
Abstract
Abstract
Background and Aims:
Patients with a dilated common bile duct (CBD) and multiple, primary, or recurrent stones are candidates for choledochoduodenostomy. This article reviews our technique and results of laparoscopic choledochoduodenostomy (LCDD) in patients with CBD stones.
Subjects and Methods:
Prospectively maintained data of patients with a dilated CBD and multiple, primary, or recurrent CBD stones who underwent LCDD after laparoscopic CBD exploration (LCBDE) at a tertiary-care teaching hospital in New Delhi, India, during a 10-year period from April 2001 to March 2011 were analyzed.
Results:
During this period, of 195 patients who underwent LCBDE for CBD stones, 27 patients underwent LCDD. The mean age of patients was 45.7±13.5 years. There were 6 male and 21 female patients. Sixteen (59.2%) patients had jaundice at presentation. Average CBD diameter was 19.6±4.4 mm. On average, 11.5±15.7 stones were removed from the CBD. Mean operative time was 156.3±25.4 minutes. Mean operative blood loss was 143.3±85.5 mL. Average postoperative hospital stay was 6.4±3.8 days. CBD clearance was obtained in all cases. One patient had a bile leak that resolved with conservative treatment. There was no mortality. No patient has had recurrence of symptoms or cholangitis after a follow-up of up to 9 years.
Conclusion:
LCDD can be safely performed in patients with a large stone burden and recurrent or primary CBD stones. Although it requires advanced laparoscopic skills, the benefits of a single-stage laparoscopic procedure can be extended to these patients safely with good results.
Introduction
Subjects and Methods
This study was conducted at a tertiary-care teaching hospital in New Delhi, India. Patients with symptomatic gallstone disease with suspicion of CBD stones based on history of pancreatitis or jaundice, raised alkaline phosphatase activity, and dilated CBD with or without CBD stones on ultrasound were evaluated with magnetic resonance cholangiopancreatography (MRCP). Patients with evidence of CBD stones on MRCP were selected for LCBDE. Patients presenting with cholangitis were managed conservatively with intravenous fluids and antibiotics and taken up for surgery after resolution of cholangitis. Patients with preoperative or intraoperative findings of a dilated CBD (>15 mm) with multiple stones, recurrent stones, or primary CBD stones underwent laparoscopic CBD clearance and LCDD.
A single primary surgeon (the first author) operated all the cases. Antibiotic prophylaxis given at induction included intravenous ceftriaxone (1 g) and metronidazole (500 mg). All patients underwent LCBDE via a choledochotomy under general anesthesia.
Operative technique
Access was obtained with five ports as described previously for LCBDE: 6 a 10-mm umbilical port for the telescope and insufflation, a 12-mm working port in the epigastrium slightly to the left of midline; two 5-mm ports, one in the midclavicular line 5–7 cm below the costal margin and another in the right anterior axillary line; and another 5-mm port inserted at the highest point in the epigastrium in the right paramedian position.
All patients underwent CBD exploration through a longitudinal choledochotomy in the immediate supraduodenal part of the anterior wall of the CBD. Stone clearance was obtained by various methods including use of Dormia baskets, Fogarty catheters, and flushing as described previously. 6 Stones impacted at the lower end of the CBD were fragmented with a Holmium laser, and the fragments were either extracted with the Dormia basket or flushed into the duodenum. Intraoperatively choledochoscopy was done in all patients to guide stone removal and to ensure complete CBD clearance as described previously. 6
After complete CBD clearance was ensured, the choledochotomy incision was extended (if not already done for stone extraction) for about 1.5 cm or more longitudinally. A longitudinal incision was made in the anterior wall of the first part of the duodenum close to and centered on the lower end of the choledochotomy as described for the open technique. The size of the duodenotomy was tailored to the size of the choledochotomy and was usually around 1.5–2 cm. The choledochoduodenostomy was fashioned to achieve a “diamond-shaped anastomosis” as in the open technique. First, a suture (3-0 Vicryl, Ethicon, Inc., Johnson & Johnson, Somerville, NJ) was used to approximate the lower end of the choledochotomy with the superior cut edge of the duodenotomy at its midpoint. This was followed by interrupted sutures, one on either side of the first suture. Interrupted sutures were then taken alternately toward the left and right side, one by one, to complete the posterior wall of the anastomosis (Fig. 1).
