
Abstract
Abstract
Background:
The NiTi endoluminal Compression Anastomotic Clip (CAC™) 30 (NiTi CAC 30) (NiTi Alloys Technologies, Ltd., Netanya, Israel) is a new device with shape-memory characteristics. We aimed to investigate the safety and early surgical outcomes of NiTi CAC 30 for intestinal anastomosis in patients with gastrointestinal malignancy.
Subjects and Methods:
Fifty patients operated on with NiTi CAC 30 were matched for sex, age, body mass index, operation type (open versus laparoscopy), operation name, and anastomosis type with patients in a control group operated on with a stapling device between November 2009 and May 2010. Early clinical outcomes were investigated.
Results:
One misfired case of NiTi CAC 30 was excluded. Between the two groups, no significant differences were observed in demographics except for previous abdominal operation history. The results of early clinical outcomes were investigated, including operation time, estimated blood loss, time to first flatus, first defecation, and discharge, and complications. No differences were noted. Postoperatively, migration started in 1 patient between 3 and 5 days, 11 patients between 6 to 7 days, and 37 patients after 8 days. The expulsion of 31 cases occurred between 2 and 3 weeks, postoperatively. The NiTi CAC 30 was expulsed within 1 week in 4 patients and between 1 to 2 weeks in 8 patients. An expulsion occurred in 1 case at over 4 weeks. No problems related to early migration and expulsion were observed, and no anastomotic leakage and bleeding occurred.
Conclusions:
Intestinal anastomosis with the NiTi CAC 30 was safe and feasible without anastomotic leakage and reoperation compared with the stapling technique.
Introduction
The concept of compression anastomosis was introduced in 1826 4 and has been recently evolved as an NiTi endoluminal Compression Anastomotic Clip (CAC™) 30 (NiTi CAC 30) (NiTi Surgical Solutions, Ltd., Netanya, Israel), which in 2004 was approved by the U.S. Food and Drug Administration for use in intestinal anastomoses.
The new clip has several possible or anticipated advantages over other commercially available compression anastomotic devices. One such advantage is that no remnant foreign body is present. By cutting through the bowel wall, the clip allows the passage of bowel contents after the anastomosis is performed. It has also overcome other problems, such as a too narrow inner caliber, difficult application and assemblage, and high cost, the specific features of which made earlier anastomotic instruments less popular among surgeons.5,6
However, many surgeons continue to be uncertain about the safety and stability of NiTi CAC 30. The current report provides early surgical outcomes or short-term complications of patients with colorectal cancer in whose surgery the clip was applied for various types of gastrointestinal anastomosis.
Subjects and Methods
Study population
Data from all the patients who underwent intestinal anastomosis consecutively and in whom the NiTi CAC 30 was used between November 2009 and May 2010 in our department were collected, and the early outcomes were analyzed. Patients who underwent an emergency operation and those known to have an allergy to nickel, an intraabdominal abscess, a prolonged use of steroids, and uncontrolled diabetes mellitus were excluded from the present investigation. All the excluded patients had undergone stapled anastomosis.
We matched study group patients for sex, age, body mass index (BMI), operation type (open versus laparoscopy), operation name, and anastomosis type of NiTi CAC 30 with patients in a control group, who were anastomosed by a double stapling technique. Each group included 49 patients on whom only one expert performed the operations. We collected the data of the NiTi CAC 30 group prospectively and reviewed retrospectively. We searched the control group to match operation type, operation name, and anastomosis type to the NiTi CAC 30 group through medical records and reviewed retrospectively. To investigate surgical outcomes, we analyzed demographic data (age, sex, diagnosis, American Society of Anesthesiologists [ASA] classification, BMI, and previous abdominal surgery), perioperative factors (operating time, open or laparoscopic surgery, and estimated blood loss [EBL]), anastomosis type (small bowel–small bowel, small bowel–colon, or colon–colon), and postoperative outcomes (hospital stay length, postoperative hospital stay length, day of first flatus and defecation, clip expulsion day, clip migration day, and postoperative complications, including anastomotic site bleeding and leakage rates).
