
Abstract
Abstract
Background:
We developed a non-survival in vivo model for testing of gastric natural orifice translumenal endoscopic surgery (NOTES) closures based on the gastric yield pressure. The aim of this study was to test our model comparing different endoscopic closure techniques with surgical closure of a NOTES gastric incision.
Methods:
Laparotomy was performed in 30 pigs. One tube for air inflation and one manometry tube were inserted into the stomach via the pylorus, which was closed gas-tight, and the abdominal wall was closed. The stomach was inflated with air, and the gastroesophageal yield pressure was measured. A gastroscopy was performed, and a standard NOTES access was created followed by randomization to closure by surgical suturing, T-tags, Padlock-G over-the-scope (OTS)-clips, OVESCO OTS-clips, and traditional clips. All closures were tested twice with air insufflation. Gastric yield pressure or leak pressure of each closure was recorded.
Results:
The mean baseline gastric yield pressure was 80.5 mm Hg. Post-closure yield pressure was 79.9 mm Hg. Leak test results after closure were as follows: surgery, 0/6 leaked; T-tags, 1/6 leaked before reaching yield pressure (56 mm Hg); Padlock-G, 2/5 leaked (71.5 mm Hg); OVESCO OTS-clips, 3/6 leaked (27.2 mm Hg); and traditional clips, 5/6 leaked (27.2 mm Hg). TAS T-tags and surgical closures leaked significantly less than the other groups (P=.01). Traditional clips and OVESCO OTS-clips leaked at significantly lower pressures than the other three groups (P=.007).
Conclusion:
This in vivo model using leak of the closure or the gastric yield pressure as endpoints for testing of the closure strength of a NOTES gastric access site seems to be reproducible. Our results support closure with T-tags and Padlock-G-clips over OVESCO OTS-clips and standard endoscopic clips.
Introduction
There seems to be no clear answer to the question of what is the amount of force that is imposed on a gastric closure after a NOTES procedure. Postoperative nausea and vomiting result in high intragastric pressures. In healthy volunteers intragastric pressure during retching and vomiting has been reported as high as 290 mm Hg. 3 But, simultaneously the intraabdominal pressure increased to 255 mm Hg, and the resultant pressure inflicted on the gastric wall and the closure site was far less. In clinical situations even endoscopic clip closure has been shown to be sufficient in securing gastric perforations, 4 even if bench top testing has shown otherwise. Our hypothesis is that the actual stress on the gastric closure in a patient will not exceed the gastric yield pressure (the pressure where the cardia opens and the patient burps or vomits). Therefore we have developed an experimental in vivo model for testing of gastric access site closures in which the intragastric pressure does not exceed the yield pressure.
The aim of this study was to test and evaluate our new experimental in vivo model based on the gastric yield pressure comparing different techniques for gastric closure.
Materials and Methods
The first part of these experiments was performed at the Sahlgrenska University Hospital in Gothenburg, Sweden, and the second part at the Vall d'Hebron University Hospital, Wider-Barcelona in Barcelona, Spain. Ethical approval had been obtained from the local Institutional Review Boards.
