
Abstract
Abstract
Introduction:
Schwannomas are rare tumors and are exceptionally retroperitoneal. In the event of clinical signs or uncertainty in the diagnosis, their removal is justified. A risk of neoplastic transformation exists.
Patients and Methods:
Three patients had a retroperitoneal schwannoma located next to or under the sacral promontory. A double approach using an initial retroperitoneoscopy and an iliac abdominal incision had been decided preoperatively. This approach has not been described previously in the medical literature.
Results:
The double approach enabled the complete removal of tumors in all patients. The iliac incision, described within, enabled the removal of the tumors despite major attachments and difficulties in exposure, due to the tumors' distal situations.
Conclusion:
A double approach by retroperitoneoscopy and laparotomy can enable removal of difficult low-seated retroperitoneal schwannomas without increasing intraoperative risk or perioperative morbidity.
Introduction
This approach has not been described previously in the medical literature. A systematic review of the PubMed database has been done using the keywords “retroperitoneal schwannoma,” “retoperitoneal tumor,” “double approach,” and “surgical technique,” and no occurrence has shown up for the last 30 years. We describe for the encountered cases the surgical technique that was used and the available data on retroperitoneal schwannomas in the literature.
Patients and Methods
This is a retrospective study concerning 3 patients who underwent surgery in the Department of Urology at the University Hospital of Rouen, Rouen, France, between 2006 and 2010. All patients had cases of low-seated retroperitoneal schwannomas that were localized next to or under the sacral promontory (Table 1). In each case, a risk of regional compression or clinical symptoms that were thought to be related to the tumor justified the surgery. The double surgical approach was decided before the beginning of the surgery in each case.
Case 1
In a 60-year-old male patient, abdominal sonography followed by computed tomography (CT) (Fig. 1) for abdominal and thorax trauma discovered a 70-mm oval tumor, localized next to the lumbar vertebrae, at the L5–S1 right foramen. The sacral promontory limited the tumor cranially; the psoas muscle and the primitive iliac vein limited it anteriorly. The patient presented no symptoms. He had a history of appendicular peritonitis. He underwent magnetic resonance imaging (MRI) (Figs. 2 and 3), which showed a heterogeneous mass of 70 mm, contrast-enhanced in its periphery, hyperintense in T1 sequence, with a hypointense center. This aspect was suggestive of a diagnosis of retroperitoneal schwannoma. Because of the risk of regional compression and neoplastic transformation, surgical removal was decided, using a double retroperitoneoscopic and open approach. Operative time was 125 minutes. Blood loss was less than 50 mL. No early postoperative complications were noted. The patient was discharged on postoperative day 4. At 3 months of follow-up, no sign of recurrence was noted on control CT scan. Intense pain was still present in the L5 region, requiring treatment by pregabalin, as well as a sensation of warm leg. Pain gradually subsided over time.

Patient 1. On injected computed tomography scan, the tumor is limited anteriorly by the psoas muscle, posteriorly by the sacral promontory, and medially by the iliac vessels. Hypodensity in the center is suggestive of a central cystic part.
