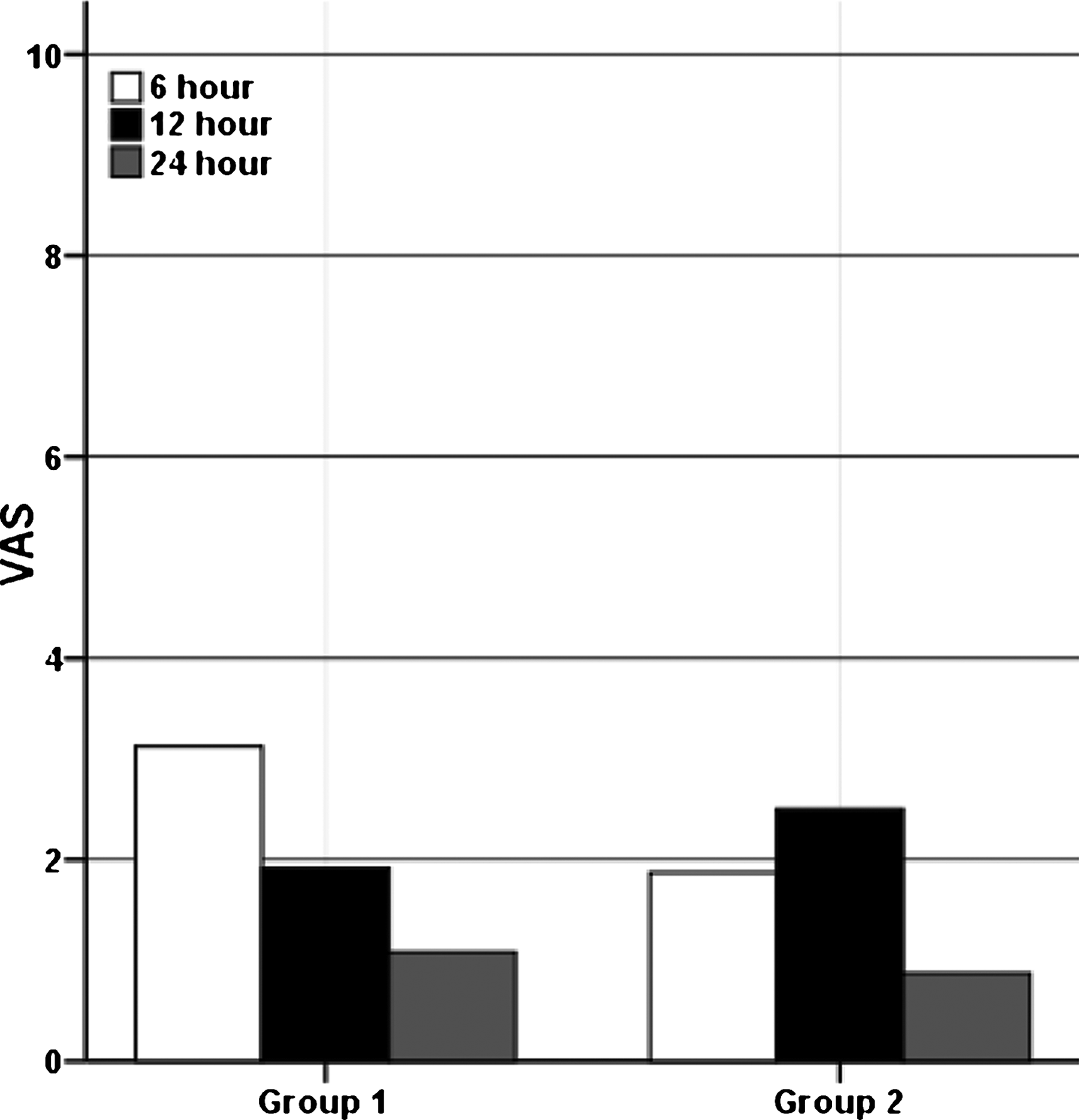
Visual analog pain scales (VAS) for shoulder tip pain at 6, 12, and 24 hours after laparoscopic cholecystectomy. There was no significnat difference between Groups 1 and 2 at 6, 12, or 24 hours after laparoscopic cholecystectomy by unpaired t test.
