
Abstract
Abstract
Aim:
Postcricoid cancer is an aggressive neoplasm that presents specific therapeutic problems. This study compares laparoscopic stomach mobilization following total pharyngolaryngoesophagectomy (TPLE) with open mobilization following TPLE with respect to postoperative recovery, perioperative morbidity, and mortality.
Subjects and Methods:
This is a retrospective study in a contemporary series of patients with resectable postcricoid cancer from a single institute (Gujarat Cancer & Research Institute, M.P. Shah Cancer Hospital, Ahmedabad, Gujarat, India). Twenty-five consecutive patients who underwent laparoscopic TPLE were compared with 40 patients who underwent open TPLE from January 2006 to December 2010.
Results:
Laparoscopic and open TPLE procedures were compared with respect to patient demographics, operative information (blood loss, duration), and complications. The mean duration of surgery was 3.5 hours in the laparoscopic group and 5.5 hours in the open group. The respective mean blood loss was 290 mL and 460 mL. The respective mean time to full oral intake was 10 days and 11 days. The respective average duration of hospitalization was 13 days and 17 days. In the laparoscopic group, 3 (12%) and 4 (16%) patients had pneumonic consolidation and wound infection, respectively, compared with 8 (20%) and 8 (20%) patients in the open group. In the laparoscopic group, there were two (8%) perioperative deaths, compared with four (10%) in the open group.
Conclusions:
Laparoscopic TPLE is safe with less morbidity and mortality and quicker postoperative recovery compared with open surgery.
Introduction
The aim of this study is to compare the outcomes from laparoscopic TPLE with those from open TPLE in a contemporary series of patients from a single institute (Gujarat Cancer & Research Institute, M.P. Shah Cancer Hospital, Ahmedabad, Gujarat, India.
Subjects and Methods
This is a retrospective study of patients with disease in the postcricoid region with or without extension to the posterior pharyngeal wall, pyriform fossa, or cervical esophagus and who were resectable on exploration. This study compares patients operated on from January 2006 to December 2010 in the different surgical units at a single institute. The patients registered under the laparoscopy unit underwent laparoscopic gastric mobilization, while the patients registered under the units not performing laparoscopic surgery underwent open gastric mobilization. Twenty-five consecutive patients who underwent laparoscopic TPLE were compared with 40 patients who underwent open TPLE. Ten patients (40%) were post-chemoradiation in the laparoscopy group, while 17 (42.5%) in the open group were post-chemoradiation. They underwent salvage surgery for biopsy-proven recurrence or residual disease.
The patients underwent routine hematological investigations and barium swallow (Fig. 1) along with histological confirmation of disease by direct laryngoscopic evaluation and computed axial tomography scan to confirm the operability (Fig. 2). The surgery consisted of cervical exploration through a collar incision. Bilateral selective neck dissection (Level II, III, and IV) was done followed by total laryngopharyngectomy. In the open group, an upper midline laparotomy was done, the stomach was mobilized, preserving the right gastroepiploic and right gastric vessels, and blind transhiatal dissection of the esophagus was done. In the laparoscopy group, the four-port technique was used with two 10-mm ports and two 5-mm ports. The camera port was placed supraumbilically in the midline, with two working ports in the right and left hypochondrium in a slightly superior plane. Another 5-mm port was placed in the epigastric region in the midline (Fig. 3). The specimen was delivered through the neck incision, and then the esophagus was divided at the gastroesophageal junction (Fig. 4). The stomach was positioned in the posterior mediastinum and assessed for viability and its ability to reach the oropharynx without tension. Care was taken for appropriate orientation of the stomach. The size of the pharyngostoma was estimated, and fundal gastrotomy was performed accordingly. In all cases the whole stomach was used as a conduit, which was then anastomosed to the pharynx (Fig. 5). A feeding jejunostomy was placed in all the patients (Fig. 6).

