
Abstract
Abstract
Introduction:
Funded knowledge about the physiological impact of laparoscopic surgery in children is sparse. Although there are data on hemodynamic compromise after creation of a pneumoperitoneum in children, little is known about microcirculatory changes at the mucosa level. Therefore, the aim of this study was to assess gastric microcirculation by continuous gastric air tonometry in the setting of laparoscopic versus open appendectomy.
Patients and Methods:
Twenty children 5–17 years old undergoing laparoscopic and 7 children undergoing open appendectomy were included in the study. Gastric intramucosal CO2 pressure (pCO2i) was measured under standardized flow and intraperitoneal pressure using continuous air tonometry (TONOCAP®, Datex Ohmeda), and ΔpCO2 (pCO2i – end-expiratory CO2 pressure [pCO2e]) was obtained for the time course of surgery.
Results:
ΔpCO2 increased significantly from the baseline value not only in the laparoscopic group but also in the open surgery group. Even though ΔpCO2 was higher in the laparoscopic group at all time points, the overall increase in ΔpCO2 for both groups was uniform. The largest differences were observed during the initial 20 minutes of the operation. The changes observed were exclusively due to an increase of pCO2i in relation to a constant pCO2e.
Discussion:
In the setting of a standardized, simple operation in an otherwise healthy child above the age of 5 years, our data suggest that the effect of a pneumoperitoneum on splanchnic perfusion is comparable to the compromise caused by open surgery. Further research must be obtained when evaluating the full impact of laparoscopy in children.
Introduction
It has been questioned whether laparoscopy by itself is a suitable surgical option in critically ill children. The cardiovascular effects of creating a pneumoperitoneum are well documented and considered to be the results of increased abdominal pressure leading to decreased preload and cardiac output as well as increased ventilator requirements.5,9,10 Additionally, insufflating the peritoneal cavity may cause alterations in heart rate and blood pressure and lead to decreased urinary output, especially in infants.9,10 Other systemic effects of pneumoperitoneum such as the impact of CO2 absorption and stimulation of the neurohumeral vasoactive system have been described.5,10 However, little is known on the physiological impact of laparoscopic surgery in infants and children at the level of the intestinal mucosa.
In adult patients, gastric tonometry has long been a tool for intraoperative assessment of disturbances in acid–base balance and splanchnic microcirculation in both open and laparoscopic surgery.11–15 Splanchnic hypoperfusion results in an increase of cellular CO2 pressure (pCO2) by two mechanisms. First, hypoperfusion induces a switch from aerobic to anaerobic metabolism with increased production of mucosal pCO2. Second, hypoperfusion reduces the “washout” of mucosal pCO2, which then accumulates in the gastric mucosa. According to international standards, adequate mucosal pCO2 measurement is performed as automated recirculating gas analysis, which has proved to be more sensitive than gastric saline tonometry.16,17 Furthermore, gastric intramucosal pCO2 (pCO2i) and the calculation of the ΔpCO2 (as described below) are known to be superior to the intramucosal pH (pHi) calculation because it does not depend on intra- and extracellular bicarbonate concentration.16,17
ΔpCO2 is used in the analysis of data gathered by gastric tonometry because it diminishes the influence of systemic alterations. In order to calculate ΔpCO2, pCO2i measurement is related either to end-expiratory pCO2 (pCO2e) or arterial pCO2 (pCO2a). The pCO2e or pCO2a, which represents the systemic pCO2 at a given time point, is subtracted from pCO2i (ΔpCO2=pCO2i – pCO2e). This is particularly important in the setting of laparoscopic surgery because CO2 insufflated for pneumoperitoneum is rapidly absorbed via the peritoneum, causing alterations of systemic CO2. 18
Here we compare pCO2i levels measured intraoperatively by continuous air tonometry during laparoscopic and open appendectomy in otherwise healthy children. Our initial hypothesis was that the creation of pneumoperitoneum during laparoscopic appendectomy would cause a decrease in splanchnic perfusion of unknown magnitude compared with open appendectomy. By analyzing the impact of pneumoperitoneum on splanchnic perfusion, we hope to better understand the physiological responses and the impact of pneumoperitoneum at the mucosal level during laparoscopic surgery in children.
