
Abstract
Abstract
Background:
Conventional laparoscopy is aided by CO2 insufflation, but this may impair cardiorespiratory function, induce stress responses, and result in life-threatening complications. CO2 insufflation is usually conducted under general anesthesia, whereas gasless laparoscopy supposedly eliminates most of these disadvantages. In this study, we compared the changes of concentration of serum cortisol, tumor necrosis factor alpha (TNF-alpha), interleukin (IL)-6, IL-10, and heat shock protein 70 (Hsp70) in patients undergoing gynecological laparoscopic surgery in order to explore the severity of the stress response following CO2 pneumoperitoneum or abdominal wall-lifting methods combined with the different anesthetic techniques performed.
Subjects and Methods:
Fifty-seven patients scheduled for gynecological laparoscopy from July 2009 to February 2010 with American Society of Anesthesiologists I–II evaluation and scheduled operation times of less than 100 minutes were randomly divided into three groups (GC, GG, or EG) with 20 patients in each group. Group GC patients were operated on with the aid of CO2 insufflation under general anesthesia. Group GG patients were operated on under general anesthesia using the gasless technique. Group EG patients underwent the same operative procedures under epidural anesthesia using the gasless technique. Serum cortisol, TNF-alpha, IL-6, IL-10, and Hsp70 were detected and analyzed at four time points: Before anesthesia (T1), 30 minutes after the beginning of the operation (T2), 10 minutes after the end of surgery (T3), and at 8:00 a.m. the following day (T4).
Results:
There were no obvious differences in the levels of serum cortisol, TNF-alpha, IL-6, IL-10, or Hsp70 among the groups at T1 (P>.05), but these values increased after the beginning of the operation and peaked in Group GC at T3 and in Group GG and Group EG at T4. The levels of serum cortisol and TNF-alpha were higher in Group GC than in Group GG at T2 (P<.05). At T3, levels of serum cortisol, TNF-alpha, IL-6, and Hsp70 were significantly higher in Group GC than in Group GG (P<.01) and were the same as the changes of IL-6 to IL-10 ratio (P<.05), while serum concentrations of cortisol, TNF-alpha, and IL-6 were also significantly higher in Group GG than in Group EG (P<.05).
Conclusions:
Gynecological laparoscopic surgery using abdominal wall-lifting methods could avoid the deleterious effects of CO2 pneumoperitoneum, and reduce the stress response. The lowest stress response was found when abdominal wall-lifting methods were used with the patient under epidural anesthesia.
Introduction
Patients and Methods
The study protocol was reviewed according to the Declaration of Helsinki and approved by the Human Ethics Committee of Nanjing Medical University. Written informed consent was received from all participants.
Between July 2009 and February 2010, 57 patients scheduled for gynecological laparoscopy, with American Society of Anesthesiologists I–II evaluation and a scheduled operation time of less than 100 minutes, were randomly divided into three groups (GC, GG, and EG) with 19 patients in each group. (Randomization was performed immediately before anesthesia by drawing prepared numbers from closed envelopes.) Exclusion criteria were as follows: Evidence or history of respiratory or cardiac disease or abnormal renal function. Group GC patients were operated on with the aid of CO2 insufflation under GA. Group GG patients were operated on under GA using a gasless technique. Group EG patients underwent the same surgical procedure under epidural anesthesia using a gasless technique. All patients were diagnosed with a single muscular tumor (approximately 5–8 cm in diameter), which included 28 cases of intramural myoma, 18 cases of subserous myoma, and 11 cases of muscular tumors in the broad ligament of the uterus.