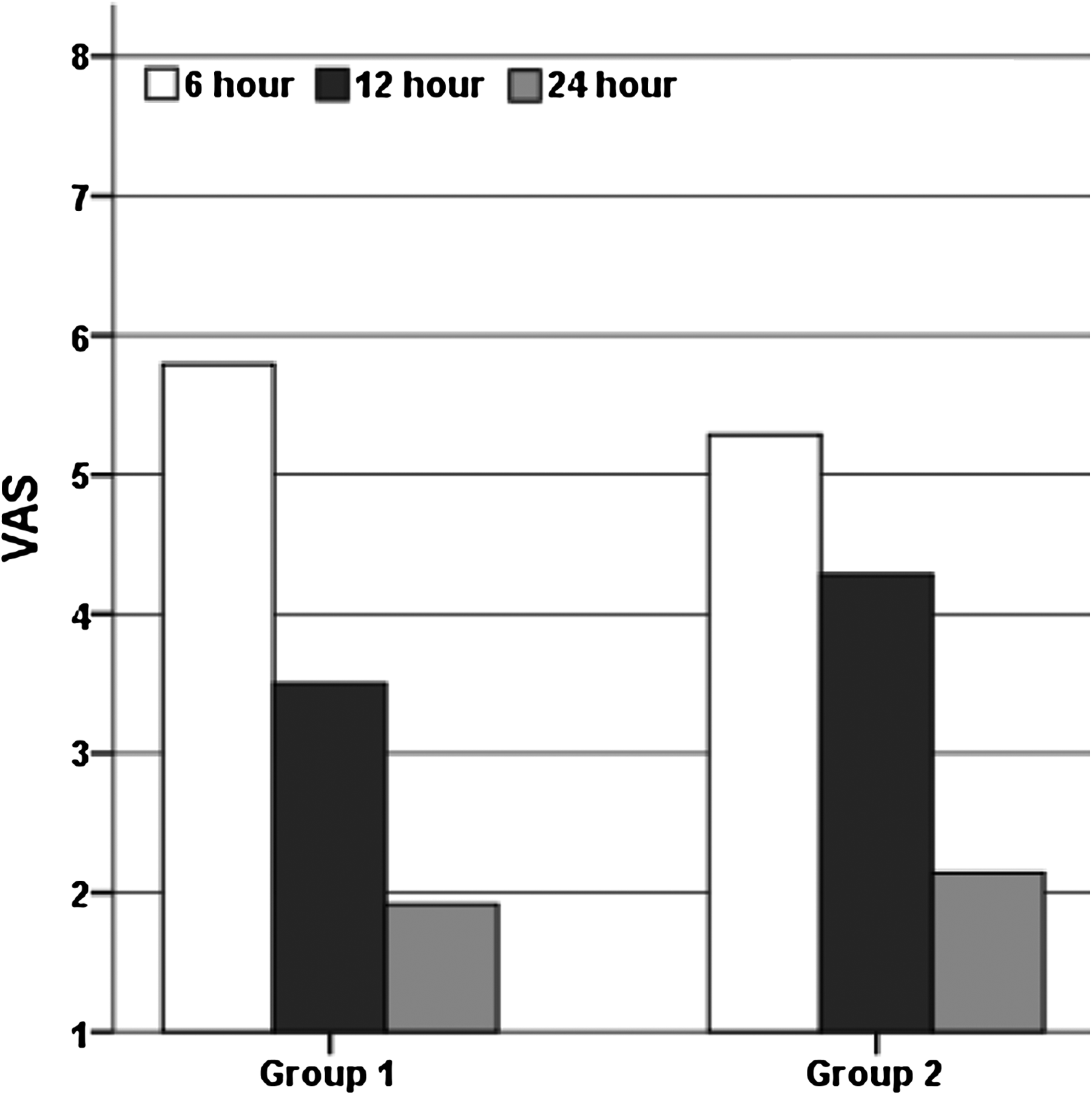
VAS for abdominal pain at 6, 12, and 24 hours after laparoscopic cholecystectomy. There was no significant difference between Groups 1 and 2 at 6, 12, or 24 hours after laparoscopic cholecystectomy by unpaired t test.