Animals
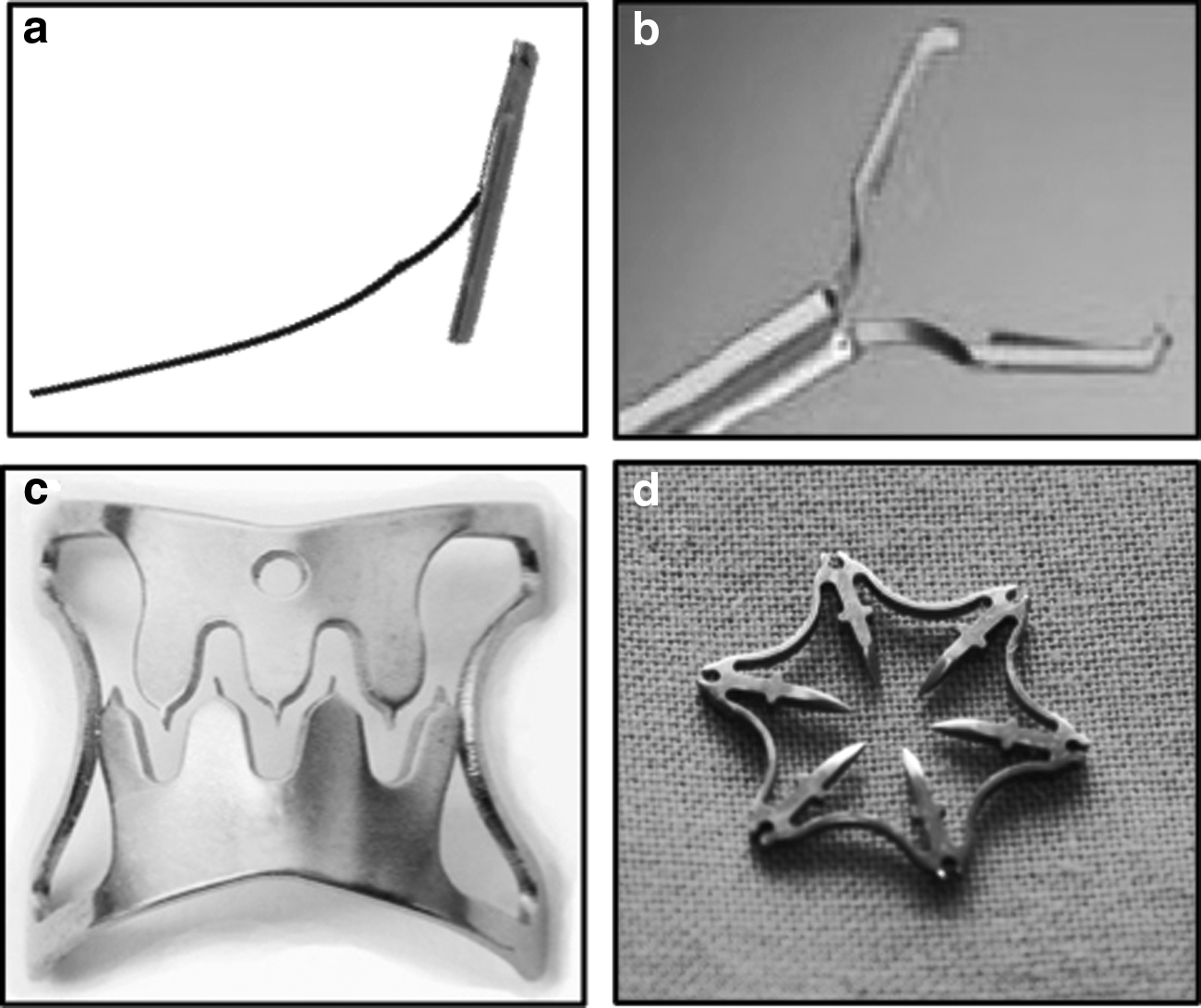
Thirty Landrace pigs with a mean weight of 35 kg (range, 24–43 kg) were used. The animals were kept on a liquid diet for 3 days before the experiments and were allowed nothing orally except for free access to water for 12 hours before the procedure. In the first part of the study 18 animals were randomized to two different endoscopic closure techniques: T-tag (TAS, Ethicon Endo-Surgery, Inc., Cincinnati, OH) and standard Boston clips versus open surgical closure (single-layer sero-muscular running suture, 3-0 resorbable monofilament), with 6 pigs in each group. In a second part 12 animals were included for closures with two different OTS clips: the commercialized OVESCO clip (Ovesco Endoscopy AG, Tübingen, Germany) and the prototype Padlock-G clip (Aponos Medical, Kingston, NH) (Fig. 1). This was done as the latter clips had been released just after the start of our study and seemed promising for closures.