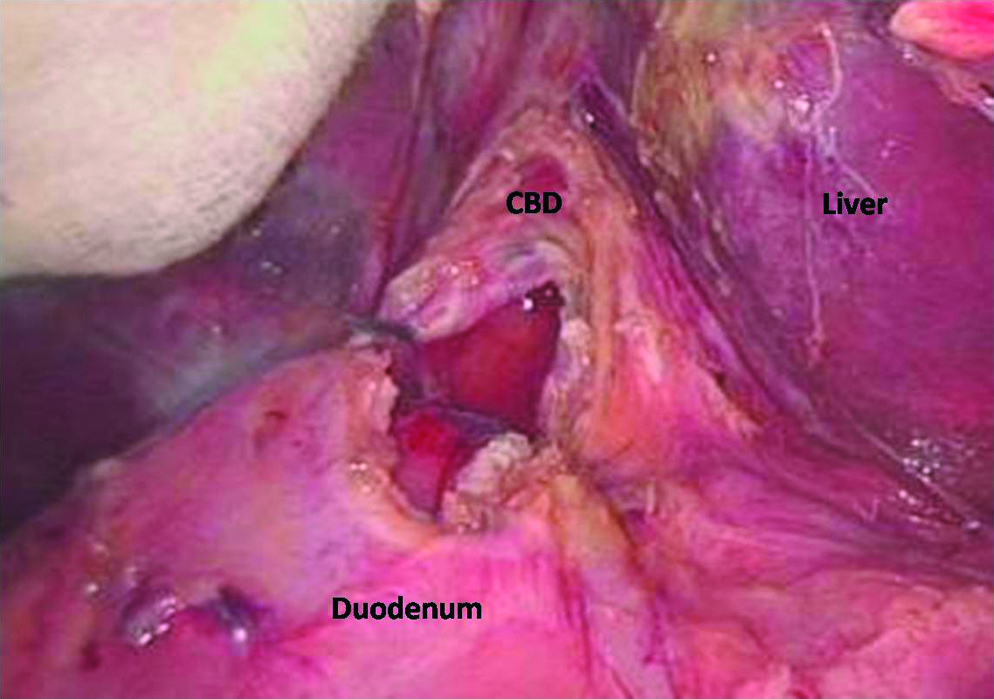
Posterior layer of the choledochoduodenostomy completed with interrupted sutures. CBD, common bile duct.
During the initial experience, this was continued further to complete the anterior wall of the anastomosis with interrupted sutures. Later in the series, two modifications were done. After completion of the posterior wall, the corner sutures of this wall were held as long stay sutures to lift the corners. This ensured that there was no gap at the corners, thereby achieving a watertight anastomosis (Fig. 2). The other modification was to suture the anterior wall with continuous sutures from the right to left side (Figs. 3 and 4).