Typically, 500 mL of magnesium citrate was used for bowel preparation for right hemicolectomy. The patients for whom colon resection was planned (except for right hemicolectomy) were prepared with 4 L of polyethylene glycol bowel lavage solution just a day before the surgery. They received prophylactic antibiotics intravenously at the time of anesthesia induction and a double dosage of antibiotics postoperatively. The remaining patients were prepared by a 1-day fast before undergoing the operation.
The migration and expulsion of the clip were monitored by checking X-rays of kidney–ureter–bladder views on the consecutive second, fifth, and seventh day after surgery and at the first outpatient department visit (21±7 days after surgery). We investigated records of the second and/or third outpatient department visits in both the groups (duration of follow-up: NiTi CAC 30, 99.5±41.4 days after surgery; control, 77±36 days). The first diet was provided after the first flatus. Postoperative complications were classified based on the Clavien–Dindo classifications. 7 The present study was approved by the Institutional Review Board.
The clip
The NiTi CAC 30 is a double-ringed instrument with a diameter of 30 mm. It is constructed from a shape-memory alloy of nickel and titanium, which is temperature-dependent (Fig. 1). This biologically inert nickel-titanium alloy ring is shaped under high temperatures in a metallurgic oven and loses its rigidity when cooled in ice water at 0°C for 1 minute, thus becoming flexible with an opening angle of 30° (Fig. 2). 8 The alloy ring returns to its original closed shape when it senses a change in ambient temperature (Fig. 3). The cost of the NiTi CAC 30 is $186.80 (using a conversion rate of $1=1082 won), which is covered by national health insurance.
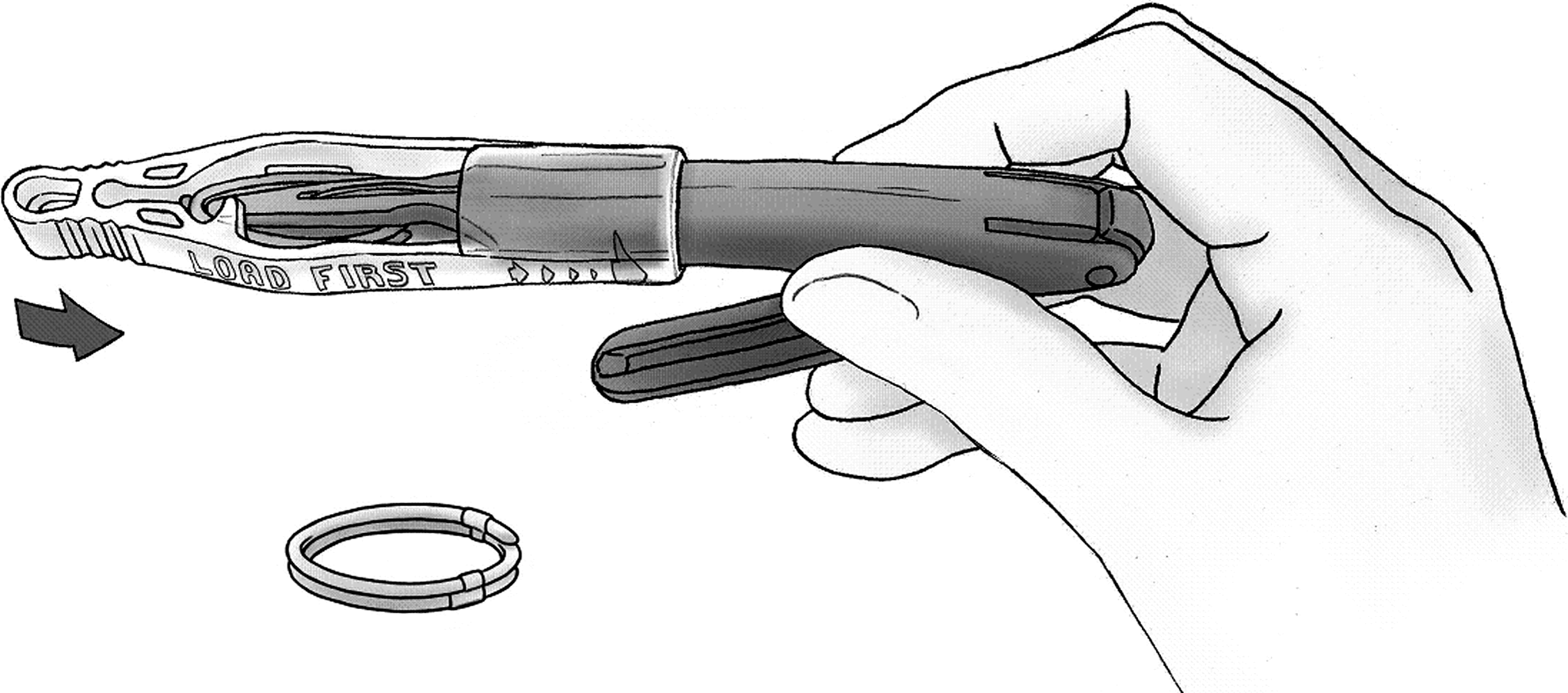
The NiTi CAC 30 is a double-ring instrument with temperature-dependent shape memory.

