
Abstract
Abstract
Introduction:
Laparoscopic adrenalectomy has become the standard of care for the surgical treatment of benign adrenal pathology. We present the following case series documenting our experience in refinement of this approach.
Paients and Methods:
Analysis of patient records identified those in whom laparoscopic adrenalectomy was performed from January 1997 through February 2010. Study variables included indications, operative time, blood loss, length of hospital stay, histopathological evaluation, and complications.
Results:
Laparoscopic adrenalectomy was performed in 306 patients using the transperitoneal lateral approach. No major operative complications were noted, and postoperative complications included a pulmonary embolism and 2 cases of pneumonia. Conversion to the open approach was necessitated in two cases. The median operative time was 95±29 minutes (range, 45–145 minutes). Estimated blood loss was 60 mL (range, 30–150 mL). The mean size of the removed gland was 5.9±1.6 cm (range, 3–13 cm). The mean size of the tumor was 5±2 cm (range, 0.5–12 cm). The median hospitalization was 4±3.7 days (range, 2–22 days). Adrenal pathology included adenoma (n=164), pheochromocytoma (n=79), hyperplasia (n=35), metastatic carcinoma (n=22), cyst (n=9), myelolipoma (n=9), hemangioma (n=3), ganglioneuroma (n=3), and melanoma (n=2).
Conclusion:
Laparoscopic adrenalectomy is a safe and feasible approach to adrenal pathology, providing the patients with all the benefits of minimally invasive surgery.
Introduction
Patients and Methods
We performed a retrospective analysis of health records for patients who were operated on at University Hospital Center Zagreb, Zagreb, Croatia, from January 1997 through February 2010. In this period 306 consecutive patients underwent planned LA.
Diagnosis of adrenal tumors was based on computed tomography scans and/or magnetic resonance imaging. The indications for LA were, according to Croatian guidelines, 5 adrenal incidentalomas larger than 4 cm in diameter, functional tumors (pheochromocytoma, aldosteronoma, Cushing's syndrome, or sex hormone–producing tumor), and solitary adrenal metastases. The diagnosis of Cushing's syndrome was based on characteristic clinical presentation and the results of hormonal criteria: increased urinary free cortisol level, low adrenocorticotropic hormone level, and nonsuppressibility of cortisol secretion in the 1-mg overnight dexamethasone test. The diagnosis of aldosteronoma was based on an elevated plasma aldosterone/plasma renin activity ratio (≥30) and nonsuppressibility of aldosterone in the saline infusion test. Pheochromocytoma was diagnosed by biochemical evidence of catecholamine overproduction and 131I-metaiodobenzylguanidine scintigraphy. Patients with pheochromocytoma were preoperatively prepared using α-receptor blockers. For patients with tachycardia, β-receptor blockers were added in addition to α-receptor blockers.
In all cases, we exclusively used the laparoscopic transperitoneal lateral approach. We have gathered the most experience using this approach. It allows inspection of the abdominal cavity by providing a favorable transabdominal view, and gravity aids in further visualization of the adrenal gland. In brief, the patient is placed with the ipsilateral side elevated 45–60° from the operating table, which is then slightly flexed below the patient's umbilicus. A Veress needle is generally used to establish pneumoperitoneum. For left adrenalectomies, we used three or four trocars, and for right adrenalectomies, four trocars. In cases of bilateral adrenalectomy, we first performed right-sided LA, followed by repositioning of the patient and proceeding to left-sided LA.
The splenic flexure, descending colon, spleen, and tail of the pancreas are mobilized on the left side. On the right side, the right lobe of the liver is mobilized to expose the inferior vena cava, and the triangular ligament is divided before placement of a liver retractor. The dissection is performed by use of bipolar cautery and an ultrasonic dissector to divide the tissue sharply. In all cases except pheochromocytoma, we dissect the adrenal gland, together with surrounding fat tissue, first laterally, superiorly, and then posteriorly, thereby lifting the gland off the muscle and clearly exposing the vein as it drains into either the renal vein on the left or the inferior vena cava on the right side. The vein is double clipped and divided after the gland is almost completely dissected. This approach minimizes bleeding from adrenal gland, which can occur if we first clip the vein.
All tumors were removed using laparoscopic retrieval bags (Memo Bag, 200 mL or 800 mL, Rüsch, Teleflex Medical). Depending on the size of the tumor we extended one incision, usually at the place of camera. All patients had a drain until drainage was less than 100 mL, with removal on the second postoperative day in most cases.
All patients were assessed for the following variables: preoperative diagnosis, histopathology, operative time, blood loss, complications, conversion to open surgery, and hospital stay.