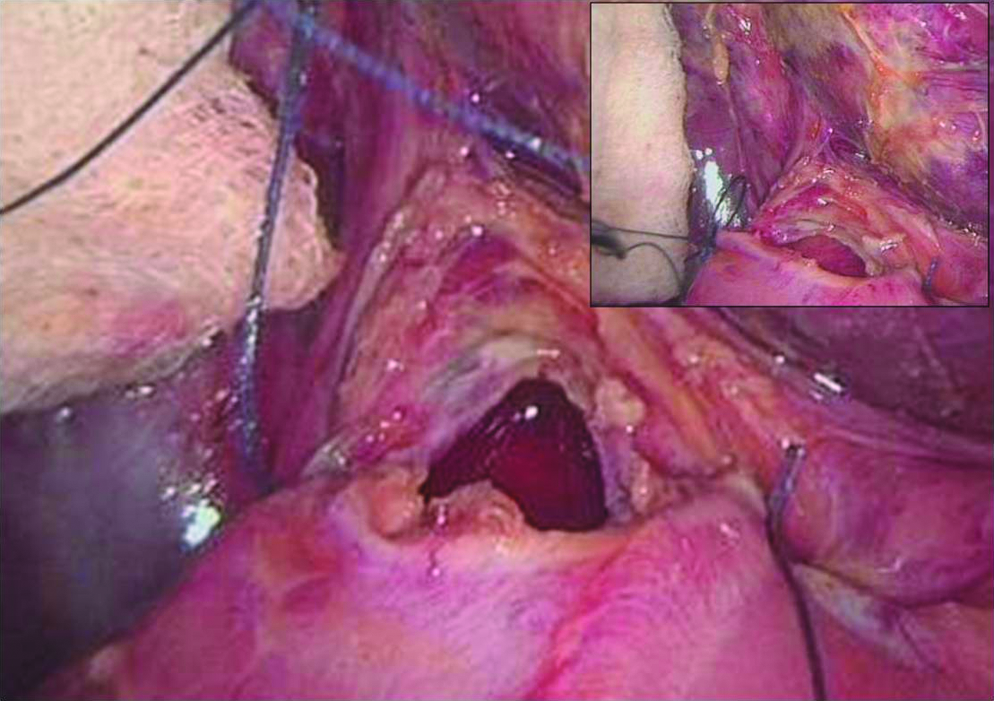
Stay sutures at the corners of the choledochoduodenostomy.

Continuous sutures in the anterior layer of the choledochoduodenostomy. CBD, common bile duct.

Anterior layer of the choledochoduodenostomy nearing completion.
A subhepatic drain was routinely placed in all patients. Patients were allowed oral intake after 48 hours. Oral intake was increased as tolerated. Antibiotics were discontinued after 48 hours unless clinically indicated. Drains were removed if the drainage was nonbilious and minimal. Patients were discharged after drain removal.
Data for these patients were maintained prospectively in a database and analyzed retrospectively.
Results
From January 2001 to April 2011, a total of 195 patients underwent LCBDE. Of these, 6 patients required conversion to open surgery for various reasons. Twenty-seven patients who underwent LCDD after successful CBD clearance were included for this study. Mean age of patients was 45.7±13.5 years (range, 19–70 years). There were 6 male and 21 female patients. Sixteen (59.2%) patients had jaundice at presentation. Four of these patients had a previous cholecystectomy more than 5 years ago. Endoscopic stone removal had been attempted in 5 patients prior to referral to us but had failed to clear the stones. The mean bilirubin levels were 5.1±5.9 mg/dL (range, 0.4–18.2 mg/dL). The average CBD diameter on preoperative MRCP was 19.6±4.4 mm (range, 15–32 mm). Stones as large as 30 mm were removed by laparoscopic approach without conversion. The mean number of stones removed from CBD was 11.5±15.7 (range, 1–69). CBD clearance was obtained in all cases. Mean operative time was 156.3±25.4 minutes (range, 90–190 minutes). Operative blood loss was 143.3±85.5 mL (range, 50–500 mL). The average postoperative stay was 6.4±3.8 days (range, 4–21 days). One patient developed bile leak as manifest in the drain that resolved with conservative treatment. There was no mortality in this series. Postoperative follow-up ranged from 2 months to 9 years. None of these patients have had any recurrence of symptoms or cholangitis.
Discussion
LCBDE is a safe single-stage treatment for CBD stones. Recurrence of CBD stones after endoscopic or surgical removal is not uncommon. Choledochoduodenostomy is an excellent technique for prevention of stone recurrence and has been extensively evaluated for management of such patients in the past. Extension of laparoscopy to management of such patients requires advanced laparoscopic skills for ensuring CBD clearance and performing the choledochoduodenostomy.