However, analgesics were administered to 20 patients: 11 in Group 1 and 9 in Group 2. The mean amounts of analgesics required by Groups 1 and 2 were 57 mg and 59 mg, respectively (not significantly different).
Measurements of βE levels
As shown in Figure 3, postoperative levels of βE were moderately higher than preoperative levels (11.3±5.1 pg/mL versus 9.7±5.2 pg/ml, P=.02) (range, 10–1280 pg/mL), with no significant difference between the groups (11.5±4.0 pg/mL and 11.2±6.0 pg/mL versus 9.3±5.3 pg/mL and 10.1±5.1 pg/mL, respectively). Apart from postoperative pain, there were no major intraoperative or postoperative complications that affected the length of hospital stay in either group.
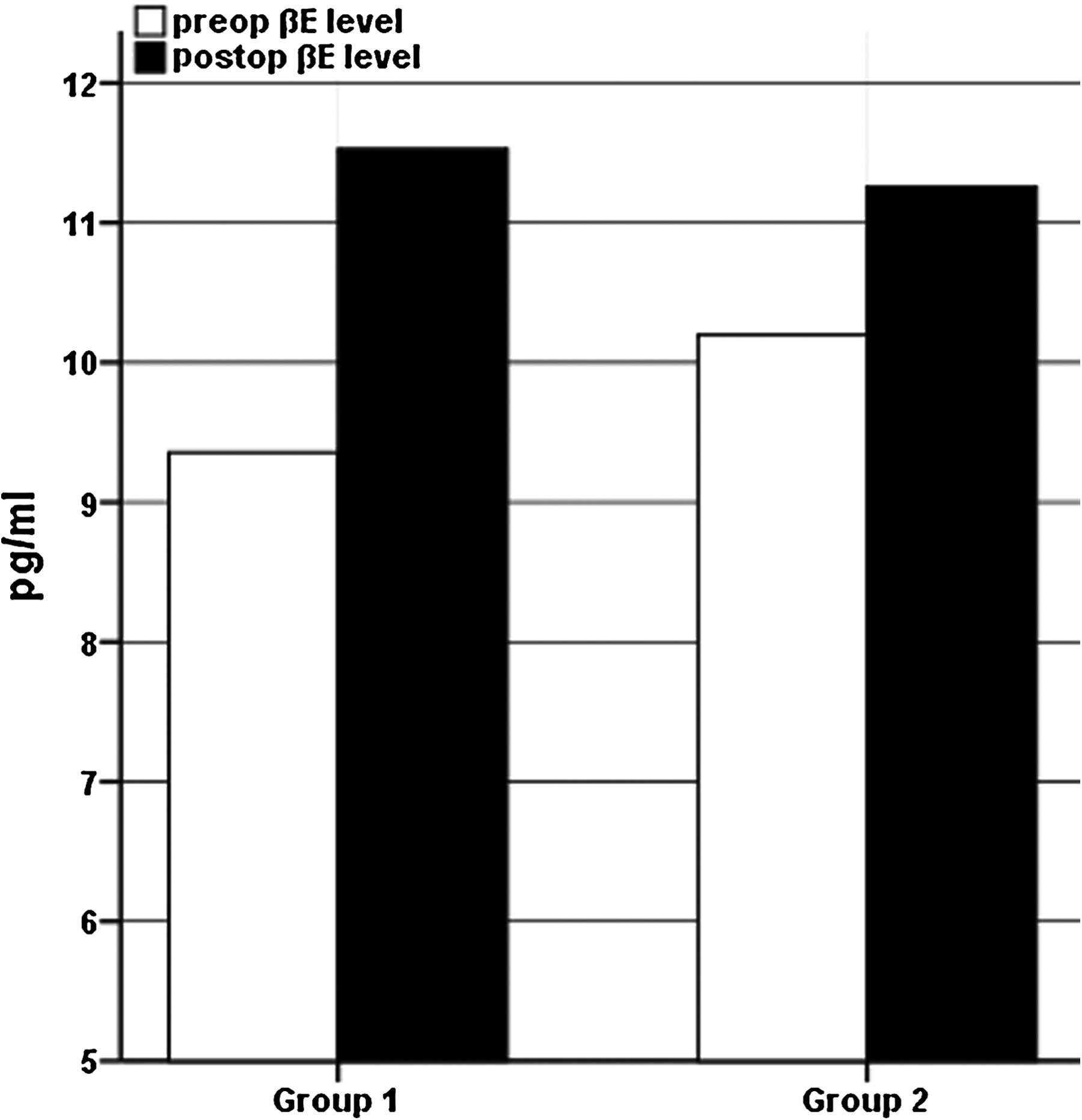
Preoperative (preop) and postoperative (postop) β-endorphin (βE) levels in the two groups. There was a statistically significant difference by paired t test between preop and postop βE levels.