All the patients had fasted for more than 8 hours before surgery and were premedicated with 0.1 mg of phenobarbital and 0.5 mg of atropine administered intramuscularly. Group GC and Group GG patients received GA with 0.05 mg/kg midazolam, 2 μg/kg fentanyl, 1.5 mg/kg propofol, and 0.12 mg/kg vecuronium and then underwent tracheal intubation with volume-cycled ventilation. GA was maintained by propofol and remifentanil (0.1 μg/kg/minute) combined with atracurium (6 μg/kg/minute), an extra bolus of 4 μg/kg fentanyl was given before surgery, and the target control infusion concentration of propofol was regulated to maintain the bispectral index at 50±3 during surgery. Ventilation was adjusted to achieve end-tidal CO2 of no more than 35 mm Hg and peak inspiratory pressure of no more than 30 mm Hg. Group EG patients received continuous epidural anesthesia. Epidural punctures were performed at the L2–L3 interspace, and the epidural space was identified by loss of resistance. After identification of the epidural space and a negative aspiration test for blood or cerebrospinal fluid, 1.5 mg/kg 0.75% ropivacaine and 0.05 mg of fentanyl were injected to achieve an upper sensory blockade level at T4–T6. Supplemental midazolam (1–2 mg) was given as needed. Ringer's solution was administered to all patients at a rate of 6–8 mL/kg/hour as maintenance.
In Group GC, the operation was executed using IAP of 12–13 mm Hg with room temperature CO2 insufflation. In Groups GG and EG, a mechanical retractor (Laparolift™ model KD-100, Nanjing Kangdaer Industry Co., Ltd.) was used to elevate the abdominal wall upwards by 8–12 cm with a force of 10–15 kg. 9 All operations were performed by the same experienced surgeon.
The heart rate (HR), systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), and pulse oxygen saturation were continuously monitored for all patients; patients under GA were monitored also by end-tidal CO2. All parameters were recorded before anesthesia (t1), at 15 minutes (t2) and at 30 minutes (t3) after the beginning of the operation, and at 10 minutes after the end of surgery (t4). In addition, after the induction of anesthesia, urine output was recorded using an indwelling catheter.
Blood samples were obtained from the cubital vein on the non-transfused side, collected into prechilled polypropylene tubes containing EDTA, and immediately centrifuged at 3000 g within 10 minutes, and the plasma was stored in polypropylene tubes at –70°C until used for analysis. Blood samples were used for determination of serum cortisol, tumor necrosis factor-alpha (TNF-alpha), interleukin (IL)-6, IL-10, and Hsp70 levels at four time points: Before anesthesia (T1), at 30 minutes after the beginning of the operation (T2), at 10 minutes after the end of surgery (T3), and at 8:00 a.m. on the following day (T4). Cortisol levels were determined by radioimmunoassay, and an enzyme-linked immunosorbent assay was used for TNF-alpha, IL-6, IL-10, and Hsp70.
Statistical analysis
Based on the previous studies,7,9 16 subjects per group were necessary to detect a difference of cortisol at 30 minutes after the beginning of the laparoscopic procedure with respect to obtaining a power of 90% (β=.10) with a two-sided design at α=.05 in this study.
Statistical analyses were performed using SAS version 9.1.3 for Windows. Data are expressed as mean±standard deviation values. The patient data (including age, weight, operation time, amount of Ringer's solution, blood loss, urine output, and the time to passage of gas via the anus) were analyzed using a one-way analysis of variance followed by Newman–Keuls multiple comparison test. Changes in hemodynamic parameters (MAP and HR) and the comparison of stress reaction parameters (cortisol, TNF-alpha, IL-6, IL-10, Hsp70, and the IL-6 to IL-10 ratio) were analyzed using repeated-measures analysis of variance with the least significant difference post hoc test. A P value of<.05 was considered statistically significant.
Results
The three patient groups were comparable in age, weight, height, physical condition, operative time, urine output, time from end of surgery to passage of gas via the anus, and use of intraoperative fluids (Table 1). The urine output in Group GG was more than in Group GC (P=0.0008) and less than in Group EG (P=.0007), and the time to passage of gas via the anus in Group EG was shorter than in Group GG (P=.0001).
Data are mean±standard deviation values. Group GC patients were operated on with the aid of CO2 insufflation under general anesthesia. Group GG patients were operated on under general anesthesia using a gasless technique. Group EG patients underwent the same surgical procedure under epidural anesthesia using a gasless technique.
P<.05 versus Group GC; bP<.05 versus Group EG.
MAP and HR both increased significantly during the first 15 minutes of insufflation in Group GC (P<.01) but remained at baseline levels in Group EG (P>.05). Compared with Group EG at t2 and t3, MAP values in Group GC and in Group GG were markedly higher (P<.05), and the highest level was observed in Group GC (P<.05) (Table 2).