Results
During the study period 306 patients underwent LA with 326 adrenal glands removed. The demographics of the patients are shown in Table 1. In this series we performed 146 left, 125 right, and 20 bilateral LAs. Additionally, in 6 patients we performed partial LA, including one patient who presented with bilateral metastasis of renal cell carcinoma, and only partial adrenalectomy was performed on the left side. Nine patients had fenestration of a cyst of the adrenal gland.
The median operative time was 95±29 minutes (range, 45–145 minutes). Estimated blood loss was 60 mL (range, 30–150 mL) and did not necessitate transfusion for any patient. The mean size of the removed gland was 5.9±1.6 cm (range, 3–13 cm). The mean size of the tumor was 5±2 cm (range, 0.5–12 cm) (Table 2).
Operative time for unilateral laparoscopic adrenalectomy was considered.
The number of complications was minimal and included one pulmonary embolus (Clavien IIIa) and two cases of pneumonia (Clavien II). 6 One patient 9 years after LA for histopathologically confirmed benign pheochromocytoma had a recurrence. There were no deaths and no injury to surrounding organs. There were two conversions, which included the 11th and 47th patient. Both conversions were due to extensive intraabdominal adhesions. Twenty patients presented with metastasis to the adrenal glands, including two patients in whom bilateral adrenalectomy was performed because of metachronous metastasis of renal cell carcinoma.
The median hospitalization was 4±3.4 days (range, 2–22 days). Patients who had a bilateral adrenalectomy had a longer hospital stay (median, 6±4.5 days; range, 2–22 days) than those who had a unilateral operation (median, 4±3.3 days; range, 2–21 days) (P=.004).
Results of the histopathological evaluation are listed in Table 3.
Including functional and nonfunctional adenomas.
Discussion
LA has replaced the open surgical approach over the last decade. This is corroborated by the large number of articles that have proven it a safe and effective procedure with minimal complications.7,8
These lower complication rates include less operative blood loss and thus less need for transfusion during the procedure. Pleasing outcomes also include less postoperative pain, earlier return to activity and diet, and better cosmetic results. All these benefits combine to produce a shorter hospital stay and lower overall costs.8,9
Indications for operations in this study were similar to those in published series, in which most of the operations were performed for aldosteronomas, glucocorticoid excess, pheochromocytomas, and incidentalomas.10,11
With overwhelming evidence solidifying LA as the procedure of choice for benign adrenal lesions and masses smaller than 6 cm, the focus of discussion in recent times has shifted towards its application in larger tumors12,13 and those more likely to be malignant.14,15 We have operated on 62 patients with tumors larger than 6 cm without conversion (Fig. 1). From this, we conclude that LA is an acceptable method for the removal of such tumors, although an increased level of caution has to be practiced. Radiological characteristics, relation to surrounding structures, and the margins of the tumor process all have to be carefully evaluated in order to determine malignancy potential, and if high, the classic open approach is still recommended. 16 Consideration has to be paid to the possibility of port site metastasis when approaching tumors of this size. If infiltration is present then we prefer the open approach because it allows greater removal of infiltrated tissue.
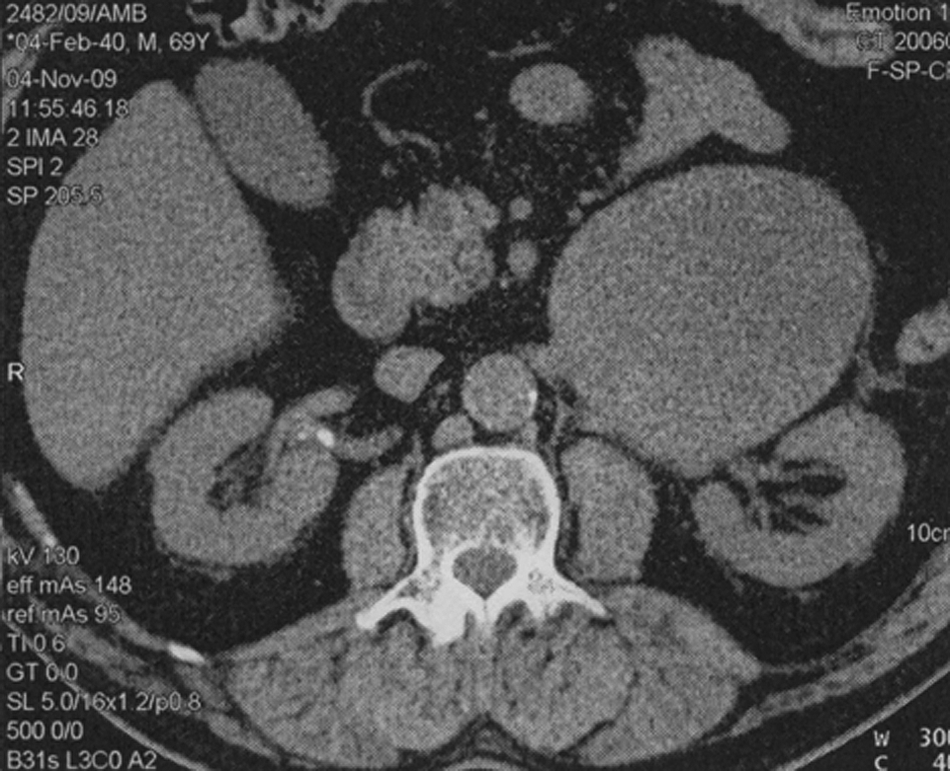
Computed tomography of a large (11.4-×10.6-cm) left-sided adrenal tumor.