Discussion
Laparoscopic surgery has become increasingly popular and has led to an enormous change in general surgery in the past decade. Less pain and early recovery are the benefits of this approach that prompt the move to laparoscopic surgery. However, even though postoperative pain is reduced it still exists. STP is a common complaint after laparoscopic surgery, although its incidence varies. Approximately one-third of patients who undergo LC suffer from STP following surgery. 7 Researchers have attempted to reduce STP by altering intraperitoneal pressure,6,7 intraperitoneal instillation of local anesthetics,3,4 or saline application.2,5,14 Saline washout is thought to be a simple, economical approach and therefore to be potentially useful for reducing STP after LC. The clinical trial reported that the local acidosis in the peritoneal cavity may be diluted and thus attenuated, leading to a reduction of STP, by intraperitoneal normal saline infusion combined with suction and drain insertion. 8 However, there are few reports demonstrating the clinical efficacy of saline in alleviating STP after laparoscopic surgery without additional methods.
βE is an endogenous opioid that has been shown to be 18–33 times more potent than morphine in reducing stress and pain. 15 Patients undergoing surgery have elevated concentrations of plasma βE, and plasma βE levels are positively correlated with severity of postoperative pain. 13 Moreover, it has been reported that intraoperative βE levels are inversely correlated with the dose of analgesic required postoperatively. 16 In this study, we found that postoperative plasma βE levels were significantly higher than before surgery. However, in a correlation analysis we found no clinical variables that were significantly correlated with the increase of plasma βE level.
STP after laparoscopy is due to many causes. CO2 gas remaining within the peritoneal cavity frequently irritates the peritoneum and causes visceral pain.10,11 Carbonic acid is thought to be a peritoneal irritant and to induce acidosis after CO2 pneumoperitoneum. 12 A delay in the effect of drainage and of the remaining saline on the extent of acidosis of the peritoneal cavity appears to be a contributing factor. However, in our study we found no significant reduction in STP in the patients who underwent saline irrigation under the diaphragm compared with the controls. Thus, the benefit of saline irrigation on reduction of postoperative STP in terms of plasma βE levels and VAS remains uncertain. However, we did not submerge the liver with normal saline and left the saline to drain from the peritoneal cavity after aspiration because we considered that draining can lead to irritation of the peritoneum, which is a major cause of postoperative pain. Given the different methods used in our study, we consider that the effect of the delay in drainage of the peritoneal cavity on dilution of the local metabolic acidosis is more important than any direct benefit of saline irrigation in reducing STP.
A limitation of this study was that we were unable to compare the long-lasting effects on STP in the two groups because most of the patients were discharged 1 or 2 days after operation in the absence of serious complications. However, the occurrence of early discharge may imply that few if any patients experienced a high level of STP.
From this study, we conclude that normal saline irrigation under the diaphragm is on its own not sufficient to decrease the incidence and severity of STP and that AP is more severe than STP in patients undergoing LC. Therefore there is a need to develop new techniques to alleviate STP and AP.
Footnotes
Acknowledgments
This work was supported by the research fund of Hanyang University (HY-201000000000224-N). We thank Adam Turner for the help with the English language.
Disclosure Statement
No competing financial interests exist.