Data are mean±standard deviation values. Parameters were recorded before anesthesia (t1), at 15 minutes (t2) and at 30 minutes (t3) after the beginning of the operation, and at 10 minutes after the end of surgery (t4).
P<.05 versus t1; bP<.05 versus Group GC; cP<.05 versus Group EG.
HR (bpm), heart rate (beats per minute); MAP, mean arterial pressure.
The pulse oxygen saturation was above 97% throughout the perioperative period in all groups. The interval (in minutes) of ventilation needed to be increased during the first 15 minutes of insufflation in Group GC to achieve normoventilation, whereas no changes were required in Group GG.
There were no obvious differences in serum cortisol, TNF-alpha, IL-6, IL-10, or Hsp70 among the groups at T1 (P>.05), and all these levels increased after the beginning of the operation, peaking in Group GC at T3 and in Group GG and Group EG at T4. The levels of serum cortisol and TNF-alpha were higher in Group GC than in Group GG at T2 (P<.05). At time T3, levels of serum cortisol, TNF-alpha, IL-6, and Hsp70 were significantly higher in Group GC than in Group GG (P<.01), as well as the changes in the IL-6 to IL-10 ratio (P<.05). Serum concentrations of cortisol, TNF-alpha, and IL-6 were also significantly higher in Group GG than in Group EG (P<.05) (Table 3).
Data are mean±standard deviation values. Blood samples were obtain before anesthesia (T1), at 30 minutes after the beginning of the operation (T2), at 10 minutes after the end of surgery (T3), and at 8:00 a.m. on the following day (T4).
P<.05 versus T1; bP<.05 versus Group GC; cP<.05 versus Group EG.
Hsp70, heat shock protein 70; IL, interleukin; TNF-alpha, tumor necrosis factor-alpha.
There were no perioperative anesthetic or surgical complications and no operative or postoperative complications in the following 3 days, and all patients were discharged without incidents.
Discussion
CO2 insufflation was the first technique used in laparoscopic surgery, but the effects on organisms were obvious.1–6,10–13 Among the reports mentioned, all of them focused on the comparison between pre- and post-insufflation. Our study compared two methods of anesthesia and two operative techniques lengthways and transverse for the same procedures and showed that CO2 insufflation could cause a strong stress response, with concentrations of cortisol, IL-6, IL-10, TNF-alpha, and Hsp70 all being increased and reaching a peak at the end of the operation and then rapidly declining after deflation, findings that were similar to previous reports.10,11 In contrast, AWL only gradually raised the concentrations of these factors, which reached their highest values at 8:00 a.m. the following day, tendencies that were in accordance with the findings of Larsen et al. 13
CO2 may cause both direct and indirect hemodynamic effects. CO2 directly dilates peripheral arterioles and depresses myocardial contractility, and CO2 indirectly activates the central nervous system and evokes sympathoadrenal activation, increasing myocardial contractility and causing tachycardia and hypertension. Exogenous CO2 increases peripheral vascular resistance and reduces the cardiac output during mechanical ventilation.5,6,11,13 During CO2 pneumoperitoneum, the indirect effects of CO2 seem to dominate. These were the agents causing the significant increases in MAP and HR observed in the CO2 insufflation procedure compared with AWL.