Biliary stone disease is more common in females. This is reflected in the results of this study as well as our previously published series of LCBDE. 6 The majority of patients with CBD stones undergo multiple sessions of endotherapy, with surgical referral being sought mainly for endotherapy failures or recurrence after successful treatment. Preoperative endoscopic retrograde cholangiopancreatography (ERCP) is also used for providing a road map for surgery.2,3,7 Five of our patients had been referred to us after a failed ERCP. We feel that sufficient information regarding biliary anatomy can be provided noninvasively by MRCP. Considering the risk of infection and bleeding, we prefer to avoid ERCP in patients with CBD stones unless mandated by unremitting cholangitis for biliary drainage. More than half of the patients in this series had jaundice at presentation. None of these patients required preoperative biliary drainage. We believe that patients with jaundice in the absence of unremitting cholangitis can be taken up for LCBDE safely without preoperative biliary drainage irrespective of the serum bilirubin levels.
Dilatation of CBD is a prerequisite for a safe choledochoduodenostomy. The dilatation helps to ensure an adequate-sized anastomosis with resultant reduction in postoperative long-term problems, including sump syndrome. We consider choledochoduodenostomy only in patients with a CBD diameter >15 mm as is also reported in other series of choledochoduodenostomy.1,3
Roux-en Y hepaticojejunostomy has also been tried laparoscopically for management of this condition. 2 However, LCDD for recurrent CBD stones is technically simpler than a choledochojejunostomy. It does not divert bile from the duodenum. In addition, there is no alteration in jejunal anatomy in a choledochoduodenostomy. Even though LCDD has also been described for bypass of malignant bile duct obstruction,1,2 we generally prefer a choledochojejunostomy in such cases for fear of recurrent biliary obstruction due to extension of disease to the anastomotic site. None of the patients in this series underwent choledochoduodenostomy for bypass for malignant biliary obstruction.
Bile leak occurred in one patient as evident in the peroperatively placed drain. This patient was an elderly diabetic woman with cholangitis that had resolved with preoperative antibiotics. She had a prolonged hospital stay (21 days) following which the bile leak resolved without any intervention. There was no mortality in this series. The results of our series compare favorably with the results of other reported series in the literature.1–3
Regarding the operative technique of LCDD, the initial report by Tinoco et al. 1 suggested use of a transverse choledochotomy. Subsequent reports have stressed the use of a longitudinal choledochotomy.2,3 Literature on open choledochoduodenostomy has emphasized the virtues of a “diamond-shaped choledochoduodenostomy.” We believe that a laparoscopic procedure should be a replication of the open procedure. Our technique of taking sutures alternately on the right and left side starting from the midline posteriorly ensures a watertight closure of the posterior layer. Reflecting back on the bile leak that occurred in our initial experience, we felt that cutting all sutures short could possibly lead to a gap in the anastomosis at the corners. After completion of the posterior layer, keeping the long corner stay sutures facilitates placement of subsequent sutures, also ensuring that there would be no excess gap at the corners as in the open technique. This is confirmed by our subsequent experience where we have not had bile leak in any other patient. Later in this series, with increasing expertise, we have used continuous sutures to complete the anterior wall of the choledochoduodenostomy safely.
To our knowledge, this is the largest experience of LCDD in patients with biliary stone disease. Despite meticulous attention and choledochoscopy, there is always a risk of residual stones in patients with multiple and/or primary stones. As reported by us previously, our patient population has a higher stone burden and intrahepatic stones with associated biliary dilatation; patients neglect their symptoms and present only after repeated episodes of cholangitis. 6 This, combined with a relatively higher incidence of recurrent pyogenic cholangitis in this part of the world, explains the relatively high proportion of our patients (12.8% of all patients undergoing LCBDE) requiring a choledochoduodenostomy for biliary drainage after LCBDE.
Conclusions
Choledochoduodenostomy is indicated in patients with large stone burden, recurrent stones, and primary CBD stones and in patients with incomplete CBD clearance. Although it requires advanced laparoscopic skills, the benefits of a single-stage laparoscopic procedure can be safely extended to this patient population with good results.
Footnotes
Acknowledgments
This work was funded by the Department of Surgery, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India.
Disclosures
No competing financial interests exist.