
Abstract
Abstract
Background:
Laparoscopic colorectal procedures (LCPs) are technically demanding; previous abdominal surgery may add to their complexity. The aim of our study was to assess the effect of previous abdominal surgery (PAS) on laparoscopic colorectal surgery.
Subjects and Methods:
A prospective database was used to record LCPs between 2001 and 2011. Patients were divided into two groups: Group A consisted of patients with no PAS, and Group B of patients with PAS. Data collected included prior abdominal operations, type of LCP, operative time, and conversions. Operative mortality, morbidity, and ward stay in both groups were compared. Statistical analysis was performed using Fisher's exact test and Student's t test.
Results:
One hundred eighty-one patients underwent LCPs: 113 in Group A and 68 in Group B. Mean operative time in Group A and Group B was 216.5 (range, 60–520) minutes and 233.2 (range, 114–544) minutes, respectively (P=.17). In the first 90 cases, the mean operative time was significantly lower for Group A (203 minutes) than in Group B (236.5 minute) (P=.02). The rate of conversion was 10.6% (12/113) in Group A and 13.2% (9/68) in Group B (P=.6). Two patients in Group B had small bowel enterotomies (1 missed on the operating table) compared with none in Group A. Morbidities were comparable in both groups. Median hospital stay was 4.5 and 4 days in Groups A and B, respectively (P=.9). There were 3 deaths in Group A (2 due to medical causes and 1 surgical-related). One surgical-related death (missed enterotomy) occurred in Group B.
Conclusions:
Short-term outcomes of laparoscopic colorectal surgery in patients with PAS are acceptable. There is no significant difference in conversion rate, hospital stay, morbidity, or mortality. The difference in the operative time is significant only in the early part of the learning curve. Meticulous adhesiolysis to avoid and recognize enterotomy is of paramount importance.
Introduction
Subjects and Methods
A prospective database was used to record LCPs performed at our institution between 2001 and 2011. This included benign as well as malignant pathology. The results of the study are based on the experience of a single surgeon. Patients who had stomas without resection (32 laparoscopic stoma procedures) were excluded from this study. Other exclusion criteria included emergency procedures and cancer resections with curative intent in the first 5 years. Patients who had had multiple previous operations or were morbidly obese were not considered suitable for laparoscopic approach in the first 5 years. Since the updated National Institute for Health and Clinical Excellence guidelines in August 2006, with the subsequent increase in the number of LCPs and hence progressive improvement of the learning curve, multiple previous operations and morbid obesity were no longer contraindications. Patients were divided into two groups: Group A consisted of patients with no previous open abdominal surgery, and Group B of patients with PAS. The information regarding previous abdominal operations and type of LCP was recorded in the database. The study compared between both groups the following criteria: operative timing, conversion rate, 30-day postoperative mortality, major surgical morbidity, and median postoperative hospital stay. The previous operations in Group B included laparoscopic and open procedures and were further grouped into midline and lateral scars. LCPs were subdivided into right-side, left-side, and multisegmental resections. Operative timing was recorded from a computerized operating theater system and calculated from the moment the patient was on the theater table until the end of the surgical procedure. Conversions were based on intention to treat. Statistical analysis was performed using Fisher's exact test and Student's t test.
Results
There were 431 consecutive colorectal procedures performed between 2001 and 2011, of which 213 (49.4%) were LCPs and 218 (50.6%) were open procedures. Among the LCPs (study group), there were 118 operations performed for malignant pathology (65.2%) and 63 procedures for benign pathology (34.8%). Of the 213 LCPs, 32 laparoscopic stomas were excluded. The remaining 181 patients who underwent an LCP were divided into 113 patients in Group A (no PAS) and 68 patients in Group B (PAS). There were no significant differences in age, sex, or American Society of Anesthesiologists grade between the two groups (Table 1).
ASA, American Society of Anesthesiologists; LCP, laparoscopic colorectal procedure; PAS, previous abdominal surgery.
The mean operative time in Group A was 216.5 (range, 60–520) minutes compared with 233.2 (range, 114–544) minutes in Group B; this difference was statistically not significant (P=.17). In the first 90 cases, the mean operative time was significantly lower for Group A (203 minutes) than for Group B (236.5 minutes) (P=.02). Subgroup analysis og the operative time in right-side, left-side, and multisegmental resection showrf no statistical significance between the groups (P=.06, .8, and .8, respectively).
The rate of conversion was 10.6% (12/113) in Group A and 13.2% (9/68) in Group B (P=.6).
The median hospital stay was 4 (range, 1–36) and 4.5 (range, 1–52) days in the two groups, respectively (P=.9). Postoperatively, 10 patients in Group A were admitted to the high dependency unit/intensive therapy unit with a median stay of 1 day (range, 1–7 days), compared with 11 patients in Group B with a median stay of 1.5 days (range, 1–14) days (P=.3) (Table 2).
HDU/ITU, high dependency unit/intensive therapy unit.