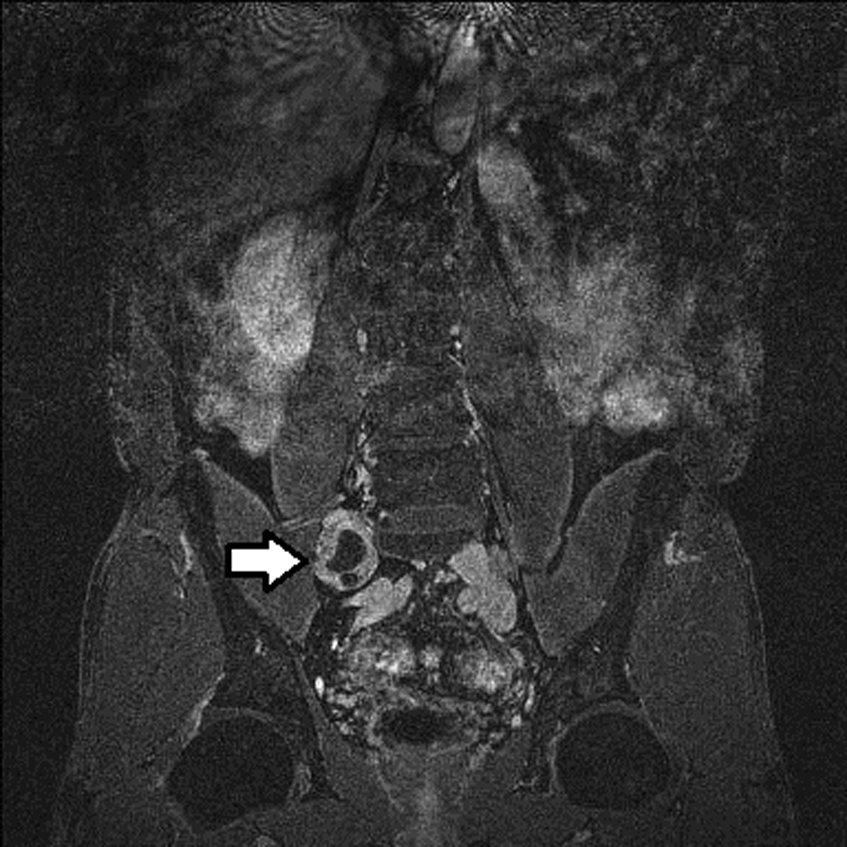
Patient 1. Magnetic resonance imaging in T2 sequence confirms the liquid center of the tumor, localized among the sacrum, psoas muscle, and iliac vessels.

Patient 1. Magnetic resonance imaging in contrast-enhanced T1 sequence.
Case 2
In a 60-year-old female patient, imaging was done for the investigation of intense lumbar back pain, without obvious radicular localization. Spinal MRI, with T1, T2, contrast-enhanced T1, and STIR sequences, found distally from the sacral promontory, behind the iliac vessel, medial from the psoas muscle, a perfectly oval 20-mm mass, characterized by a mixed MRI signal, with an important, strongly contrast-enhanced central zone, of tissular aspect, and a more peripheral zone, of liquid aspect. A diagnosis of cystic schwannoma was suggested. Surgical removal was effected. Operative time was 120 minutes. The patient did not require blood transfusion. She was discharged on postoperative day 6. At the 12-month follow-up, no recurrence was found on control CT scans. Pain has completely disappeared.
Case 3
A 55-year-old female patient presented with ongoing sciatic pain for 3 years. MRI and CT imaging, done to explore the symptom, showed a 64-×38-mm retroperitoneal mass of tissular aspect after contrast injection. It was low-seated, immediately beneath the sacral promontory to the left of the lumbar column. Complete hormonal testings were done to exclude an adrenal origin and were negative. Surgical removal was decided as a means of acquiring a definite histological diagnosis. Operating time was 150 minutes, and no transfusion was needed. The patient was discharged on postoperative day 4. No recurrence was found on control CT scan at the 6-month follow up. Initial pain had disappeared. Left lumbar hypoesthesia persisted after surgery.
Procedure
The following technique has been used for all cases:
Under general anesthesia, the patient was prone, on his or her side contralateral to the lesion (Fig. 4).
