
Abstract
Abstract
Background:
The aim of this report is to describe our surgical technique for robot-assisted laparoscopic bladder diverticulectomy. In this technique, methylene blue is instilled into the bladder to aid in intra-abdominal identification of the diverticular neck.
Subjects and Methods:
We retrospectively reviewed the records of patients who underwent robot-assisted bladder diverticulectomy by a single surgeon.
Results:
Between September 2008 and January 2011, 5 patients successfully underwent robot-assisted laparoscopic bladder diverticulectomy using 1% intravesical methylene blue. All cases were completed without intraoperative complication or need for open conversion. Mean operative time was 216 minutes, with a mean estimated blood loss of 45 mL. Patients were discharged 1–2 days following surgery. No patient experienced a perioperative complication.
Conclusions:
The robot-assisted approach for bladder diverticulectomy is a viable alternative to both open and laparoscopic surgery. The use of intravesical methylene blue greatly aids in identification of the diverticular neck during this procedure.
Introduction
Patients and Methods
Data collection
After Institutional Review Board approval, we retrospectively reviewed all RALBD cases performed by a single experienced robotic surgeon in our department (R.J.L.). Records were reviewed for clinical history, imaging results, intraoperative variables, and postoperative course.
Preoperative workup for all patients included cystoscopy and computed tomography urogram to estimate the size and location of the diverticulum, especially in regard to proximity to the ureters. Urodynamic studies were performed in 2 of the patients to confirm adequate detrusor contraction and to evaluate bladder outlet obstruction.
Study cohort
Patient 1
A 79-year-old man with a history of benign prostatic hyperplasia (BPH) who previously underwent transurethral microwave thermotherapy and transurethral resection of the prostate (TURP) presented with lower urinary tract symptoms and a post-void residual of 274 mL. Cystoscopy revealed a medium-to-large narrow neck diverticulum in the right hemitrigone.
Patient 2
A 48-year-old man presented with a history of BPH with decreased force of urine stream that was unimproved following transurethral microwave thermotherapy. The patient was referred to our center after a videourodynamics cystogram demonstrated a left-sided, posterior bladder diverticulum with a volume of approximately 900 mL. Urodynamic studies showed decreased detrusor activity, with a post-void residual of 950 mL requiring self-catheterization for voiding.
Patient 3
A 26-year-old woman presented with chronic urinary tract infections and hematuria for over 10 years. Cystoscopy showed a left-sided posterior bladder diverticulum with an estimated volume of 150 mL.
Patient 4
A 46-year-old man with BPH and a history of a weak stream and post-void dribbling presented with painless gross hematuria. Evaluation revealed a left-sided 5-cm bladder diverticulum with an estimated volume of 100 mL. During preoperative cystoscopy, a suspicious lesion within the diverticulum was biopsied and found to be consistent with inflammatory changes.
Patient 5
A 64-year-old man with a history of BPH following TURP presented with recurrent urinary tract infections, as well as incomplete voiding and occasional urgency. Computed tomography scan and voiding cystourethrogram demonstrated a posterior bladder diverticulum measuring approximately 6 cm in diameter with a residual volume of 600 mL.
Operative technique
Rigid cystoscopy is first performed to confirm the location of the diverticulum. A retrotrade ureterogram is then performed to visualize the course of the ureter in relation to the bladder diverticulum. A 6-French ureteral double-J stent is placed on the ipsilateral side to the diverticulum to aid in intraoperative ureter identification. A 16-French indwelling Foley catheter is then placed.
A Veress needle or the Hasson method is used to access the abdomen. Port placement mimics the configuration used in the da Vinci prostatectomy, with a 12-mm trocar placed supraumbilically serving as a camera port and an array of two or three 8-mm trocars placed in a W configuration. A 12-mm assistant port is also placed on the side ipsilateral to the diverticulum.
A transperitoneal approach is used to access the bladder. Because the pneumoperitoneum makes visualization of the diverticulum difficult, the bladder is distended by instilling 1% methylene blue solution into the 16-French indwelling catheter. When viewed intra-abdominally, the area of the diverticulum appears blue, thus aiding in identification of the diverticular neck (Fig. 1).
