
Abstract
Abstract
Purpose:
Laparoscopic colorectal surgery creates fewer adhesions compared with open colorectal resection. Small bowel obstruction after laparoscopic colorectal resection may be caused by internal herniation of the small bowel through a colomesenteric defect, probably related to a lack of adhesion formation. This is seen especially after left colonic resections.
Methods:
A literature review was conducted using the key words “intestinal obstruction” and “laparoscopic left colonic resection,” and 9 documented case reports of obstruction following laparoscopic left colorectal resection were identified. We present 2 additional cases and discuss the etiology, diagnosis, management, and possible options for avoiding this complication.
Results:
In total, 167 consecutive laparoscopic procedures were performed in our study, and 8 were left hemicolectomies. Four of these patients (50%) developed intestinal obstruction, with 2 requiring surgical intervention for internal hernia. For the remaining 159 colorectal procedures, there were only 2 admissions with intestinal obstruction, with 1 patient requiring surgery (P=.006).
Conclusions:
Laparoscopic left hemicolectomy carries a significant risk of internal herniation. Performing a laparoscopic subtotal colectomy or fashioning the colocolonic anastomosis through the small bowel mesentery may minimize this risk.
Introduction
This article presents the problem of an internal hernia occurring following a “classic” laparoscopic left hemicolectomy, where the midtransverse colon is anastomosed to the mid- or proximal sigmoid colon for pathology around the splenic flexure. In this case, approximation and closure of the colonic mesenteric defect are technically difficult as the duodenal-jejunal (D-J) flexure will lie above and to the left of the neo-splenic flexure. Repositioning of the small bowel to the right side of the anastomosis requires mobilization of the entire small bowel mesentery, but again this is technically challenging. This is in comparison with other laparoscopic left-sided colorectal procedures where closure of the defect may be technically feasible.
We present 2 such cases and discuss the etiology, diagnosis, management, and possible ways to avoid this complication.
Case Reports
Case 1
A 70-year old woman underwent an uncomplicated laparoscopic left hemicolectomy for a descending colon tumor. She was admitted 2 months later with small bowel obstruction, which was confirmed on a computed tomography (CT) scan. At laparotomy, most of the small bowel had herniated behind the neo-descending colon. Small bowel resection was required, but closure of the mesenteric defect that caused the internal herniation was unsuccessful because of the position of the duodenal-jejunal (D-J) flexure in relation to the neo-splenic flexure.
Case 2
An 85-year-old woman underwent laparoscopic left hemicolectomy for a descending colon tumor. On postoperative Day 2, she developed abdominal pain and vomiting. A CT scan showed small bowel obstruction with most of the small bowel loops on the left side of the abdomen. Despite a trial of conservative management, she had a laparotomy on day 4. This revealed internal herniation of the small bowel loops behind the neo-descending colon. However, the small bowel was viable, and the colocolonic anastomosis was intact and therefore was left undisturbed. The small bowel was decompressed using a nasogastric tube. It was not possible to bring all the small bowel loops to the right of the descending colon or to close the mesenteric defect. The patient was discharged home on Day 7.
Literature Review
Laparoscopic surgery may create fewer adhesions and hence decrease adhesion-related admissions compared with open colorectal resections.1,2 However, the results from the MRC CLASSIC studies showed that this was not translated into a significant difference in surgical intervention for adhesive bowel obstruction between the two operative groups. 2 Other causes of small bowel obstruction after laparoscopic colorectal procedures are port site hernias and internal herniation. Internal herniation of the small bowel is seen more often after left-sided resections. 3 Although only 9 such cases have been reported in the literature, this complication may be underreported (Table 1).3–7
F, female; Lap, laparoscopic; LAR, laparoscopic anterior resection; M, male.
When an open left-sided colonic resection is performed, closure of the mesenteric defect may not be required as the large bowel quickly becomes adherent to the mobilized plane over Gerota's fascia. Recent case reports have highlighted a higher incidence of internal herniation after laparoscopic left colonic resections.3–7 The largest series of internal hernias after laparoscopic colonic resection has been described by Trabaldo et al., 3 who reported 5 patients with internal small bowel herniation out of 436 left colonic resections, representing an incidence of 1.14%.