TNF-alpha is a sensitive cytokine involved in the early stress response; in general, its level rises rapidly after surgery and peaks at about 90–120 minutes. Inflammatory cascade reactions are activated once TNF-alpha is secreted, and the release of IL-6 and IL-8, among others, is promoted. Both IL-6 and IL-10 are important cytokines, playing contradictory roles in regulation of the inflammatory reaction. Serum IL-6 levels are early and sensitive markers of tissue damage because they rise in proportion to surgical trauma and associated injury. Additionally, elevations in IL-6 levels have been correlated with the subsequent clinical development of major complications.14,15 IL-10 is involved in immunomodulation and has an inhibitory action. IL-10 may thus inhibit IL-6 production at the transcriptional level of mRNA by inhibiting nuclear factor-kappaB activation and down-regulate the TNF-alpha secretion of mononuclear macrophages. 16
Heat shock proteins are highly conserved throughout evolution and have attracted great interest in both basic biology and in medicine. They are expressed at low levels under normal conditions, but their expression can be strongly induced by several stressors. Similar to cytokines, Hsp70 can mediate inflammatory reactions. Hsp70 binds with high affinity to the plasma membrane, elicits a rapid intracellular calcium flux, activates nuclear factor-kappaB, and up-regulates the expression of pro-inflammatory cytokines such as TNF-alpha and IL-6 in human monocytes. 17 The changes observed in Hsp70 levels were similar to those of IL-6 and IL-10 in this study. Njemini et al. 18 reported a positive correlation between the levels of Hsp70 and those of IL-6 and IL-10 and speculated that Hsp70 might be the originator of the inflammatory reaction. One potential mechanism of protection is the ability of Hsp70 to inhibit genetic expression of pro-inflammatory cytokines, the transcription of which is dependent on nuclear factor-kappa B activation. Yoshikai 19 also witnessed the inhibition of the excessive inflammatory reaction mediated by Th1 T-helper cells through Hsp 70 activation of CD4+ T cells and production of IL-10. However, IL-10 was also inhibited by the overexpression of Hsp70, but this did not block the increase in IL-6 synthesis; therefore, Hsp70 plays a role in mitigating the adverse effects of inflammatory reactions during infection or other pathological stresses. 20
Laparoscopy is “minimally invasive.” The main stimulus is CO2 pneumoperitoneum, which may produce a seriously unhealthy reaction resulting from increased IAP and hypercapnia and similar reperfusion injuries after deflation.1–3 All these stimuli could activate the reactions of the neuroendocrine and cardiovascular systems; meanwhile, other reactions mediated by the central nervous system include increased adrenocorticotrophic hormone-releasing hormone and adrenocorticotrophic hormone activation of cortisol secretion through the hypothalamic-pituitary-adrenal axis. As in previous research, 2 our study also showed that the degree of stress reaction positively correlated with the length and IAP resulting from CO2 pneumoperitoneum. A positive correlation among serum cortisol, vasopressin, norepinephrine, epinephrine, dopamine, and renin and MAP has been reported during CO2 pneumoperitoneum, 10 and this was also seen in our study. Compared with CO2 pneumoperitoneum, AWL avoided the effects of CO2 pneumoperitoneum and reduced the stress response during surgery, with the lowest stress response being observed in the AWL methods under epidural anesthesia; these were the reasons underlying the higher indices observed in Group GC than in Group GG at t2 and at t3.
A prospective, randomized clinical trial of 12 female patients undergoing laparoscopic resection of ovarian tumors showed that in the CO2 pneumoperitoneum group, arterial CO2 tension increased, dynamic pulmonary compliance decreased, peak inspiratory airway pressure increased, and plasma levels of epinephrine, norepinephrine, dopamine, and antidiuretic hormones all increased significantly during the laparoscopic procedure compared with the abdominal lift group. 9 Larsen et al. 13 carried out a randomized trial involving 50 consecutive patients scheduled for laparoscopic cholecystectomy and reported significantly higher levels of serum cortisol and insulin in the CO2 pneumoperitoneum group compared with the gasless procedure group.
In animal experiments carried out by Sahin et al., 2 21 rats were divided into three groups. Rats in the control group were subjected to GA only for 60 minutes. The stepwise group was subjected to CO2 insufflation at 5 mm Hg for 10 minutes, 10 mm Hg for 10 minutes, and 15 mm Hg for 60 minutes without deflation. In the Pp15 group, the pressure of CO2 insufflation was fixed at 15 mm Hg for 60 minutes without deflation. The result demonstrated that the highest plasma and liver malondialdehyde, TNF-alpha, and IL-6 values were observed in the Pp15 group, followed by the stepwise and control groups. However, plasma and liver superoxide dismutase levels measured in the control group were significantly higher compared with the stepwise and Pp15 groups. The lowest plasma and liver levels of superoxide dismutase were in the Pp15 group, followed by the stepwise and control groups. Significantly higher histopathologic scores were found in the Pp15 group, followed by the stepwise and control groups, as well as malondialdehyde and inflammatory cytokine (TNF-alpha, IL-6) levels. All these demonstrated that the stress response could be relieved to a certain extent through preliminary insufflation, while the gasless procedure could avoid it altogether. De Souza et al. 3 reported similar findings and also discovered that the frequency and severity of celiac adhesion correlated with the amount of CO2 insufflated and the IAP.