The NiTi CAC 30 is opened after being cooled in ice water.
The NiTi CAC 30 returns to its original closed shape when it senses a change in ambient temperature.
Surgical technique
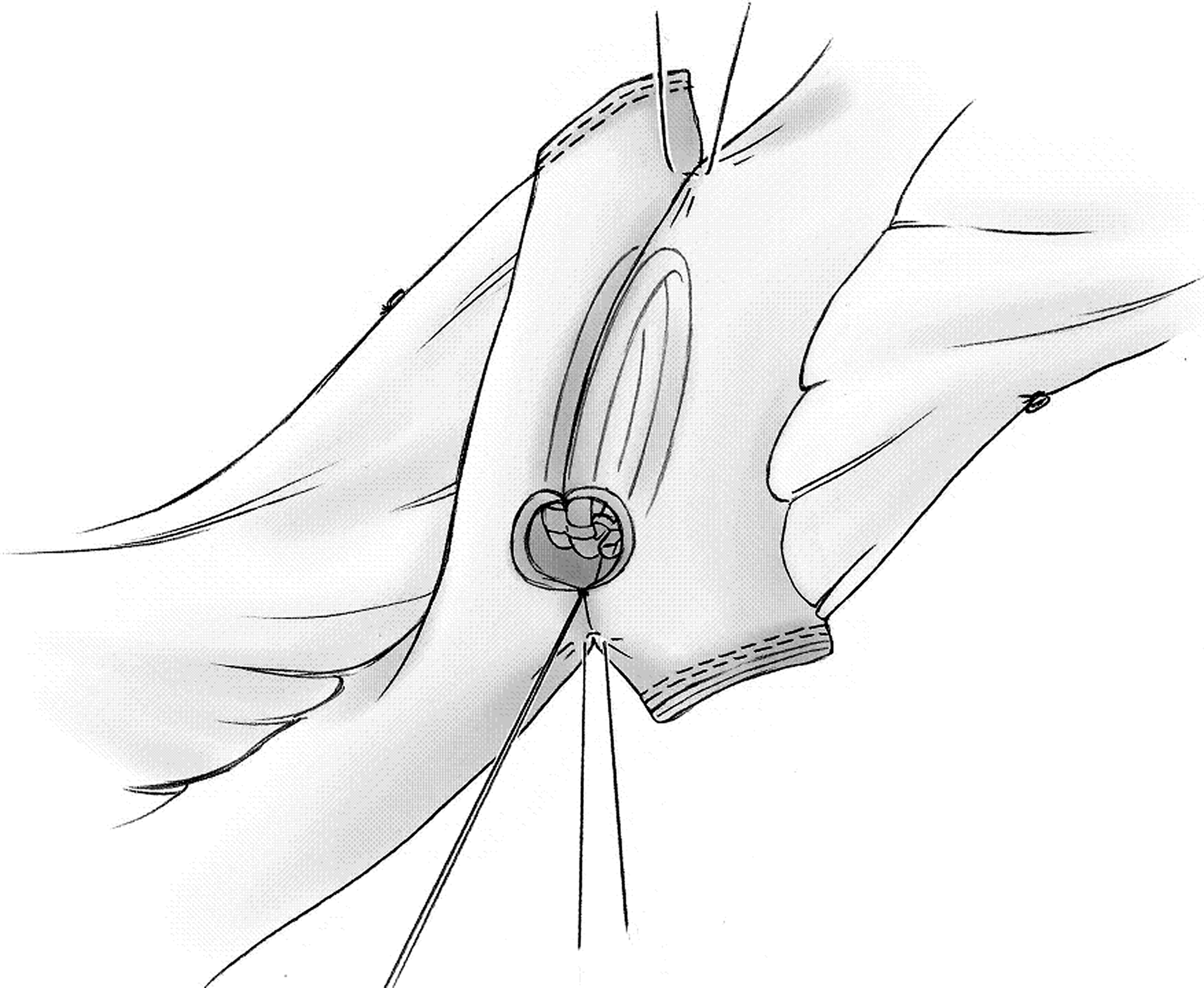
We prepared cold sterile saline (4–15°C) prior to the anastomotic procedure and positioned the two limbs of bowel that were to be anastomosed either isoperistaltic or retroperistaltic side-to-side, in a overlapping condition by a minimum of 5 cm. Two stay sutures were applied 1 cm from each edge. Two 0.5–0.7-cm-sized enterotomies were created just lateral to the antimesenteric border of both the bowel limbs (Fig. 4). The adjacent enterotomies were tied to each other by polyglactic acid 3-0 suture. The applier jaws were opened by pressing and releasing the lever of the NiTi CAC 30 (first click). The NiTi CAC 30 was inserted all the way into the enterotomies along the bowel axis, using the anchoring suture that had been placed earlier. Before applying the clip, we ensured that no mesentery of the bowel limbs was incorporated within the clip by placing two