Endoscopic closure was performed using
Experimental setup
The experimental model was equally prepared in all animals. A 10-cm midline laparotomy was performed with the pig under general anesthesia. Through a duodenotomy two catheters were placed into the stomach via the pylorus: one standard four-channel manometer catheter (Medtronics Inc., Minneapolis, MN) and a nasogastric tube for air insufflation (22 F). The pylorus was tightened over the tubes to prevent air leakage from the stomach, and the abdominal wall was closed using graspers (Fig. 2). The position of the catheters was checked by endoscopy. After removal of the endoscope, air was inflated at 3.5 L/minute into the stomach, and the gastric yield pressure was measured twice by recording the gastric pressure level when the pig burped and the manometry curve peaked. The experimental setup is shown in Figure 3. The mean yield pressure value was calculated from the two measurements and the four manometry channels. An Olympus (Hamburg, Germany) GIF 140 gastroscope was used.
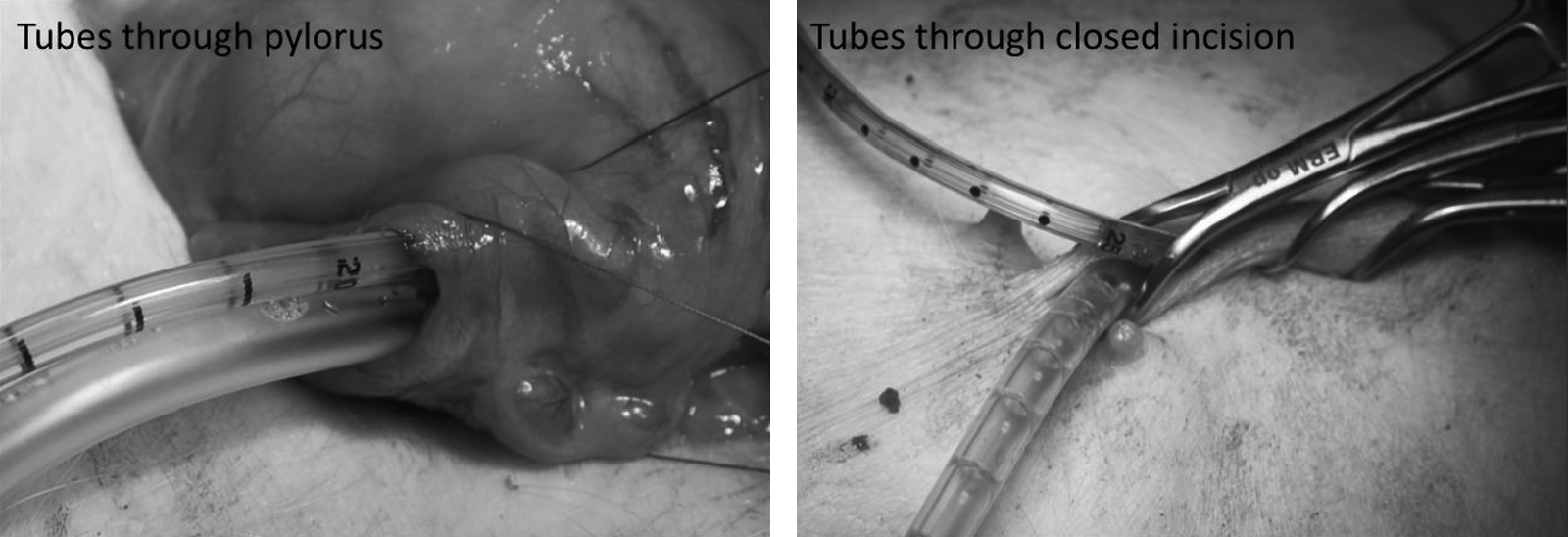
One manometry tube and one tube for air insufflation were placed through the pylorus via a duodenotomy. The abdominal wall was closed using towel clamps.