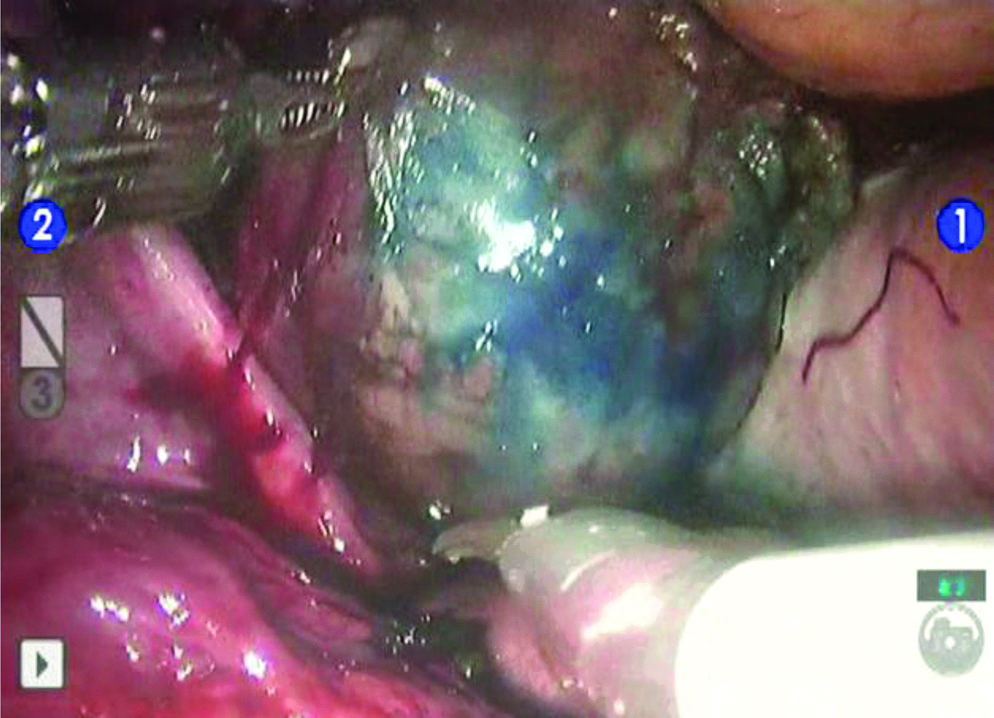
Intra-abdominal identification of a diverticulum aided by intravesical methylene blue.
Once the diverticulum is distended, the peritoneum is incised, peridiverticular structures are dissected, and the ureter is identified. This step is aided by prior ureteral stent placement. Once the diverticulum is mobilized and the diverticular neck is identified, it is incised with cold scissors (Fig. 2). The diverticulum is then completely excised and placed into a laparoscopic entrapment sac for later extraction.

Dissection of a bladder diverticulum.
The ureteral orifice and trigone are inspected prior to bladder closure. A two-layer closure is then performed with 2-0 polyglactin suture, with the first layer through the mucosa and detrusor, running and interlocking every third stitch. A second imbricating layer is then sawn. The bladder is then distended with 250 mL of saline to confirm a watertight closure.
Results
Between September 2008 and January 2011, one woman and four men underwent RALBD. The mean patient age was 52.6 years (range, 26–79 years), with a mean age-adjusted Charlson comorbidity index of 2.2. Patient characteristics are summarized in Table 1.
AACI, age-adjusted Charlson comorbidity index; BMI, body mass index; LUTS, lower urinary tract symptoms; NA, not available; PVR, post-void residual; UTI, urinary tract infection.
All five RALBD procedures were successfully performed without complication or need for open conversion. The mean operative time was 216 minutes (range, 175–265 minutes), with a mean estimated blood loss of 45 mL (range, 25–50 mL). In the immediate perioperative period, no patient experienced a complication, and 4 patients were discharged on the first postoperative day.
All of the patients with the exception of Patient 5 had cystography performed on postoperative Day 7 or 8, showing no evidence of leakage from the cystotomy closure site. After normal cystography, the Foley catheter was removed, and all patients were able to void without difficulty. Substantial improvements in post-void residual volumes were observed for the 3 patients for whom both pre- and postoperative data were available. Final pathologic evaluation of excised tissue showed inflammatory changes for 1 patient (Patient 4) and normal urothelium for the remainder of the patients.
Discussion
Various operative techniques have been described for the treatment of BD. Open bladder diverticulectomy was first described in the late 1800s and thus is well established and has been confirmed to have excellent outcomes and low complication rates. 3 Endoscopic procedures involving either fulgaration or diverticular neck resection were first described in the 1970s.5–8 Endoscopic management is generally reserved for patients who are poor candidates for invasive surgery or for patients with a small diverticulum found during a TURP.