No intraoperative enterotomy occurred in Group A, but there were two incidental enterotomies in Group B, one of which was missed and subsequently the patient developed peritonitis. During the 30-day postoperative period 3 patients developed mechanical obstruction requiring surgery: 1 patient in Group A (0.9%) and 2 in Group B (2.9%) (P=.6). Ten patients in Group A (9%) had postoperative ileus compared with 5 patients in Group B (7.4%) (P=.8). The wound infection rate was 13.3% (15/113) and 11.8% (8/68) in Groups A and B, respectively (P=.8). Additionally, 2 patients developed an anastomotic leak in Group A (1.8%) but none in Group B (P=.5).
The mortality rate was 2.7% (3/113), with one death due to surgical morbidity, in Group A and 1.5% (1/68), which was surgically related, in Group B (P=1). These results are summarized in Table 3.
Twenty-nine LCPs were performed in the first 5 years of the study. Of these, 34.5% (10/29) had had PAS. Since August 2006, 152 LCPs were performed, of which 58 (38.2%) had had PAS (P=.8).
The laparoscopic procedures were subdivided into right-side, left-side, and multisegmental resections. The breakdown of the LCPs is shown in Figure 1; again, this shows no statistically significant difference in the number of right-side, left-side, or multisegmental resections between the two groups (P=.09, .15, and .77, respectively).
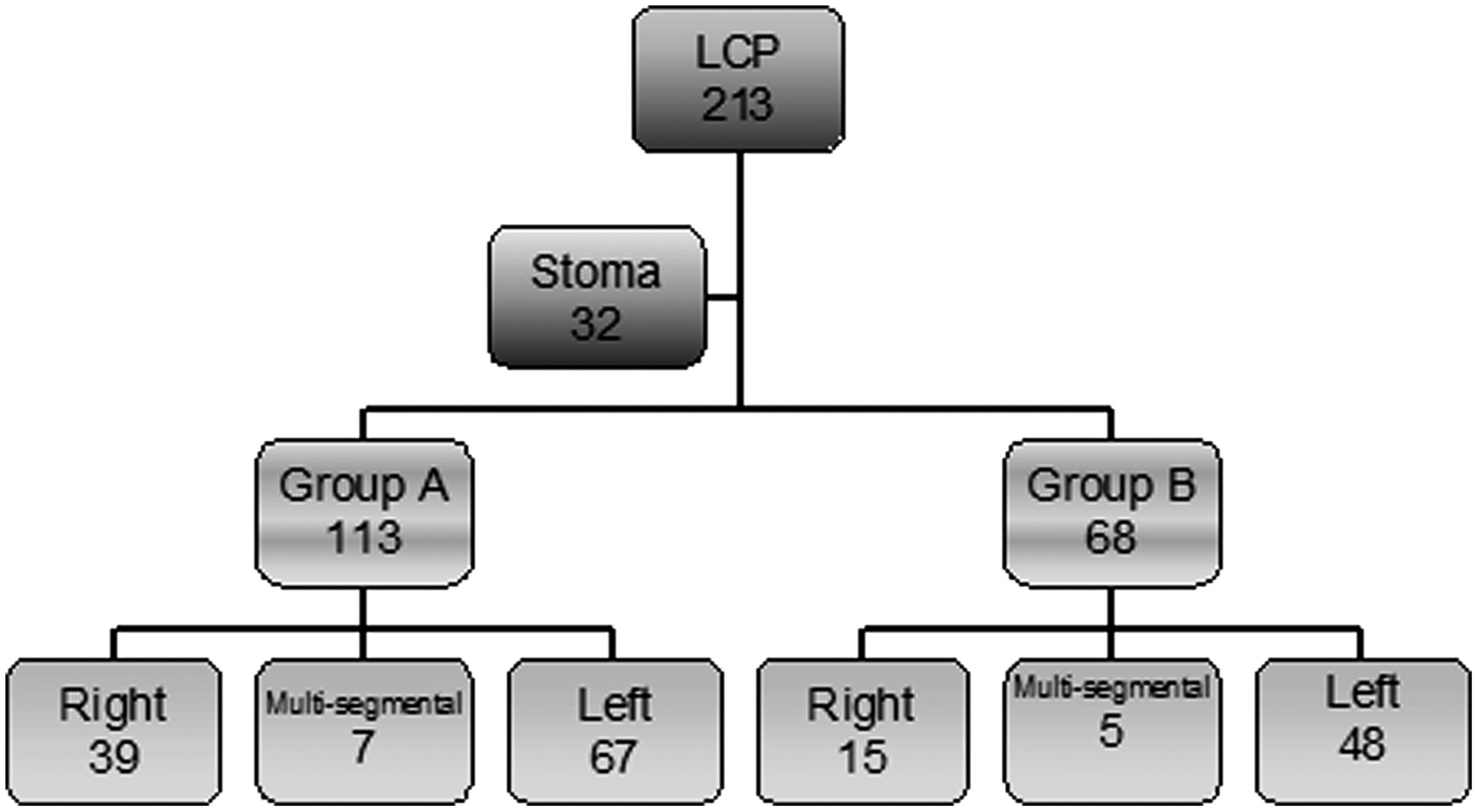
Flow diagram of laparoscopic colorectal procedures (LCPs). Group B patients had had previous abdominal surgery.