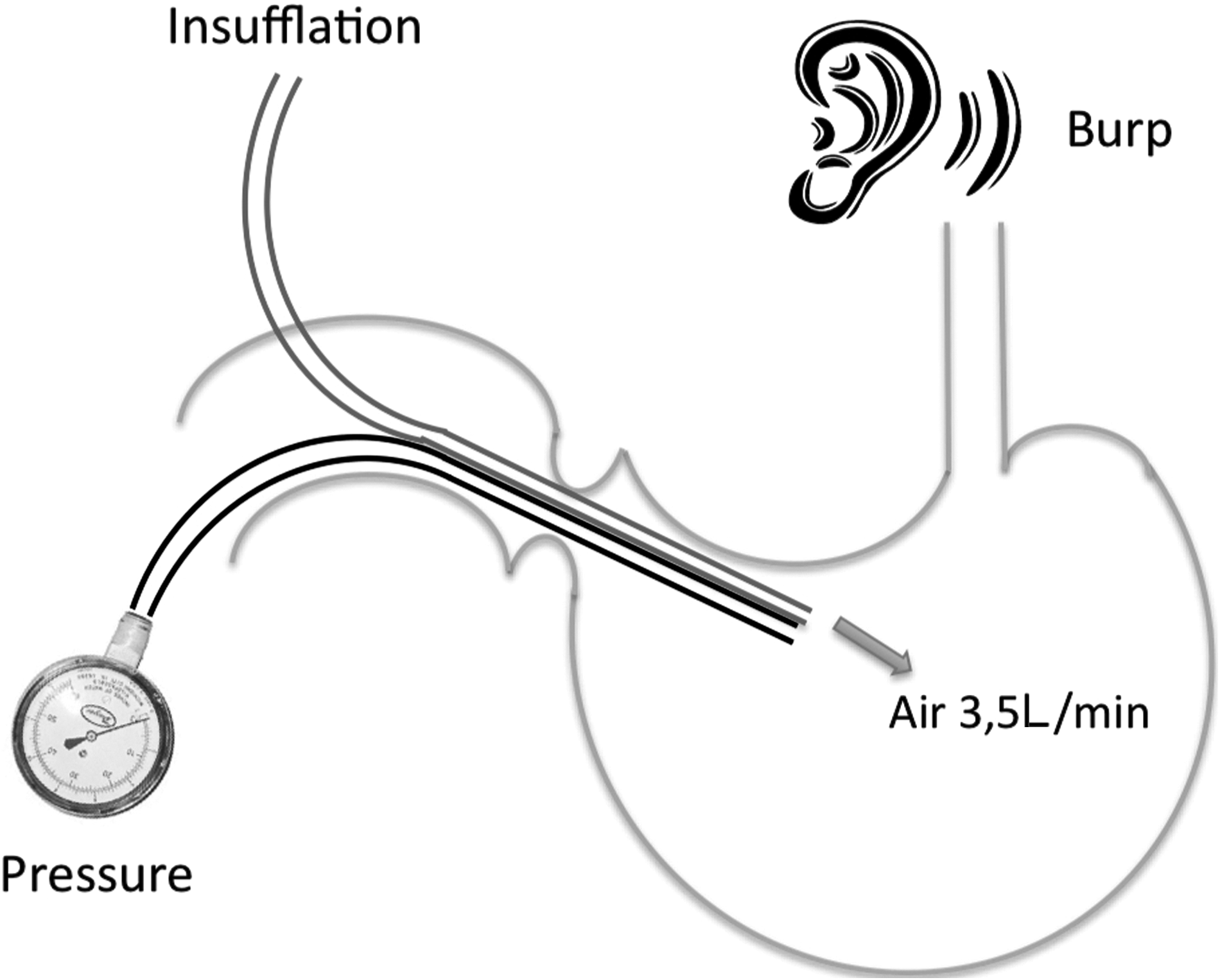
Schematic drawing of the experimental model.