fingers between the bowel limbs (Fig. 5). The lever was pressed and released again to close the clip and clamp the tissue (second click). This position should be maintained for 30 seconds to enable complete compression of the tissue by the clip. With the third press and release of the lever (third click), the internal blade created a slit through the compressed tissue, and the fourth press and release freed the clip from the applicator (fourth click). After the device was withdrawn from the lumen, we ensured that the slit indicator was cut and split in half. The enterotomy was closed with an absorbable 3-0 suture. Suturing of the enterotomies started from the edge of the clip (opposite of the anchoring suture) and was carried out in two layers. After the enterotomies were closed, two or three reinforcing sutures were placed at the distal side of the clip to reduce tension.
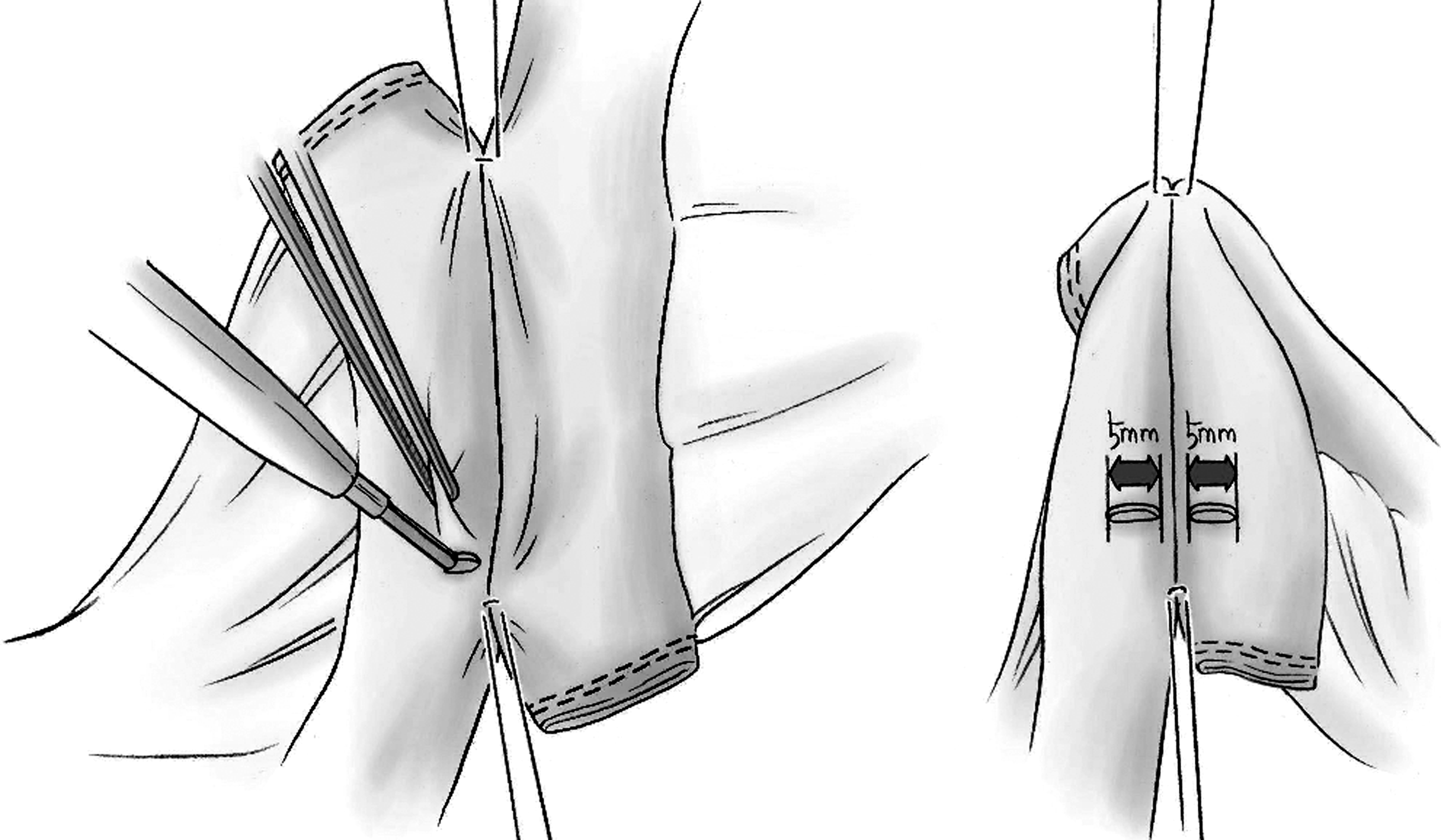
Two stay sutures were applied at 1 cm from both ends of the limb, and 0.5-cm-sized enterotomies were created just lateral to the antimesenteric border.
