
Abstract
Abstract
Background:
The aim of the current study is to compare the results after partial and complete splenic flexure mobilization (SFM).
Subjects and Methods:
The records of laparoscopic and hand-assisted laparoscopic procedures for primary rectal tumor patients were abstracted from a prospectively designed database. The phrenicocolic and splenocolic ligaments were divided via a four-trocar technique in the partial SFM group, and dissection was continued with the separation of gastrocolic and pancreaticomesocolic attachments via a five-trocar procedure in the complete SFM group. The following data were compared between the groups: Demographics, intra- and postoperative information, and pathological features.
Results:
In total, 122 cases (77 [63.1%] male, 58.2±13.2 years old) who underwent a partial (n=36, 29.5%) or a complete (n=86, 70.5%) SFM were included. Reservoir creation (48.8% versus 19.4%, P=.003) was more common and conversion (8.1% versus 22.2%, P=.039) was less frequent in the complete SFM group, but there were significantly more T4 tumors in the partial group (16.7% versus 2.3%, P=.008). Demographics, other intra- and postoperative parameters, and pathological features were identical.
Conclusions:
In our study, complete SFM decreased conversion rates, but this finding may be related to the higher rate of T4 tumors in the partial SFM group. Complete SFM assures an increase in reservoir creation in patients receiving a low anterior resection. Because other parameters are identical, the decision for the level of SFM is better left to the surgeon in cases undergoing a low anterior resection, but complete SFM may be preferred in cases who are candidates for a reservoir formation.
Introduction
On the other hand, the definition of SFM may not be homogeneous in different studies because the length of proximal remnant is highly likely related to dissection of the splenocolic, phrenocolic, gastrocolic, or pancreaticomesocolic ligaments or attachments, but the border of the mobilization has not clearly been determined in most analyses. The principal goal in the current study is to assess the necessity of SFM in patients with rectal tumors who are candidates for a low anterior resection. In addition, we have also aimed to precisely define the levels of dissection in patients undergoing partial and complete SFM.
Subjects and Methods
Our Institutional Review Board approved the design and content of the study prior to data abstraction (protocol number B104ISM4340029/1009/57). Data from patients who had undergone laparoscopic or hand-assisted laparoscopic resections for premalignant and malignant lesions located at the rectum since 2006 were abstracted from a prospectively designed database. Those who had undergone an operation for a recurrent cancer or a tumor located in the sigmoid or rectosigmoid colon were excluded as other tumors rather than adenocarcinomas or dysplastic polyps in order to homogenize the information. In addition, those who had undergone an abdominoperineal resection for a rectal cancer were also excluded because SFM is generally unnecessary for these cases. Patients were divided in two groups according to the types of the procedure. The cases were assigned regarding to the level (partial or complete) of SFM.