Experiment
Transgastric peritoneal access was achieved as follows. The stomach was perforated using a needle knife in the anterior wall of the antrum, and a guide wire was passed into the peritoneal cavity. The access gastrotomy was dilated over the guide wire with a 20-mm TTS-balloon. The size of the gastrotomy, 20 mm, was chosen to mimic the gastrotomy access in a standard NOTES procedure. The endoscope was then passed into the peritoneal cavity. After withdrawal of the endoscope, randomization took place, and closure was performed using one of the five techniques. After the perforation was closed, air was once again inflated through the catheter into the stomach (3.5 L/minute), and the yield pressure or leaking pressure of the closure was measured twice (if leakage had not occurred during the first test). A mean pressure for yielding or leakage was calculated from the two measurements and the four manometry channels. To detect leakage from the closure site, water was instilled in the abdominal wound. All perforation/closure sites were then inspected through the endoscope as well as postmortem.
Statistics
Results are given as mean±SD values. Comparisons between groups were performed using non-parametric tests: the Kruskal–Wallis test for multiple non-related data and the chi-square test for nominal data. All statistics were processed using SPSS (Chicago, IL) version 19 software. Differences were considered statistically significant at P<.05.
Results
The initial yield pressure for all animals was 78.9±27.6 mm Hg without any significant differences among the groups. One animal was withdrawn from the Padlock-G group as the cardia was insufficient and yield pressure was not measurable. Post-closure yield pressure for those animals that did not leak was 79.9±29.3 mm Hg. It did not differ from the baseline pressure prior to performing the gastrotomy or among the groups.
Open surgical closure
The post-closure yield pressure was 88.9±19.2 mm Hg in the open surgical group without any leakages (Table 1).
TAS T-tags
The gastrotomies were closed using two double stitches. In the TAS group 5 animals reached yield pressure (mean 90.3±30.9 mm Hg). One TAS closure leaked at 56 mm Hg (Table 1).
Endoscopic clips
Five to 10 clips were used for the closures. Only one of the standard clip closures reached yield pressure, at 73.4 mm Hg. The other five closures leaked at 15, 20, 23, 31, and 48 mm Hg (Table 1).
Padlock-G
One clip was used for closure in all except 1 animal, where two clips were used. Three out of 5 animals in the Padlock-G group reached yield pressure at a mean of 53.7±13.7 mm Hg, whereas two closures leaked at 63 and 80 mm Hg (Table 1).
OVESCO
One clip was used in 4 animals. In one animal two clips were used, and in another one three clips. Three OVESCO clips closures reached yield pressure at 72.8±51.4 mm Hg, but the other three leaked at 22, 27, and 55 mm Hg (Table 1).
Comparisons
Comparing type of response at post-closure gastric distension, burp (= yield), or leak (Fig. 4), we found a statistically significant difference among the groups (P=.033, chi-square test). Pairwise comparisons gave statistical difference between open surgery and TAS T-tags versus regular clips (P=.008 and P=.04, respectively) (Fig. 4).