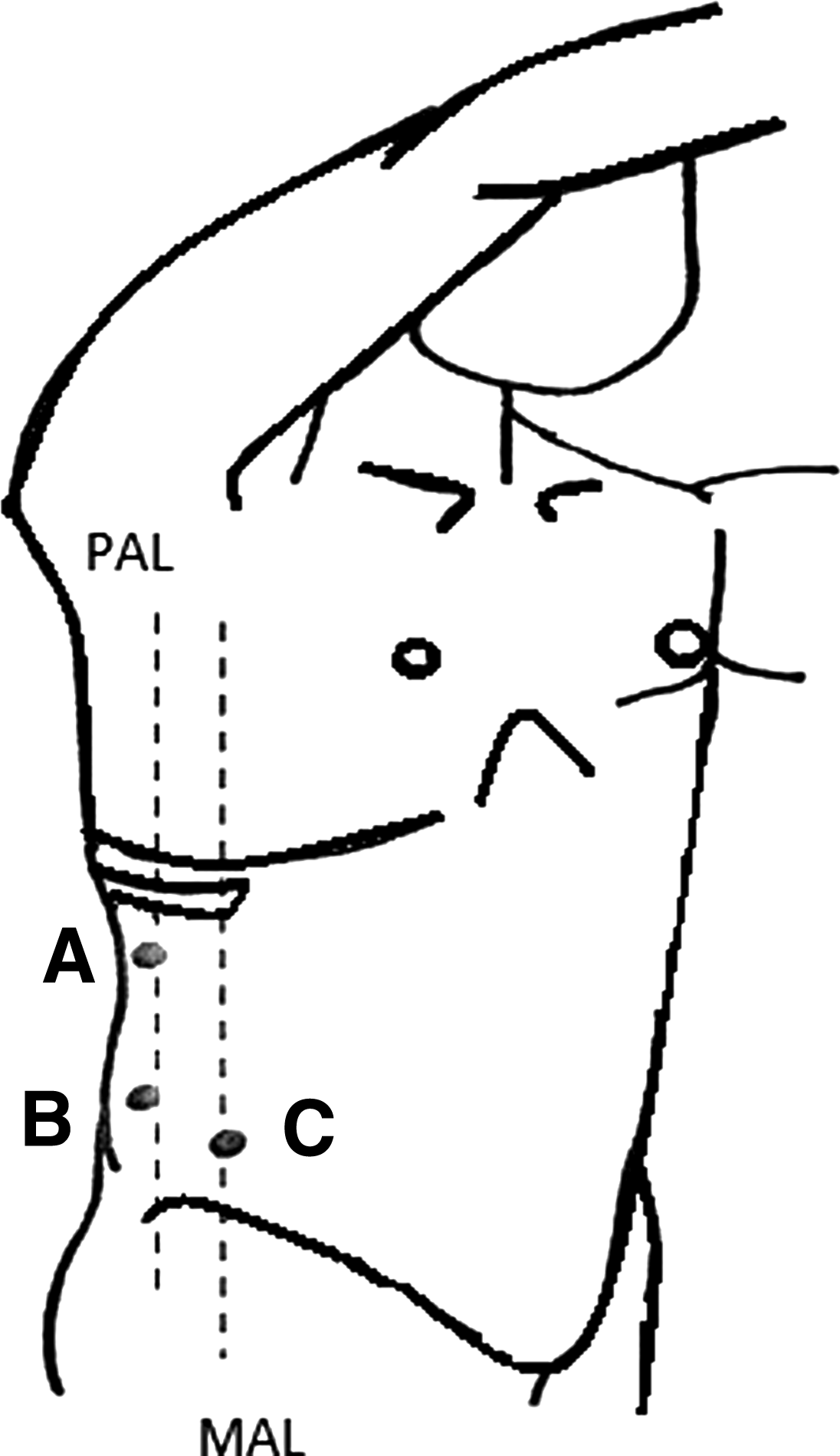
Initial retroperitoneoscopy installation: The patient is prone on the homolateral contralateral side. A, trocar A, 12 mm; B, trocar B, 10 mm (camera); C, trocar C, 5 mm. MAL, mean axillary line; PAL, posterior axillary line. Based on Lefi et al. 20
Initial retroperitoneoscopy was effected through a 12-mm screwed trocar that was inserted under the 12th rib, a 10-mm trocar right next to the iliac crest, and a 5-mm trocar in the iliac fossa. A 0° lens camera was used through the 10-mm trocar after the peritoneum was pushed back manually. Retroperitoneal dissection enabled direct visualization of the ipsilateral ureter, iliac vessels, and the lower portion of the inferior vena cava. Dissection was limited by overhanging iliac psoas muscle (2 cases out of the 3) and by intense adhesions between the tumor and the posterior plane (1 case out of the 3).
To complete the dissection, an ipsilateral iliac incision was made of limited length (8 cm) and that stayed strictly retroperitoneal. The psoas muscle was reclined with great effort using retractors, in order to expose the tumor. The tumor was progressively dissected and freed from adjacent structures, to which it was always strongly attached: Internal iliac vein, coxal and vertebral periost, and other nervous and vascular structures. Deep adhesions were difficult to free and required great caution. In all cases, the tumor was found to emanate from a nervous structure, which was severed in order to extract the tumor and send it for histopathological analysis.