The breakdown of the previous surgery for patients in Group B is shown in Table 4. Eighteen patients in this group had more than one operation.
Discussion
Postoperative adhesions are inevitable consequences of abdominal surgery. This seems to occur more after open surgery than after laparoscopic procedures. 2 The incidence of adhesions after previous surgery varies with types of incision. Karayiannakis et al. 3 studied the effect of PAS on laparoscopic cholecystectomy. In a large cohort of 1638 patients, adhesions were found in 70.7%, 58.8%, and 2.1% of patients who had had previous upper, lower, or no PAS, respectively. Adhesiolysis was required in 78%, 30%, and 0% of these cases, respectively. The conversion rate was higher in patients with upper abdominal incision. 3
An LCP has the advantage of a smaller incision, less postoperative pain, and early recovery/discharge. PAS could be considered a contraindication for LCPs for surgeons early in their learning curve. Extra time is required for meticulous adhesiolysis, using additional ports and frequent change of camera position. This 10-year study reveals our experience with LCPs, including the learning curve. Because of the previous restrictions of the National Institute for Health and Clinical Excellence on suitability of laparoscopic resection for malignant disease, there was a small number recruited before August 2006; however, there was no significant difference between the early and the later parts of the learning curve in the percentage of patients who had had PAS (34.5% versus 38.2%).
Presumably patients undergoing an LCP with prior surgery should take longer operative time, probably related to adhesiolysis prior to port placement. Similar results have been shown in various studies 4 ; however, when similar studies included only right-sided resections, no difference in time of surgery was found between patients who had or did not have any previous abdominal operations.5,6 During our learning curve, there was a statistical significant difference in the operative time between patients who had had no PAS and those who had had previous abdominal operations. With the increase in the laparoscopic workload (91/181 in the last 2 years) the contemporary difference is not statistically significant.
The mixture of right-side, left-side, and multisegmental resection was similar in both groups as shown in Figure 1.
Review of the literature reveals contrasting numbers; however, all studies have revealed an acceptable conversion rate, with the maximum being 19.2%.6,7 Barleben et al. 6 commented on higher conversion rates in patients having left-sided resection with PAS. The other thing to consider is the definition of conversion, which is quite variable. We based this on intention to treat rather than decide later based on diagnostic laparoscopy. In our study there was no statistically significant difference in conversion between the two groups: 13.2% versus 10.6%, respectively.
The most serious complication of adhesiolysis is small bowel enterotomy, especially if it is missed at the time of operation. In a large series of 820 patients undergoing laparoscoic colorectal surgery in Pennsylvania, patients with PAS had a significantly higher rate of inadvertent enterotomy (5/347 [1.4%] versus 1/473 [0.2%]; P=.04; odds ratio 6.9), a higher incidence of postoperative ileus (23/347 [6.6%] versus 14/473 [3.0%]; P=.012; odds ratio 2.3), and higher reoperative rates (8/347 [2.3%] versus 1/473 [0.2%]; P=.006; odds ratio 11.1). 8
Despite the small difference in enterotomy between the two groups (none versus two), enterotomy is a serious complication with possible fatal consequences if missed at the time of operation. There was no significant difference in postoperative ileus or intestinal obstruction between the two groups (9 versus 7.4 and 0.9 versus 2.9).
This study looked only into the 30-day postoperative morbidity and mortality. We are aware that the number of patients in the study may not be large enough to show statistical significance for certain parameters concerning morbidity/mortality (Type II error).
The mortality rate was 2.2% for the whole series, which is slightly high, but this may be a reflection of the level of co-morbidity in our catchment population (36% were American Society of Anesthesiologists Class 3 or more).
In our study, median ward stay was comparable in both groups. This has been reflected in most of the previous studies.4–7,9 Median ward stay for conversions was longer (11 days).
Although a lot of technological changes may have occurred in the last 10 years (e.g., high-definition laparoscopic system with improved instrumentation/energy devices and flexible endo staplers that facilitate multisegmental resections and low pelvic dissection), the principles remained the same for patients who had had PAS. An open lateral Hassan port away from the previous scar is routinely used. We tend to use more ports, which are more laterally placed during adhesiolysis. Dynamic change of the camera and table positions is usually helpful. We perform adhesiolysis in a stepwise fashion using scissors, dividing adhesions between the abdominal wall and omentum/bowel followed by adhesions between the omentum and bowel. Division of the adhesion between small bowel loops and the mesorectum is usually required. Inter-loop small bowel adhesions are divided only if necessary.
Our study has shown feasibility of LCPs in patients with PAS. Most studies, including ours, have been retrospective, which carries a possible selection bias. There may be place for a randomized control trial of LCPs in patients with previous abdominal operations. Subgroup analysis was limited in our study. Further detailed analysis can be addressed in larger series.
Conclusions
Short-term outcomes of laparoscopic colorectal surgery in patients with PAS are acceptable. There is no significant difference in conversion rate, hospital stay, morbidity, or mortality. The difference in operative time is significant only in the early part of the learning curve. Meticulous adhesiolysis to avoid and recognize enterotomy is of paramount importance.
Footnotes
Disclosure Statement
No competing financial interests exist.