Surgical procedures
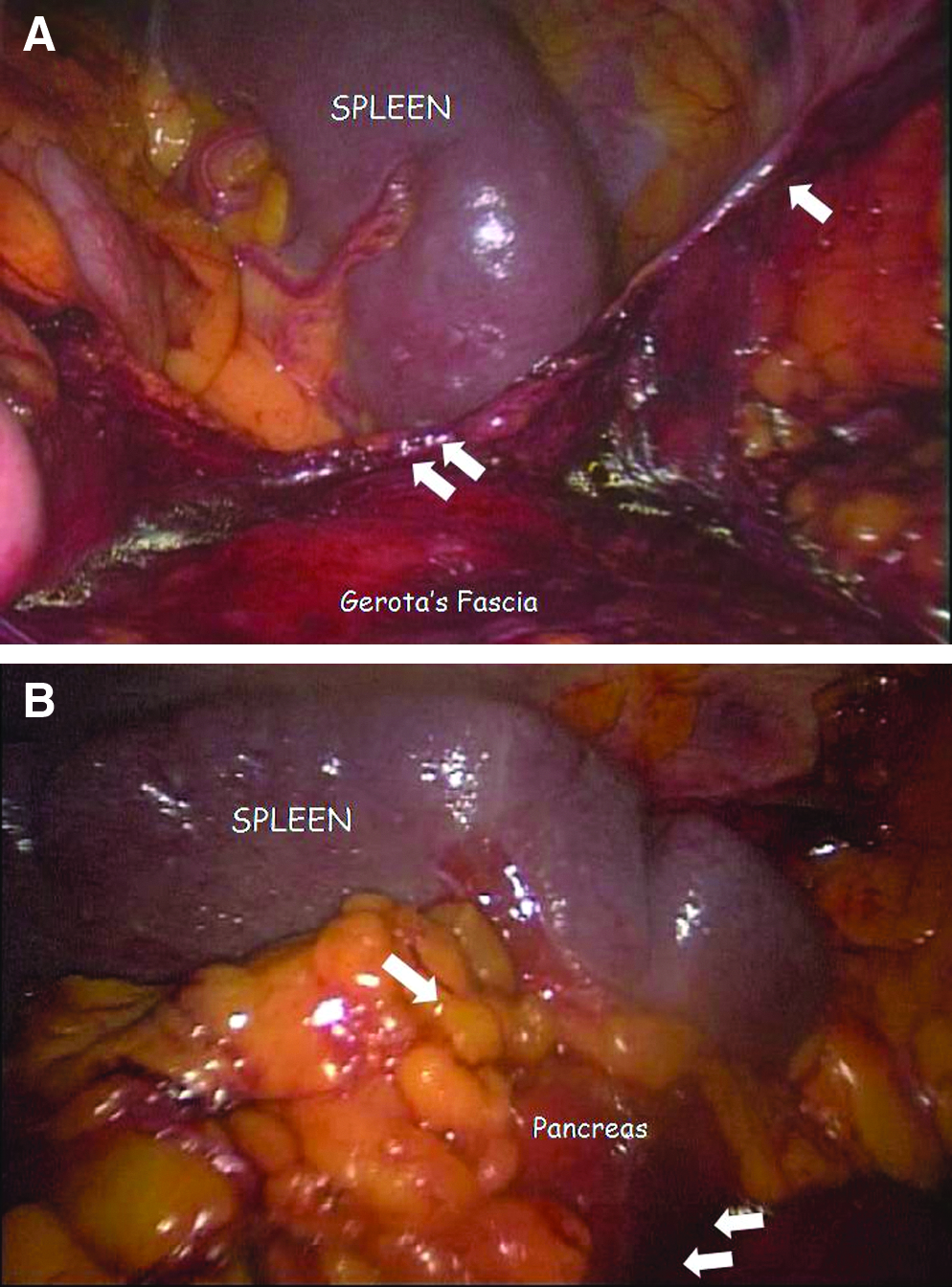
Since 2006, all patients with tumors at the rectum have been candidates for laparoscopic surgery at our department except those who had a recurrent cancer. A hand-assisted technique was generally preferred for rectal cancers as described in our previous study, but a laparoscopic technique has been chosen in selected cases. 11 A medial-to-lateral approach was followed, and high ligation of inferior mesenteric artery was routinely performed in our practice. 8 The retroperitoneal dissection was continued over Gerota's fascia until Toldt's fascia and the pancreas were seen at the lateral and superior borders of the dissection, respectively. After the dissection of Toldt's fascia and mobilization of the sigmoid and descending colon, the phrenicocolic and splenocolic ligaments were sealed and divided until the body of the spleen was clearly demonstrated (partial mobilization) (Fig. 1). The operation was completed via four trocars in the partial SFM group, but we preferred to insert an additional trocar between the umbilicus and xiphoid process and moved the camera to this port while performing a complete SFM, which was more commonly performed in recent years. In this technique, in addition to dissected ligaments during partial SFM, gastrocolic and pancreaticomesocolic attachments were also divided (Fig. 1). The anastomoses were performed intracorporally and always secured with a diverting ileostomy. In patients with tumors very close to the dentate line, an intersphincteric resection combined with a handsewn coloanal anastomosis was preferred.