Subjects and Methods
Patients
Between January 2008 and June 2010, 27 otherwise healthy children (17 boys and 10 girls, 5–17 years old; mean, 10.7 years), in whom either laparoscopic or open appendectomy was performed, were prospectively enrolled in the study. Children were selected into one or the other group because of the surgeon's preference independently of clinical suspicion for perforation. It is important that both groups were homogeneous for age and weight (Table 1). Operations were carried out at either Ingolstadt Hospital or Dr. von Hauner Children's Hospital, both teaching hospitals of Ludwig-Maximilians University Munich, Munich, Germany. Pathologic findings of the excised appendices, operative times, and postoperative course were assessed in all patients. The study was reviewed and approved by the ethics committee of the Ludwig-Maximilians University Munich. Informed consent was obtained from the parents for all children.
Data are mean±SEM values or mean (%), depending on the data set analyzed.
P values were calculated as described in Subjects and Methods.
Surgical technique
All patients in the laparoscopic group underwent standard three-port laparoscopic appendectomy, exclusively stapling the stump. Pneumoperitoneum was established by insufflation of the peritoneum with standard CO2. No laparoscopic case was converted to open. Open appendectomy was through a standard oblique incision in the right lower quadrant and ligation of the stump. Mean operative time was 53 (range, 27–101) minutes for laparoscopic appendectomy and 41 minutes (range, 28–65) minutes for open appendectomy (Table 1).
Intraoperative tonometry
The gastric pCO2i was measured under standardized flow (5 L/minute) and intraperitoneal pressure (10 mmHg) using continuous air tonometry (TONOCAP®, Datex Ohmeda). The pCO2e was recorded from the return flow of the ventilatory circuit (Dräger/Primus®). Data points were measured for both pCO2i and pCO2e prior to establishing a pneumoperitoneum as well as over the course of the surgical procedure every 10 minutes until the end of the case. The pCO2i was related to pCO2e in order to assess the ΔpCO2, defined as the difference between pCO2i and the systemic (=end-expiratory) pCO2 (ΔpCO2=pCO2i – pCO2e). For 16 children who underwent laparoscopic appendectomy and two children who underwent open appendectomy, the corresponding parents gave additional consent in order to obtain pCO2a measurement for comparison with pCO2e at the beginning of surgery.
Statistical analysis
Data are given as mean±SEM values. Aggregated data are represented using the usual descriptive means. Statistical significance of differences was determined by two-tailed Student's t test for scale and the chi-squared test for dichotomous variables. In all tests, differences were considered significant at P<.05.
Results
Changes of pCO2i during open and laparoscopic appendectomy
Both pCO2i and pCO2e were analyzed over the time course of the operation in the laparoscopic and open group and related to one another in order to calculate the ΔpCO2 (Fig. 1). In the laparoscopic group, pCO2i and pCO2e were similar at the initiation of the operation, with a pCO2i of 37.1 mmHg and pCO2e of 34.8 mmHg before and a pCO2i of 41 mmHg and pCO2e of 36.8 mmHg at the initiation of the pneumoperitoneum (Fig. 1A). Over the next 30 minutes, pCO2i steadily rose by approximately 3 mmHg every 10 minutes and then plateaued. Because the pCO2e remained constant during this time, ΔpCO2 increased significantly over the time course of the operation (P<.05). It is interesting that a similar observation was made for changes in pCO2i in children undergoing open appendectomy, although to a lesser extent (Fig. 1B).

Mean intramucosal CO2 pressure (pCO2i) (dots) values and SEM (bars) are shown in relation to their corresponding end-expiratory CO2 pressure (pCO2e) (squares) values over the time course of the operation for
When the ΔpCO2 of the laparoscopic was compared with that of the open group, ΔpCO2 was higher in the laparoscopic group at all time points over the time course of the operation (Fig. 1C). In order to better quantify the differences between ΔpCO2 observed between the two groups, we expressed the ΔpCO2 of the laparoscopic group as a fold increase compared to the open group for each time point (Fig. 1D). The largest differences were observed during the initial three time points (0–20 minutes). At zero-time, ΔpCO2 in the laparoscopic group was increased threefold compared with the open group. At 10 and 20 minutes, the increase in ΔpCO2 in the laparoscopic group was 2.7-fold and 1.7-fold, respectively. For the time points at 30 and 40 minutes, ΔpCO2 was increased by 1.3-fold, and at 50 minutes, 1.2-fold (Fig. 1C, D).