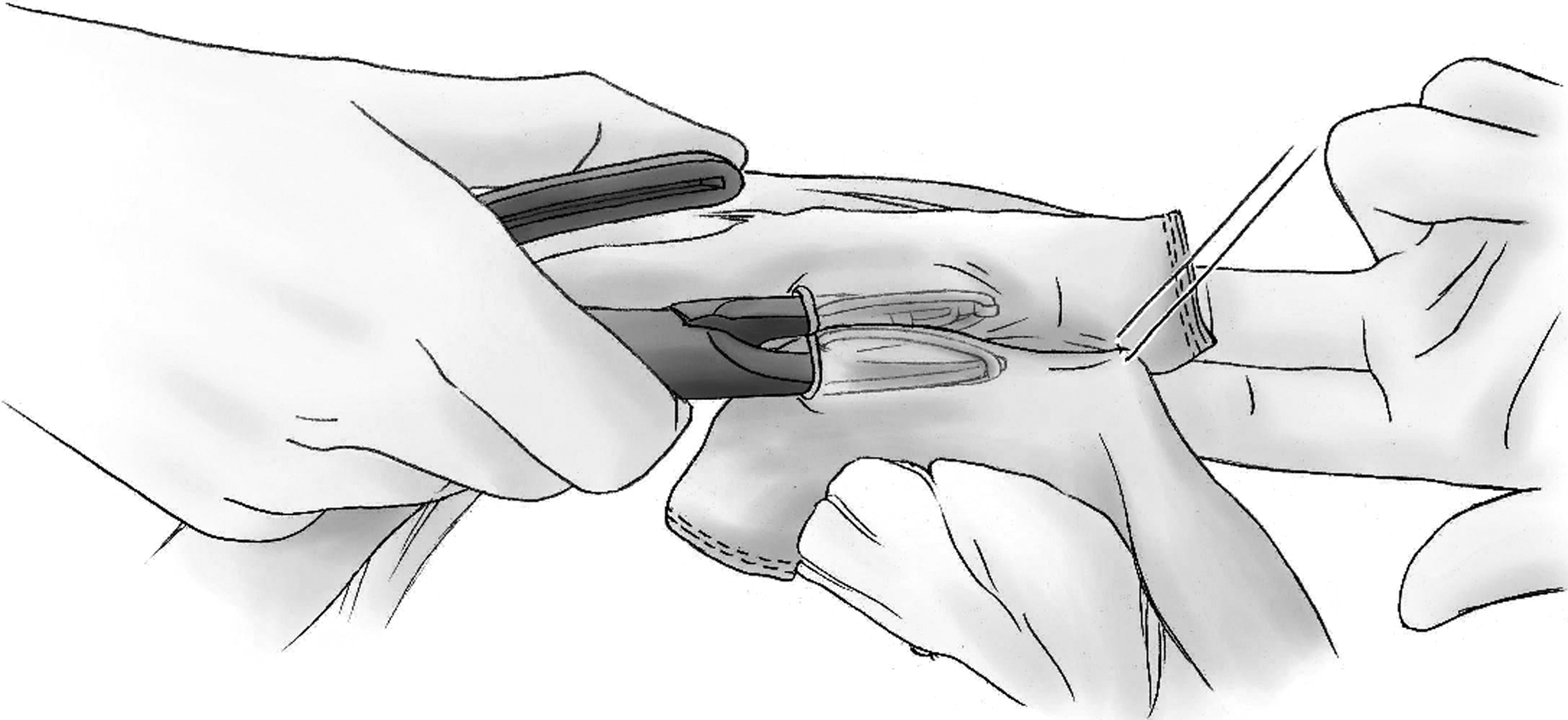
Before the second click, the surgeon should insert fingers to avoid grasping mesentery between the insides of the clip.
Statistics
The statistical analysis of quantitative variables with independent groups was performed with either the t test or the nonparametric Mann–Whitney U test. In the statistical analysis of categorical variables, Fisher's exact test was used. All the statistical analyses were carried out using SPSS version 17.0.
Results
Fifty patients who had undergone surgery using the NiTi CAC 30 (male:female ratio=25:25; mean age, 60±11 years; range, 36–78 years) met the study entry criteria. The mean ASA score was 1.6±0.5 (range, 1–3). One case of clip misfiring (2%) occurred during one colon–colon anastomosis procedure and was thus switched to stapled anastomosis.
The mean age and ASA score of the control group were 60.9±10.2 years (range, 39–81 years) and 1.7±0.5 (range, 1–3), respectively. The demographic data and diagnoses of the 49 patients who made up the final study group are given in Table 1. Gender, age (P=.741), BMI (P=.795), and ASA score (P=.313) showed no significant difference, although previous abdominal history was different (P=.004). The operative characteristics and early surgical outcomes including complications showed no significant differences (Tables 2–4). The results of mean operation time (P=.138), mean EBL (P=.465), operation types (P=.803), time to first flatus (P=.963), time to first defecation (P=.200), and time to discharge (P=.923) were not significant. In the NiTi CAC 30 group, 38 procedures were performed by open surgery and 11 by laparoscopic surgery. Forty control procedures were performed by open surgery. Sixteen cases were of small bowel–small bowel anastomoses (13 cases for ileostomy closure and 3 cases for small bowel segmental resection), 30 cases were of colon–small bowel anastomoses (28 cases for right hemicolectomy, 1 case for ileocecectomy, and 1 case for subtotal colectomy), and 3 cases were of colon–colon anastomoses (1 each for transverse colectomy, left hemicolectomy, and anterior resection). Three patients underwent multiple anastomoses (Table 2).