The following data were analyzed for the two groups: Demographics, application of neoadjuvant chemoradiation therapy, intraoperative data (operation time, amount of bleeding, presence of synchronous metastasectomy, and conversion to open surgery), length of hospital stay, the total requirement and amount of transfusion during the perioperative period, complications, necessity of a reoperation, 30-day mortality, and pathological information (T stage, length of the specimen, number of harvested lymph nodes, and distal margin).
Statistical analysis
Data were analyzed by using SPSS version 15.0 for Windows. Results were given as percentages, mean and standard deviations, or median and ranges. Quantitative and qualitative variables were compared with Student's t test and chi squared (Pearson's or Fisher's exact) test, respectively. A P value of <.05 was considered significant.
Results
After the exclusion of patients with recurrent or colon cancers or those who underwent abdominoperineal resection, in total, 122 rectal cancer cases (77 [63.1%] male; mean age, 58.2±13.2 years) who underwent a low anterior resection for an adenocarcinoma (n=118, 96.7%) or dysplastic polyp (n=4, 3.3%) were included to the study. Complete SFM was performed in 86 (70.5%) cases. Demographics, the status of neoadjuvant chemoradiation therapy, and most intraoperative data, including operation time, amount of bleeding, and number of cases who underwent synchronous metastasectomy, were identical between the groups (Table 1). However, the incidence of reservoir creation was significantly higher in patients treated with a complete SFM (Table 1). In addition, the conversion rate was significantly higher in the partial SFM group; reasons for conversion were as follows: Clinical T4 tumor (n=6 [16.7%] in the partial and 2 [2.3%] in the complete group, respectively; P=.008), technical difficulties (n=1 [2.8%] in the partial and 1 [1.2%] in the complete group, respectively; P=.505), tumor perforation (n=0 in the partial and 2 [2.3%] in the complete group, respectively; P=.999), anatomic restrictions (n=1 [2.8%] in the partial and 1 [1.2%] in the complete group, respectively; P=.505), and severe adhesions (n=0 in the partial and 1 [1.2%] in the complete group, respectively; P=.999). The postoperative data and pathological information were identical between the groups (Tables 2 and 3).
Data are mean±standard deviation values or median (and ranges).
The actual numbers of the patients (stated in parentheses) were used for the comparisons because of missed information.
Data are mean±standard deviation values or median (and ranges).
Data are mean±standard deviation values or median (and ranges).
T0 includes dysplastic polyps and tumors that had completely responded to neoadjuvant chemoradiation therapy.
A radial margin of <1 mm was accepted to be positive, and actual numbers of the patients (stated in parentheses) were used for the comparisons because of missed information.
Discussion
Routine SFM is widely considered to be an essential part of low anterior resections in order to perform an oncologic resection and to achieve a safe, tension-free anastomosis.9,12–15 A recent review has revealed that SFM reduces the leakage rate in patients who underwent a low anterior resection for rectal cancer. 10 In contrast, SFM is a difficult step, may lengthen the operation time, and may be associated with some problems, including prolonged operation time, extended incision, or additional port insertion and injury of the spleen.6,13 Thus, many advocate that SFM may be omitted in most of the patients without worsening the surgical and oncological outcomes.5–7,16
Whether a routine or a selective SFM is considered, the major problem in the literature is the lack of a precise definition of SFM because the border of the mobilization has not clearly been determined in most analyses. The splenic flexure and the transverse colon are fixed to the spleen with the phrenicocolic ligament, which does not always exist but lies as an extension of Toldt's fascia, and with the splenocolic ligament. Dissection of these fascias may enable taking down the splenic flexure partially; however, further dissection through the gastrocolic attachments, which are actually the connection between the omentum and transverse colon, is required. In addition, the peritoneum located anterior to the pancreas goes by on the mesocolon and connects the pancreas and mesocolon. Complete SFM may only be achieved when the pancreaticomesocolic attachment is dissected through the inferior border of the pancreas, and sometimes ligation of inferior mesenteric vein at this level may also be required. We had decided to perform a partial SFM during the initial years of our laparoscopic colorectal surgery practice; however, in recent years we have preferred to dissect the gastrocolic and pancreaticomesocolic attachments (complete SFM) via an extra port in addition to the phrenicocolic and splenocolic ligaments that had been ligated during partial SFM. The current study aimed to analyze and compare the outcomes of these two procedures.