In the recovery room ΔpCO2 decreased to the normal range in both groups (data not shown).
pCO2e represents pCO2a
Laffon et al. 19 found the pCO2e to overestimate the pCO2a (assessed by arterial blood gas analysis) during laparoscopy in children. Therefore, in our study, at the beginning of the operation, pCO2 was measured by arterial puncture and formal arterial blood gas analysis for comparison. Despite some variations, we mostly found pCO2e to correlate with pCO2a (Fig. 2). Fifty percent (9/18 children) of the time, the two data points were within 2.6 mmHg (95% confidence interval). The mean value of all pCO2e data points compared with the mean of pCO2a was 0.7 mmHg. In a paired t test analysis, no significant difference was detected (P=.6633) (Fig. 2).
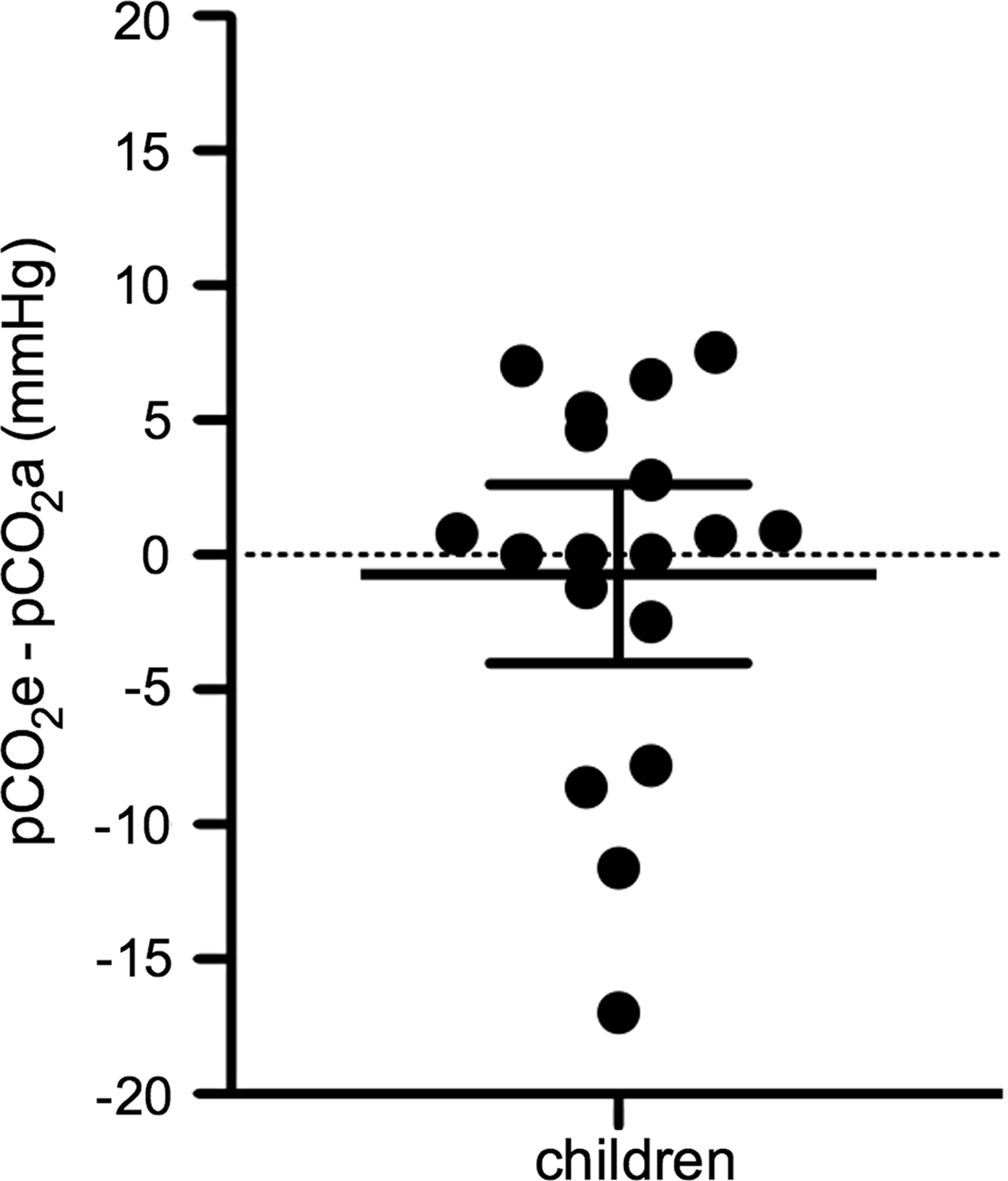
The differences in the individual measurements of pCO2e and arterial CO2 pressure (pCO2a) by formal blood gas analysis at the beginning of each operation are shown in mmHg for 18 children. The closer the dots are to the zero value, the more accurate that data set is. Data points below zero represent underestimation of pCO2e to pCO2a; values above zero represent overestimation. The long horizontal line represents the mean; the shorter lines represent the 95% confidence interval.