A challenge that the surgeon often faces is that of patients with previous abdominal surgery and the aftermath of adhesions that may be present. This becomes a true test of skill because adhesions make access to the lesion more treacherous. More than 30% of our patients have had previous abdominal surgery. We did not have to convert to open surgery in any of these cases. Even after Chevron incisions, LA is feasible in an experienced surgeon's hands (Fig. 2). It requires meticulous dissection, open placement of the first trocar, and mobilization of adhesions. Because of the unpredictable state that may be encountered in the intraabdominal cavity, trocar placement may have to be adjusted accordingly. After these additional initial steps and mobilization of adhesions, the procedure is handled in the same way.

Male patient after bilateral laparoscopic adrenalectomy for renal cancer metastasis in both adrenal glands. The Chevron scar from a previous open nephrectomy is clearly visible (operated on another hospital). For the left-sided adrenalectomy five trocar sites were used because of extensive adhesions. On the right side four trocars were used, and for specimen retrieval one trocar entry point was extended.
In certain patients, such as those presenting with bilateral pheochromocytoma or Cushing's disease, a bilateral adrenalectomy may have to be performed. 17 We have completed 20 such procedures using the laparoscopic approach and can conclude that all the benefits of the method are retained. The only setback is in terms of time spent shifting the patient after removal of one gland and proceeding to the other.
LA in morbidly obese patients may be technically demanding, and these patients are at increased risk for complications as well as a greater chance for open conversion. 18 In our experience, we find that except for the extra efforts that are required on the part of the surgical team, the patient's health is not more compromised than with open surgery (Fig. 3). On the contrary, patients benefit from all the advantages of the minimally invasive surgery. It has been demonstrated that compared with open adrenalectomy, laparoscopy in the morbidly obese offers significantly decreased blood loss, quicker return of bowel function, less analgesic requirement, shorter convalescence, and reduced hospital stay. 19 Also, in patients with Cushing's syndrome, who have delayed wound healing, we did not observe complications regarding wound healing and infection. We must mention that the one and only patient who had a pulmonary embolus had a body mass index of 30 kg/m2, and thus precautions should be taken in these higher-risk patients.

A morbidly obese female patient after right-sided laparoscopic adrenalectomy for glucocorticoid-secreting adenoma (Cushing's syndrome).
In the case of pheochromocytoma, we clip and control the adrenal vein prior to any manipulation of the gland. Although some authors have reported this as unnecessary, 20 we found our patients to have better cardiac rhythm and blood pressure. This logic is based on the attempt to avoid any catecholamine release related to gland manipulation. Specifically, for pheochromocytoma the medical team has to avoid unabated catecholamine release into the systemic circulation, which could lead to devastating consequences through the activation of the sympathetic nervous system.21,22
A case of note with which we were presented involved a male patient with recurrence of pheochromocytoma 9 years after initial right-sided LA for benign pheochromocytoma. The patient presented with characteristic clinical symptoms, and after computed tomography and metaiodobenzylguanidine scintigraphy, a right-sided pheochromocytoma was again suspected. We performed a laparoscopic exploration that revealed a multinodular infiltrating tumor in the adrenal area. Biopsy material was obtained, and after evaluation we concluded malignant pheochromocytoma. After this, an open adrenalectomy was performed as well as ipsilateral nephrectomy and a partial resection of the vena cava in order to remove infiltrating tumor radically.
To conclude, LA is a method of choice for treatment of benign adrenal pathology. It can be safely performed for bilateral pathology as well as in morbidly obese patients or patients after previous abdominal surgeries. When performed by a skilled laparoscopic team it is an effective, low-morbidity procedure having all the benefits of minimally invasive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.