Barium swallow of a patient with postcricoid cancer.
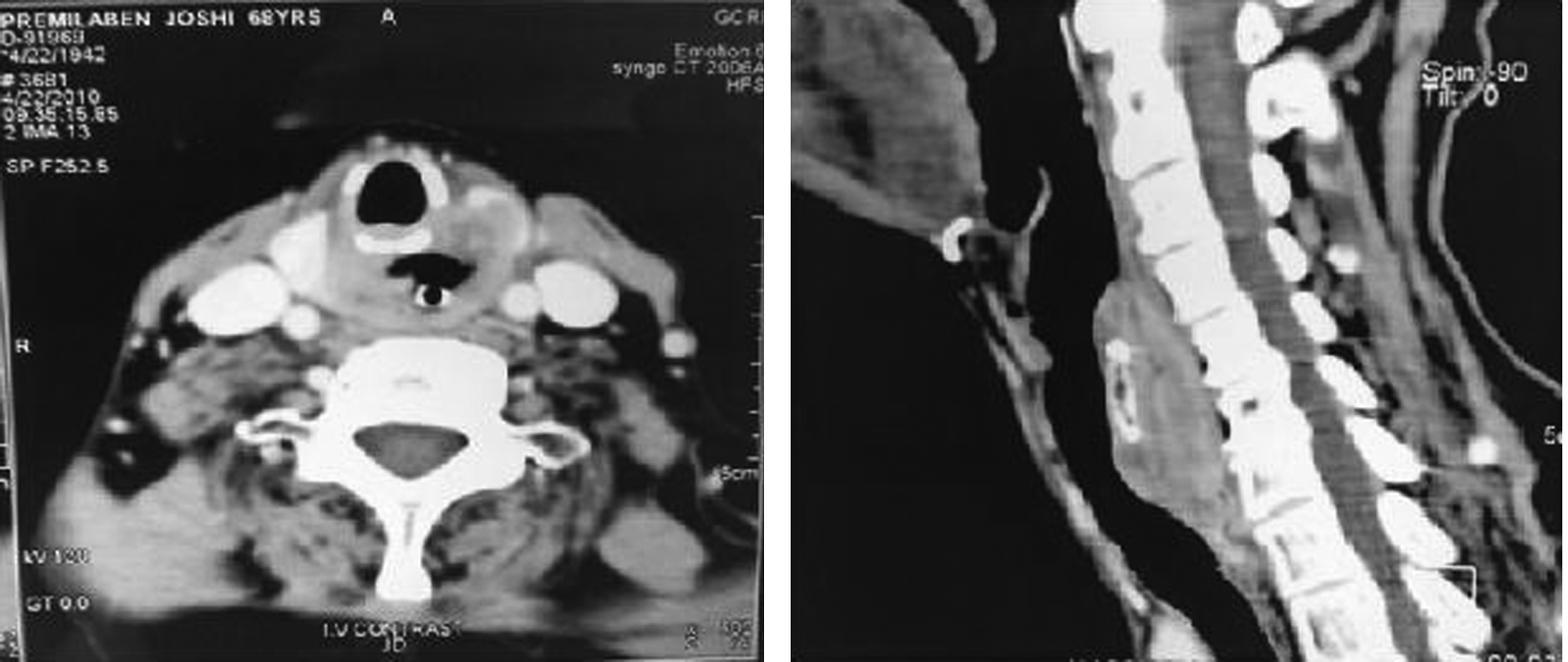
Computed axial tomography scan of a patient with postcricoid cancer.

Port placement.

Specimen from total pharyngolaryngoesophagectomy plus bilateral Level II, II, and IV cervical lymph node dissection.

Pharyngogastric anastomosis.