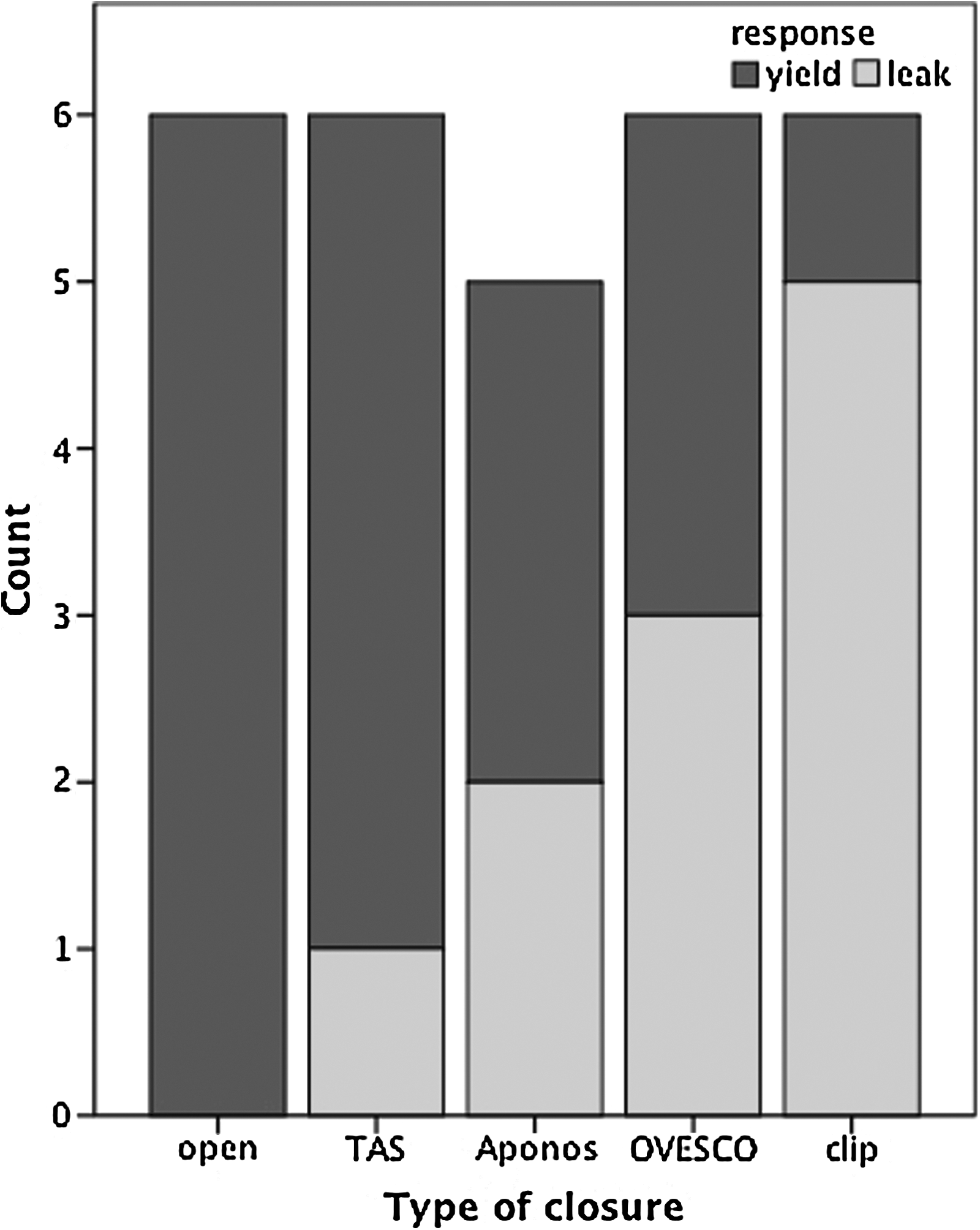
Type of response—yield (burp) or leak—for the different closure techniques. Aponos, Padlock-G.
Discussion
In this non-survival study different closure techniques of a gastric NOTES access have been tested in a new in vivo model using gastric yielding or leakage of the closures as endpoints. Standard hand-sewn and T-bar closures seem to be more reliable than regular endoscopic clips. Half of the closures with the newly introduced OTS clips leaked before reaching gastric yield pressure, indicating non-reliable closures.
The White Paper of the ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery from 2005 states that: “If NOTES is to reach human trials, a 100% reliable means of gastric closure must be developed.” 5 It is also important, as in open or laparoscopic surgery, that the closure allows instant postoperative intake of liquids and that no nasogastric tube is required to relieve and protect the closure.
Various types of clips, suturing devices, staplers, and plugs have been used to close NOTES gastric access incisions.6–9 Tunneled and self-approximating gastrotomy methods have been described to reduce the need for sutured or other mechanical closure methods. 10 It has even been suggested that closure may be unnecessary. 11 However, in clinical practice this would not be acceptable to surgeons or endoscopists.