Levels of TNF-alpha and IL-6 were lower in Group EG than in Group GG at T3 in our study because AWL was still a surgical procedure and the stress response could not be inhibited by GA, while epidural anesthesia could efficiently inhibit conduction from the stimulus to the central nervous system, which not only blocked the impulse of the sympatho-adrenomedullary system, but also inhibited hypermetabolism and excitation of the hypothalamic-pituitary-adrenal axis. Meanwhile, the vagal tone increased following blockage of the adrenergic nerve, which might accelerate enterokinesia; this could explain why the time to passage of gas via the anus was shorter in Group EG.
The IL-6 to IL-10 ratio was related to the prognosis of patients with the systemic inflammatory reaction syndrome: A high ratio indicated poor prognosis; otherwise, eusemia. 21 In this study, the IL-6 to IL-10 ratio in Group GC was higher than that in Group GG at T3, which hinted that CO2 pneumoperitoneum might have an immunosuppressive effect. A lower CD4 to CD8 ratio in peritoneal tissue following CO2 pneumoperitoneum was seen in animal experiments by Gutt et al. 22 Takeuchi et al. 23 studied Donryu rats and found that laparotomy and CO2 pneumoperitoneum depressed splenic natural killer cell activity at 24 and 96 hours, and laparotomy also depressed hepatic natural killer cell activity at 24 hours, whereas in contrast, the gasless procedure did not show any reduction in splenic and hepatic natural killer activities (see the schematic flow of the relation of variables in the stress reaction in Figure 1).
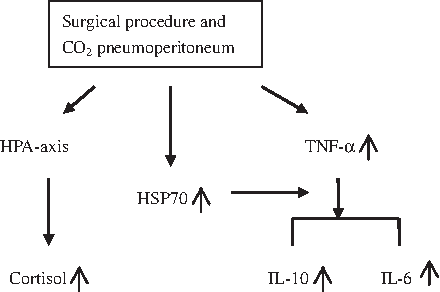
Stress stimuli induce activation of cortisol secretion through activation of the hypothalamic-pituitary-adrenal (HPA) axis and induce activation of tumor necrosis factor-alpha (TNF-α), which then results in inflammatory cascade reactions, releasing the inflammatory cytokines interleukin-6 (IL-6) and interleukin-10 (IL-10). Meanwhile, the stress response also induces activation of heat shock protein 70 (HSP70), which can regulate the secretion of IL-6 and IL-10 and keep the system in balance.
In this study, urine output was the lowest in Group GC, an effect that depended on the amount of IAP and the diminished renal blood flow caused by excitation of the sympathetic nervous system. Gutt et al. 12 documented the inverse correlation between IAP and both renal perfusion and urine output. At 15 mm Hg, cortical renal flow decreased by 28%, medullar renal flow decreased by 31%, glomerular filtration rate decreased to 18–31% of normal values, and urine output was below 0.5 mL/minute. Therefore, the easiest method for maintaining renal perfusion is the application of a sufficient intravascular volume loading before and during pneumoperitoneum. Low-dose dopamine 2 (μg/kg/minute) can prevent the renal dysfunction that is commonly associated with long-lasting surgical laparoscopic procedures with higher pneumoperitoneal pressures.12,24
In conclusion, gynecological laparoscopic surgery using AWL methods could avoid the deleterious effects of CO2 pneumoperitoneum and reduce the stress response during surgery. Among the groups the lowest stress response was seen when AWL methods were used with the patient under epidural anesthesia, and this procedure not only simplified anesthetic management but also maintained the stability of the respiratory and circulatory systems.
Footnotes
Disclosure Statement
No competing financial interests exist.