Pathological findings
All excised appendices were analyzed routinely by the pathologist, and findings were reviewed for this study. Of the 20 children undergoing laparoscopic appendectomy, one had perforated and 18 had nonperforated appendicitis; one appendix was without pathological finding. Of the 7 children who underwent open appendectomy, two had perforated and four had nonperforated appendicitis; again, one was without pathological finding.
Discussion
The indications for pediatric endosurgery are constantly expanding, and young age and small size are no longer exclusion criteria for laparoscopic surgery.4,5,7 Notwithstanding contradicting data from adult patients, surgical interventions by a laparoscopic approach are traditionally thought to be questionable in critically ill patients because of the ill-defining hemodynamic and metabolic effects of the induced pneumoperitoneum.20,21 However, our understanding of the physiologic response to laparoscopic surgery in childhood is limited. The cardiovascular effects of creating a pneumoperitoneum are thought to mainly result from increased intraabdominal pressure. 9 Very little is known about the impact of CO2 absorption, stimulation of the neurohumeral vasoactive system, and splanchnic hypoperfusion. 10 Therefore, the aim of this study was to compare gastric pCO2i levels measured intraoperatively by continuous tonometry during laparoscopic and open appendectomy in otherwise healthy children. We found ΔpCO2 to increase significantly from the baseline value in both groups. Even though ΔpCO2 was higher in the laparoscopic group, especially during the initial 20 minutes after incision, the overall increase for both groups was uniform.
Tonometry has long been used in critical ill adult patients as a tool for the assessment of gastric mucosal perfusion and was found to have prognostic value.22–25 Furthermore, it is a valuable method for intraoperative assessment of disturbances in acid–base balance and splanchnic perfusion in both open and laparoscopic surgery.11–15 Our own previous data showed that continuous gastric tonometry is a valuable method to assess anastomotic perfusion of the esophagogastrostomy in patients undergoing gastric tube formation for esophageal carcinoma. 13 In a clinical application, our previous data showed that mucosal pCO2 may serve as a predictor for a complicated postoperative course and an indicator for an anastomotic leak in this patient population. 15
Data for comparison regarding gastric tonometry or gastric mucosal perfusion are sparse in children. In one study, in 51 critically ill children an association was found between the pHi measured by tonometry and multi-organ failure. 26 A similar observation was made by Duke et al. 27 in 20 children on extracorporeal membrane oxygenation due to underlying cardiovascular or respiratory compromise regarding mortality. Bichel et al. 28 found that low mucosal pH in children during cardiac surgery to be associated with significantly less frequent life-threatening complications in the early postoperative course. In another study analyzing 38 premature infants with a birth weight of less than 1500 g, decreased pHi was associated with gastrointestinal complications. 29
To our knowledge, no data exist comparing changes of gastric pCO2i in children undergoing standard open versus laparoscopic surgery. In our current study, even though uniform in their overall increase, we found ΔpCO2 to be higher in the laparoscopic group compared to the open group. Our finding that ΔpCO2 is increased during a laparoscopic procedure not only during the entire time course of the surgery but additionally at the beginning of the operation is of particular interest. It is well known that in laparoscopic surgery CO2 is absorbed via the peritoneum and leads to increased systemic CO2 load, requiring increased minute ventilation.30,31 Pacilli et al. 18 showed in an excellent study that systemic absorption of CO2 in pediatric laparoscopic surgery is highest during the initial phase of surgery and plateaus at about 20–25 minutes. Their findings are in accordance with studies from adult patients.31–34 During the plateau phase, the additional pCO2 load absorbed by the peritoneum during laparoscopic surgery is believed to be between 10% and 30% of total pCO2e.33,34 When analyzing our data under these considerations we found the ΔpCO2 in the laparoscopic group on average to be 1.3-fold (22%) higher compared to the open group after 30 minutes (30–50 minutes) of surgery, but 2.3-fold (57%) higher before that (0–20 minutes) (Fig. 1D). This is in accordance with the observation made by Pacilli et al. 18 Analyzing these data, one must keep in mind that because pCO2e is subject to alteration via minute ventilation, the additional pCO2 load caused by absorption from the pneumoperitoneum in the setting described here is not reflected in the pCO2e but in the pCO2i. Therefore, neither the largely increased ΔpCO2 observed in the laparoscopic group during the initial phase of the operation nor the smaller increases during the later phases must necessarily represent a compromise of splanchnic perfusion compared with the open group but can be attributed to higher systemic pCO2 load from increased pCO2 absorption.