In Patient 3's case, surgery was immediately preceded by a cystoscopy, which enabled the setting of a 7-French ureteral stent in the ureter that was closely attached to the tumor on preoperative imagery.
No intraoperative incidents were noted. Mean operative time was 131 minutes. Mean hospital stay was 4.6 days.
Discussion
Schwannomas are rare tumors that originate from the Schwann cell, which produces neural myelin. Most frequent sites include head and neck, 1 in particular the 8th neural pair. 2 The retroperitoneal site is very rare, with an incidence of 2 cases for 1.5 million hospital admissions in France.2,3 Between 0.7% and 3% of schwannomas are of retroperitoneal localization.2,4,5 The schwannoma incidence is much higher in patients affected by Van Recklingshausen's disease.6,7 Malignant cases are only found in cases affected by this disease.
The review of the medical literature yielded mostly short series (fewer than 5 cases), with tumors sizes generally larger than those of our series: Mean sizes of 10.4 cm (2–20 cm) among 17 patients.7–11 No case was found of surgical removal of schwannomas localized under the sacral promontory. Most affected sites were in superior areas: Usually inside or next to a perinephric space or next to the duodenopancreatic region. Very strong attachment to adjacent structures was often found, with the vertebral column, sacrum, and kidney. This sometimes mimicked the behavior of malignant tumors, with genuine tissue erosion, visible on preoperative imagery.7,10,12 Removals have been described by open or laparoscopic approaches.
Schwannomas are usually discovered on imaging (sonography, CT scan, MRI) done for unrelated symptoms: Back pain, abdominal pain, and gastrointestinal issues.7,13,14 These varied symptoms explain the frequent delay to diagnosis and thus why tumors are usually diagnosed at advanced stages, with sizes larger than what we found here.7,8 Schwannomas are usually described on imaging exams as well-limited masses, sometimes within a pseudocapsule. They are of homogeneous aspect when they are small but of a more heterogeneous aspect when they acquire a larger size, due to intratumoral bleeding or necrosis. 15 MRI is a useful tool, as it gives a strong diagnostic suspicion: In T1 sequence lesions are isointense, and in T2 sequence they are usually hyperintense. They are strongly enhanced after contrast injection.12,16 Up to 66% of ancient schwannomas appear in some form of cystic transformation, with a liquid component. 17 Diagnosis by imaging is often unsure: One-third of schwannoma diagnoses are made on histopathological findings.
Standard treatment is surgical removal. The removal must be complete with tumor-free margins, in order to prevent recurrence. 7 During the last decade, authors have described removals of retroperitoneal schwannomas by laparoscopic approaches.9,18,19 However, tumors removed in such a manner were all localized cranially to the sacral promontory, in the lumbar or iliac areas, and were all of large sizes. In our series, tumors were of sizes of less than 70 mm, localized in the pelvis, between the psoas muscle and the iliac vessels. The initial retroperitoneoscopic approach granted the surgeon an extraperitoneal dissection, without the usual intraabdominal laparoscopic risks (gastrointestinal tract injury, intraabdominal adhesions, postoperative gastrointestinal paralysis). Open surgery was thus limited to the final tumor removal phase. The retroperitoneoscopy-only approach does not grant sufficient room to retract the psoas muscle and expose with sufficient security the deep portion of the tumor because of the overhanging muscle. Ipsilateral iliac incision was limited in size because the vast majority of the dissection has already been done by retroperitoneoscopy, which granted safe vascular control on most of the tumor, especially concerning the deep portion, which is difficult to access using traditional open surgery. This enabled the complete removal of the tumor.
No early or late complications have been found in our series. Every tumor removal was complete, and no recurrence has been noted in the patients' follow-up.
Conclusions
The removal of lumbar schwannomas by retroperitoneoscopy had already been described. In the case of low-seated tumors, especially under the sacral promontory, in the event of intense local attachments or if the dissection is rendered hazardous or impossible because of the overhanging psoas muscle, a double approach by an initial retroperitoneoscopy followed by an open approach is possible, assisting the dissection by a limited incision, with no additional morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.