Pneumovesicoscopic diverticulectomy has been also reported in the treatment of BD.9,10 In this technique, the bladder is insufflated with carbon dioxide. Under cystoscopic visual guidance, three laparoscopic trocars are placed percutaneously directly into the bladder. Intravesical resection of the diverticulum and defect closure then proceeds. The results with this approach are comparable with standard methods.
Parra et al. 12 were the first group to report transperitoneal laparoscopic diverticulectomy in 1992. This technique has seen widespread use and has evolved over the past two decades. A comparison between laparoscopic and open diverticulectomy in combination with TURP was made in 2002 by Porpoglia et al. 4 This report showed a smaller decrease in postoperative hemoglobin levels as well as a shorter length of hospitalization in the laparoscopic treatment group. Yet, laparoscopy remains a technically demanding modality for diverticulectomy, especially in suturing the bladder closure when compared with open surgery.
The robotic da Vinci Surgical System provides several advantages over conventional laparoscopy for performing bladder diverticulectomy.15–19 These include improved surgical dexterity with articulating instruments, three-dimensional visualization, and greater magnification. In 2007, Myer and Wagner 15 reported the first series of RALBD in 5 patients. This report demonstrated shorter operative times than conventional laparoscopy with surgical outcomes comparable to those reported for laparoscopic and open surgeries in the literature. In 2010, a review of RALBD case reports found that operative times ranged from 63 to 300 minutes compared with from 90 to 360 minutes for conventional laparoscopy. 16 Altunrende et al. 19 recently reported a series of 6 patients who successfully underwent RALBD, with a median operative time of 232 minutes, a median hospitalization of 3 days, and no significant postoperative complications. In this series, the authors successfully performed a ureteroneocystotomy with a refluxing anastomosis along with the diverticulectomy for a case of a ureter terminating within the diverticulum.
A consensus in the literature is that the most difficult aspect of RALBD is the identification of the diverticulum and dissection of the diverticular neck. Many BD are posterior, and oftentimes the pneumoperitoneum compresses the diverticulum, making it difficult to identify. Thus, various techniques have been proposed to ease the identification of BD. The first such technique to aide in dissection of the diverticulum during open surgery was described by Lerche in 1912, as noted by Esho and Cass. 20 In this technique, an early version of a balloon catheter was placed transurethrally into the diverticulum and inflated. A similar approach was taken by Myer and Wagner 15 in the first series of RALBD. These authors described using an angiographic occlusion balloon catheter for the distension of BD. Another technique involves the placement of a second Foley catheter with the balloon inflated to occlude the neck of the diverticulum and provide distension.14,21 The drawbacks to the dual-catheter approach include fitting the two catheters into a relatively narrow urethra and difficulty with the balloon becoming dislodged in large-mouthed diverticula.
Cystoscopic illumination is a technique that was described in the laparoscopic literature previously and was first used in RALBD by Macejko et al. 17 Altunrende et al. 19 also used this technique in their recent series of RALBD cases. The assistant first fills the bladder with saline, then removes the catheter, and introduces a flexible cystoscope. The laparoscope is dimmed, and the cystoscope enters the diverticulum and illuminates it, thus aiding in dissection.
In our series of 5 patients, BD were distended by injecting dilute methylene blue into the bladder via the 16-French catheter. Because a bladder diverticulum is a thin-walled protrusion of mucosa through the detrusor muscle, the instilled dye appears dark-blue in the area of the outpouching. It is this effect that aids the surgeon in the intra-abdominal identification of the diverticular neck (Fig. 1). We found this technique in combination with preoperative imaging and cystoscopy to be adequate in identifying the diverticulum, thus allowing for circumferential dissection. After undergoing our technique, most patients (4 of 5) were discharged on the first postoperative day. Immediate (<30-day) follow-up revealed no complications. However, at 3 months postoperatively, one patient (Patient 4) had recurrence of lower urinary tract symptoms and urinary retention. We suspect a neurogenic etiology for his symptoms, which will require confirmation with videourodynamics.
Conclusions
RALBD is an excellent alternative to open surgery and conventional laparoscopy for the management of BD. The robotic da Vinci Surgical System makes this procedure less technically demanding than conventional laparoscopy while still providing the benefits of minimally invasive surgery. The intravesical instillation of methylene blue greatly aids in identification of the diverticular neck during this procedure.
Footnotes
Disclosure Statement
R.J.L. has received compensation from Angiodynamics, Inc., for a scientific study, from Covidien, Inc., for a scientific study and as a consultant, from Cook Medical as a lecturer, from Intuitive Surgical as a proctor, and from Applied Medical as a lecturer. No competing financial interests exist for the other authors.