Because demographics and rates of neoadjuvant chemoradiation therapy application were similar, both groups may be considered to be homogeneous and comparable. In contrast to the previous studies, current data disproved an increase in operation time and intraoperative bleeding in patients receiving a complete SFM.6,17 In addition, the perioperative requirements for transfusion were also identical; however, the incidences for transfusion were significant in both groups. Although SFM was the only risk factor for splenic injury on multivariate analysis in a case-matched study, we have not observed this challenging complication in any of our patients. 18 The length of hospital stay was also identical between the groups. However, postoperative outcomes had the paramount significance, and previous studies have revealed that SFM does not decrease the rates of complications and re-operations and 30-day mortality.5,6 Correspondingly, these parameters were similar within the groups in our study, but occurrence of anastomotic leaks seemed to be higher in the completely mobilized group, which was the opposite of what had been expected. The increased frequency of leakage in the complete SFM group may be linked to the higher incidence of reservoir creation in this group, but our data did not clarify whether the anastomosis line or the reservoir staple line was the origin of the leaks. However, higher leak frequency may also be related to our extended effort to detect this complication in recent years, when complete SFM has been routine in our department, because most of these leaks were not clinically evident or worsened the early postoperative results and in particular did not increase the risk of a re-operation or 30-day mortality. In addition, complete SFM does not produce an extended volume of the specimen because there was no difference between the groups regarding the number of harvested lymph nodes, the length of specimen, and distal margin.
Although our data have shown that complete SFM and partial SFM are identical in almost all parameters studied, the conversion rate was less common and reservoir creation was more frequent in the complete SFM group. However, we do not know whether or not the conversion rate in the complete SFM group was directly related to the level of SFM because further analysis has shown that there were significantly more patients with T4 tumors necessitating conversion to open surgery in the partial SFM group (6 [16.7%] versus 2 [2.3%], P=.008). In addition, the experience gained may also have a role in the reduced rate of conversion because complete SFM has been more recently performed in our practice. Thus, although statistical analysis showed significance, in our opinion, the level of SFM may not have an effect on the conversion rate. Finally, our data have shown that reservoir creation is more common in the complete SFM group. Reservoirs after rectal cancer surgery may decrease defecation problems and consequently increase life quality and thus have been recommended in recent years. 19 We believe that the increased possibility of reservoir creation seems to be the only benefit of complete SFM, when compared with partial SFM.
As conclusion, in our opinion, the outcomes after partial and complete SFM may be similar because most of the parameters studied were identical regarding operation time, amount of bleeding, requirement and amount of transfusion, length of hospital stay, risks of complications, reoperation, and 30-day mortality, and pathological information including length of the specimen, number of harvested lymph nodes, and distal margin. Although complete SFM promises a decrease in conversion, it is unclear whether or not this finding is related to the technique of complete SFM, the higher rate of T4 tumors in the partial SFM group, or increased surgical experience. However, complete SFM may increase the possibility of reservoir creation. Therefore, we believe that the decision for the level of SFM is better left to the surgeon in cases undergoing a low anterior resection, but complete SFM may be preferred in patients who are candidates for a reservoir creation.
Footnotes
Disclosure Statement
No competing financial interests exist.