Synchronous colon cancer with sigmoid colon cancer (1 case).
Anastomosis recurrence of sigmoid colon cancer (1 case).
For ileostomy closure.
ASA, American Society of Anesthesiologists; GIST, gastrointestinal stromal tumor; NS, nonsignificant; SB, small bowel.
Simultaneously operated with cholecystectomy (1 case) and bladder resection (1 case).
Simultaneously operated with gastric wedge resection (1 case).
AR, anterior resection; EBL, estimated blood loss.
POD, length of postoperative hospital stay.
P=.610 for significance of difference in complication occurrence between groups.
Clavien–Dindo classification Grade I.
Clavien–Dindo classification Grade II. The patient was taken care of in the intensive care unit.
Clavien–Dindo classification Grade III. Fluid was drained percutaneously.
Clavien–Dindo classification Grade III. Reoperation was performed. There was no definite evidence of anastomotic leakage.
Clip migration began between 3 and 5 days postoperatively in 1 patient, between 6 to 7 days in 11 patients, and after 8 days in 37 patients. Expulsion of the clip was confirmed in 44 patients: ≤7 days postoperatively in 4 patients, from 8 to 14 days in 8 patients, between 15 to 21 days in 31 patients, and over 1 month after surgery in 1 patient. The X-ray examination was not done in 5 patients, and no expulsion data were available. We investigated their X-ray films during the third outpatient department visits. There was no remaining NiTi CAC 30 on X-ray, and in none of the patients was expulsion of device recognized. However, no expulsion-associated complaints and complications occurred among them (Table 3). During defecation, 47 patients did not notice the expulsion of the clip, 1 patient felt slight pain accompanied by slight bleeding, and only 1 patient found the clip.
In the NiTi CAC 30 group, complications were reported in 11 cases. Seven patients had postoperative ileus, 2 had wound seroma, 1 had chyle leakage, and 1 had abdominal pain, which was thought to be related to the clip (Table 4). Postoperative ileus occurred in 4 patients who underwent ileostomy closure, in 1 who had small bowel segmental resection, in 1 who had right hemicolectomy, and in 1 who underwent concomitant right hemicolectomy and anterior resection. All of those recovered with no sequelae after conservative treatment. Two of the 11 complications were thought to be related to the clip. One patient who had sudden abdominal pain at 14 days postoperatively showed a small amount of fluid collection and inflammatory change around the anastomotic site on abdominopelvic computed tomography. At the time of re-admission, he had no fever or leukocytosis. The patient received antibiotic therapy for 3 days and started his diet from water on the fifth day of hospitalization. He was discharged on the eighth day of hospitalization after initiation of soft diet. One patient who had postoperative ileus for 1 week after right hemicolectomy showed a dilated bowel just proximal to the anastomotic site on abdominal X-rays. Improvement was seen in the ileus on the fourth day of rehospitalization, and the patient was discharged on the eighth day of hospitalization.
No leakage or bleeding from the anastomotic site or mortality was observed.
In the control group, complications were reported in 8 cases. Three patients had postoperative ileus, occurring in patients who underwent ileostomy closure, concomitant small bowel segmental resection and anterior resection, and right hemicolectomy, respectively. One of them had wound seroma, one had abdominal pain, and one had intraabdominal fluid collection, which was drained percutaneously. One patient was treated at the intensive care unit because of the possibility of occurrence of intraabdominal bleeding, and subsequently the patient recovered without any intervention. One patient receiving a right hemicolectomy showing symptoms of peritonitis was suspected of having anastomosis leakage, and thus exploratory surgery was performed. A small amount of turbid fluid collection was seen in the abdominal cavity, but no definite defect of anastomosis was observed (Table 4).
Discussion
The mechanism of the NiTi CAC 30 is similar to that of other compression anastomotic devices. The intestinal walls are placed, pressed, and clamped between coils of the ring, and steady pressure creates gradual and controlled necrosis of a part of the intestine within the area defined by the coil's perimeter, while the external edges of this area become sealed, thus forming an anastomosis. 8 The NiTi CAC 30, which becomes detached from the anastomotic site, is eventually expelled from the body. 8 One important potential benefit of the NiTi CAC 30 is that there is no residual foreign body.