Given the generalized perception that induced pneumoperitoneum is ill defined compared with an open approach, these findings are rather remarkable. One interpretation of these data is that, at least in a noncomplex standardized operation such as simple appendectomy in otherwise healthy children of the age group presented here (5–17 years; mean, 10.7 years), the effect of pneumoperitoneum on the acid–base balance and splanchnic perfusion is less prominent compared with an open approach than generally perceived, particularly after the first 20–30 minutes of surgery. This would indeed be encouraging when considering laparoscopic surgery in a broader range of patients. Whether our findings are applicable to infants or children who suffer from specific conditions such as cancer or sepsis cannot be extrapolated from our current data.
There are several factors regarding our study that could potentially flaw our results. First, because laparoscopic appendectomy is performed more frequently in our hospital compared with open appendectomy, the control group (open group) is smaller than the laparoscopic group. However, we analyzed not only the means of the control group but also the individual data of each patient and found a homogeneous, comprehensible data set as indicated by the small SEM. Additionally, the groups were found to be homogeneous for age, gender and weight. Second, we included both perforated and negative appendectomies in the study. It is important that the decision for patient selection into the open or laparoscopic group was made because of the surgeon's preference independently from clinical suspicion for perforation. A true randomization, which we did not perform, would have been superior. However, when analyzing the individual data of each patient, we found similar data for the 3 patients who had perforated appendicitis and the 2 patients with negative appendectomies. Third, from our experiments we cannot determine with certainty what portion of the differences in the ΔpCO2 observed is provoked not by splanchnic hypoperfusion, but by the increases in systemic pCO2 caused by the pneumoperitoneum. The magnitude of this phenomenon is well documented for laparoscopic surgery in numerous studies and by itself justifies the extent of differences we see in our results, making a significant difference in splanchnic perfusion between the two groups even less likely. Finally, others have found pCO2e to overestimate the actual pCO2 identified on formal blood gas analysis in laparoscopy in children, possibly because of the pneumoperitoneum and CO2 absorption. 19 We therefore conducted additional pCO2a measurements for comparison. Despite selected dissimilarities, we typically found pCO2e to correlate well with pCO2a (Fig. 2). The discrepancies observed in our study regarding the correlation of pCO2e to pCO2a are most likely due to the fact that not all blood gas analyses were obtained at the exact planned time.
In summary, our data suggest that insufflating the peritoneum during laparoscopic appendectomy in older healthy children and adolescents does not have profound adverse effects on gastric mucosal microcirculation compared with the open procedure. Further research is needed in order to identify the true impact of pneumoperitoneum and laparoscopic surgery in infants and children during other laparoscopic procedures.
Footnotes
Acknowledgments
We would like to thank the parents for their cooperation and participation. This study was supported by the Friedrich-Baur Institute, Germany (to M.L.) and the German Academic Exchange Service (to M.B.).
Disclosure Statement
No competing financial interests exist for any of the authors. M.B. performed research, analyzed data, and wrote the article, J.H. and J.G. performed research, M.L. designed and performed research, analyzed data, and wrote the article, E.R.-M designed research, and O.M. and D.v.S. analyzed data and wrote the article.