One relevant question is to which pressure level the gastric closure will be exposed postoperatively. This is also important when designing experimental models for testing closures. Postoperative nausea and vomiting are common problems in a surgical patient population, occurring in an estimated 35% of all cases. 12 Vomiting and retching seem to cause high intragastric pressures and strain on the gastric closure. It has been reported that the intragastric pressure may be as high as 290 mm Hg when retching and vomiting occur. 3 However, in this study the intraabdominal pressure (measured in the bladder) simultaneously reached 255 mm Hg, resulting in a net pressure exerted on the gastric wall and the closure (clips or sutures) of only 45 mm Hg. The retrograde contraction of the muscles in the gastric wall might even decrease tissue tension. The yield pressure in humans varies from very low pressures in patients with gastroesophageal reflux disease up to 15 mm Hg in healthy volunteers. In patients operated on with a 360° fundoplication (e.g., Nissen) the yield pressure will not reach over 40 mm Hg. 13 These relatively low pressures might explain why standard endoscopic clips, only approximating the mucosa, are sufficient for closing NOTES gastric access sites and accidental perforation following endoscopic mucosal resection in patients, 4 even if experimental data indicate the opposite.
Most of the described models for testing gastric closures are either ex vivo1,2,14 or survival6,7,15 models. The optimal test of different closure methods is a survival test, but there is still a need for reliable and reproducible non-survival testing methods. Our model is an in vivo model correlating with postoperative physiologic conditions. One weakness of this model is the individually varying yield pressures of the pigs, but this is also the case in patients. The yield pressure in pigs is higher than in humans. 13 The strength of our model is that both closure and testing are performed in vivo on live tissue. In the ex vivo model described by Voermans et al., 2 the closures of the gastrostomies were performed on the bench, which is easier than in vivo. This might be the reason why the previous researchers found a very high mean leak pressure using resolution clips, whereas we had difficulties in closing the gastric access site with the same clips. In the experiment by Ryou et al., 1 both access and closure were performed on the bench in explanted refrigerated stomachs. Leak pressures were determined by distension with air or water. Explanted refrigerated stomachs are probably more fragile and less elastic than live tissue, which might reflect their result of leaks occurring through the needle/clip holes.
In the current study none of the hand-sewn closures leaked before the distension of the stomach reached yield pressure. T-tag closure performed nearly as well and showed only one leak out of six. This is in line with results from our previous survival studies, where T-tags have shown to be reliable in both gastric and colonic closure.6,16 In our study the Padlock-G clip closures leaked in two out of five closures; however, these leakages occurred at relatively high pressures, 63 and 80 mm Hg, which was close to the overall mean yield pressure (79 mm Hg). The OVESCO clips leaked in half of the cases at relatively low pressures (22, 27, and 55 mm Hg), indicating that they are not reliable for clinical closure of a NOTES gastric access site. This was also found by von Renteln et al. 17 In our experience it seems that these clips are not big enough for a 20-mm gastrotomy. It is probably necessary to bring the entire gastric defect into the clips' opening for secure closure, which is difficult and not always possible because of tissue edema of the edges of the perforation. One explanation for the difference between the Padlock-G clips and the OVESCO clips might be their different designs.
Closures with standard endoscopic clips were in our hands difficult and resulted in leakages in almost all cases. In reported bench testing the strength of similar clip closures has been shown to be inferior to that of other types of closure. 2 However, in other hands these clips have proven to be sufficient to close accidental perforations in clinical situations. 4
Ex vivo and in vivo models are important as a first step for testing and evaluation of new closure techniques. However, the conclusive test of a NOTES gastric access site closure is a non-leaking well-healed closure in a survival model. It is surprising that in survival experiments exploring different surgical NOTES techniques, secure healing of the access site seems not to be a big issue.
Conclusion
The described in vivo model using leak of the closure or gastric yield as endpoints for testing of the closure strength of NOTES gastric access sites seems to be reproducible and offer a more physiologic approach to this issue. Our testing results support closure with T-tags and the Padlock-G clip. However, the number of animals in each group is too low for definite conclusions to be made, and further studies are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.