Immediate postoperative appearance.
Standard postoperative care, which included antibiotics, intravenous fluids, chest physiotherapy, and analgesics, was observed for all the patients. Enteral nutrition started on postoperative Day 2 via feeding through a jejunostomy tube. An oral test feed was given on postoperative Day 5, and if no evidence of leak was seen, full feeding was initiated. The jejunostomy tube was removed when the patient was able to swallow and retain a full diet. Once the histopathology report was available, standard adjuvant treatment was given as per the TMN staging. The outcomes from laparoscopic TPLE compared with open TPLE with respect to patient demographics, operative information (blood loss, duration, and complications of surgery), and short-term results were evaluated.
Results
In the laparoscopy group, 25 patients, of whom 5 were male and 20 were female, underwent surgery. In the open group, of the total of 40 patients who underwent surgery, 12 were male and 28 were female. Median age was 40 (range, 28–65) years in both groups
In the laparoscopy group, 3 patients (12%) developed pneumonic consolidation, and 4 patients (16%) had a wound infection. In the open group, 8 patients (20%) developed pneumonic consolidation, and 8 patients (20%) had a wound infection. The complications are shown in Table 1. In the laparoscopy group, there were two (8%) perioperative deaths, one due to internal jugular vein blowout following anastomotic leak and one due to tracheal injury. In the open group there were four (10%) deaths, three due to septicemia following pneumonia and one due to cardiac arrest during exploration for thoracic duct leak. The histology of all the patients was squamous cell carcinoma.
IJV, internal jugular vein.
The final stage of the cancer was comparable in both groups, with 80% being stage IVA as shown in Table 2. The patients whose final stage was I or II had undergone salvage surgery for recurrence after curative chemoradiation, whereas of the patients undergoing surgery for stage III disease, 1 patient in each group underwent upfront surgery as the preoperative computed axial tomography scan was suggestive of major cricoid cartilage involvement, while the others underwent salvage surgery. In the laparoscopy group 6 (30%) patients with stage IVA underwent salvage surgery, whereas 11 (34%) patients in the open group underwent salvage surgery.
Discussion
An extensive search in PubMed was conducted to review the literature available on this technique; however, only limited data are available. Advanced carcinoma of the hypopharynx and postcricoid region are formidable challenges to the skills of the cancer surgeon. Ong and Lee 2 and LeQuesne and Ranger 3 pioneered TPLE and gastric transposition. These authors challenged the opinion of Goligher and Robin 4 that the stomach would never reach the pharynx. Montgomery et al. 5 were among the first to report the use of laparoscopic gastric mobilization in patients with postcricoid cancer. The posterior mediastinal dissection is undertaken through the hiatus under direct vision. This allows for decreased complications associated with blind dissection such as cardiac impairment, tracheal perforation, aortic bleeding, and pneumothorax. 6 Open TPLE is also associated with significant pulmonary complications.
Although it has been questioned whether laparoscopic techniques can provide adequate oncological clearance, there is no reason to expect any increase in local recurrence or distant or port site metastases as mobilization of the tumor is performed by open neck dissection. 7 Laparoscopic mobilization is reserved for essentially normal tissue and follows conventional surgical methodology. Wong et al. 8 have until now reported the largest experience on minimal invasive approach of gastric mobilization and esophageal dissection with 12 TPLE procedures, of which 9 were done totally laparoscopically and 3 were performed hand-assisted. This series confirmed the feasibility of the laparoscopic approach and demonstrated its safety. The mean operative time was 8.5 hours (range, 5–11 hours), there was no 30-day mortality, and the morbidity rate was 42%, which was more favorable in comparison with their open approach. In our series mean duration of surgery was 3.5 hours, of which the mean time taken for laparoscopy was 2 hours, but as the experience increased in the last 8 cases it was 1.5 hours. This observation is comparable to what was reported by Wong et al. 8 with a median total operative time of 8.5 hours (range, 5–11 hours) and a laparoscopic time of less than 4 hours. Mean duration of hospital stay in our patients was 13 days (range, 7–37 days), comparable to what reported by Rossi et al. 9 and less than that by Wong et al., 8 where the mean hospital stay was 41 (range, 18–75) days.
Our initial experience has shown that laparoscopy has many advantages over the open procedure, in terms of rapid recovery due to fewer respiratory and other complications arising from laparotomy. Laparoscopy does not affect the prognosis, but postoperative recovery definitely improves. As the pleural cavity is not breached, the potential pulmonary insult is minimized, and the absence of an upper midline incision further reduces postoperative wound pain. There was less blood loss in the laparoscopic TPLE group than in the open approach group. In our laparoscopic TPLE group 73% of patients had postoperative morbidity, whereas 89% of the patients developed morbidities in the open group. There was significant reduction in respiratory complications with the laparoscopic TPLE group (12%) compared with the open group (20%). Wound complication rate was also reduced in the laparoscopic TPLE group. The immediate postoperative mortality was also less in the laparoscopy group. Shuangba et al. 10 in their review of 208 patients over 20 years had a postoperative morbidity rate of 41.8% following open gastric pull up. Our morbidity rate is much higher compared with this study.
Various other minimally invasive methods had been reported on gastric and esophageal mobilization. Law et al. 11 compared the thoracoscopic approach of esophageal mobilization with the traditional open transhiatal technique and could not demonstrate any significant reduction in mortality or morbidity. The potential benefit of the thoracoscopic approach could have been offset by prolonged one-lung ventilation, and an upper midline incision was still required for gastric mobilization. Free flap reconstructions using a jejunal free flap and tubed gastro-omental free flap are also now standard techniques for reconstruction of the pharyngoesophageal defect.12,13 Conventional harvesting of the jejunal segment is performed with a midline open laparotomy, which is associated with complications including prolonged ileus, abdominal pain, wound infection, or dehiscence, which has given way to laparoscopic harvesting of the free flap. 14 Thus minimally invasive techniques are here to stay for the reconstruction of the pharyngoesophageal segment following TPLE.
Conclusions
A minimally invasive technique for stomach pull up in patients with postcricoid carcinoma is safe and comparable with an open approach with respect to operative technique and procedure-related complications. The patient's outcome from TPLE with respect to morbidity and perioperative mortality comparing the open approach with a laparoscopic TPLE shows a favorable result in the latter group. The laparoscopic TPLE group had less operative blood loss, decreased respiratory complications, and decreased hospital stay compared with the open group. The application of minimally invasive techniques has the potential to decrease morbidity, hospital stay, and other outcomes when compared with open methods. As this procedure is associated with a learning curve, results improve with time.
Footnotes
Disclosure Statement
No competing financial interests exist.