Stapling devices have several advantages, such as quick application and minimal tissue reaction, and there has been increasing standardization of the technique. 9 One Cochrane review demonstrated that anastomosis with a stapler was associated with less radiologic and clinical dehiscence in ileocolonic anastomosis than hand-sewn methods, and it had a similar rate of anastomotic leak in colon and rectal anastomoses. 9 A stapling technique, however, leaves a permanent foreign body that may be related with anastomotic recurrence of cancer and inflammatory bowel disease at the site of anastomosis.10,11 In addition, the crossing line of the staples in the double stapling technique is one of the weak points of anastomosis, thus posing a risk for ischemia and leakage. 8
Sutureless anastomoses, such as compression anastomotic devices and staplers, have been found to be superior to conventional anastomoses in terms of operative time, postoperative complications, and return of bowel function.12–14 Compared with staplers, the NiTi CAC 30 has several potential merits, such as creation of a uniform size of lumen (3 cm), no crossing line of multiple staples, no remnant foreign body, and no bleeding from the anastomosis because there is no cutting of any vessels around the anastomotic site. The early postoperative course of anastomosis was not different from that of the double stapling technique.
In spite of the advantages of the NiTi CAC 30 in the setting of intestinal anastomosis in gastrointestinal surgery, the device is still not widely accepted because many surgeons continue to be uncertain about the safety of an anastomosis that is created without any sutures or staples. No anastomotic leakage occurred in any of the 49 cases reported in the current series. We were also able to confirm the generally accepted estimation of the NiTi CAC 30 detachment occurring between 2 and 3 weeks after the operation. 7 Moreover, the 4 patients with an early expulsion (within 1 week) of the clip did not demonstrate any related complications. The complications that were documented in 11 patients were mild and could be managed by conservative treatment. The only two cases with postoperative ileus and abdominal pain were thought to be related to the NiTi CAC 30. Even though no statistical significance of incidence was observed, the control group needed intervention and reoperation to solve the complications.
This series also showed the efficacious implementation of the NiTi CAC 30 for various types of intestinal anastomoses, specifically, small bowel–small bowel, small bowel–colon, and colon–colon. In experienced hands, we believe that an ileo-ileostomy for an ileostomy closure and ileo-colostomy for performing a right hemicolectomy are additional procedures that can benefit from the associated advantages of the NiTi CAC 30. We needed less adhesiolysis compared with the stapled technique for performing ileostomy closure, and the anastomoses were easily performed despite the unequal size of the ileal edges. We also found that the new device could provide either an isoperistaltic or a retroperistaltic side-to-side anastomosis in right hemicolectomies without the disadvantages of the crossing line of staples.
This study has a few limitations, such as its small sample size, that it was observational, and that it was not a randomized and prospective study.
Some words of caution are warranted with regard to the application of the NiTi CAC 30 in setting of surgery for colorectal cancer. The surgeon should be aware that it is possible for the mesentery of a narrow bowel to be incorporated between the clips and that this area may become an ischemic point of an anastomosis. This problem can be solved by introducing a finger behind each edge of the two parts that will be joined to ensure that they are free of mesentery while applying the NiTi CAC 30. Closing the enterotomy is a cumbersome and time-consuming procedures. If it is not sutured correctly, there may be leakage or retention of the clip inside the lumen for a long time. These problems will be solved with launch of the new device.
In conclusion, intestinal anastomosis with the NiTi CAC 30 was safe and effective, ranging from the small bowel to the colon. The device was able to provide a uniform size for the lumen and obviate the sequelae of residual foreign bodies and crossing line of staples. Early detachment of the clip caused no problems. The technique for applying the clip is not difficult, but a certain degree of skill on the part of the surgeon is needed. The spectrum of uses of the NiTi CAC 30 in gastrointestinal surgery is still evolving, and further studies with a larger patient population and longer follow-up are warranted.
Footnotes
Acknowledgments
We thank Esther Eshkol for editorial assistance.
Disclosure Statement
No competing financial interests exist.