Although we can attribute internal herniation after laparoscopic colorectal resections predominantly to decreased adhesion formation, there could be other contributing factors:
1. Splenic flexure mobilization may be less in laparoscopic surgery, so the resultant mesenteric defect may be narrow and tight when compared with open mobilization. 2. In a left hemicolectomy, the neo-splenic flexure may lie below and to the right of the D-J flexure. In this position, the proximal bowel lies to the left, and the terminal ileum lies to the right side of the colocolonic anastomosis; hence there is inevitable internal herniation of small bowel loops behind the colocolonic anastomosis (Fig. 1).
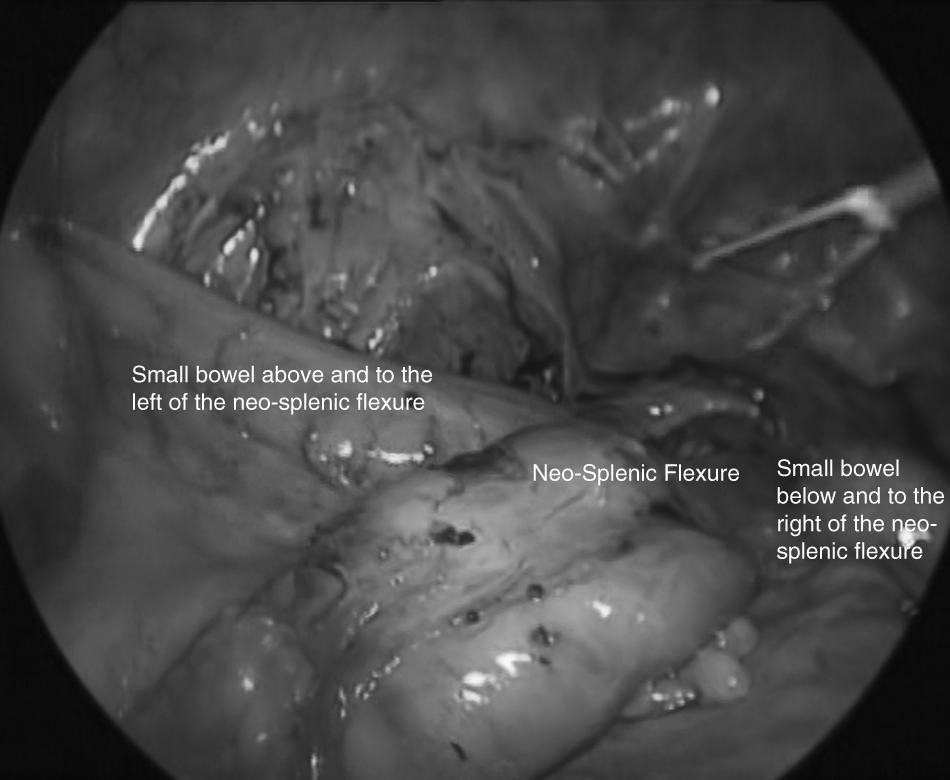
Inevitable internal herniation of small bowel loops behind the colocolonic anastomosis.
All but one case of small bowel internal herniation have been reported within the first 2 months of the primary resection (Table 1). A high index of suspicion is required, and an early CT scan is helpful. The CT scan usually shows the displacement of the mesenteric vessels, the presence of dilated small bowel loops in the left side, and collapsed bowel on the right side of the abdomen. 8 Although we performed a laparotomy to relieve the obstruction, this could be managed by laparoscopy. 5
The 9 cases reported in the literature revealed no predilection for age, sex, or pathology (Table 1). Two patients required small bowel resection, and in one case, performing a Hartman's procedure was the only way to relieve the obstruction. 3 There was one death due to mesenteric ischemia and septic shock.
In our series of 167 laparoscopic resections performed between 2002 and 2011, 8 patients had a laparoscopic left hemicolectomy. Four of these patients then developed small bowel obstruction, and 2 required surgical intervention. One patient required a small bowel resection, and the second patient had small bowel decompression only. In both patients, it was not possible to close the mesenteric defect responsible for the internal herniation. Of the remaining 159 laparoscopic patients, 2 were admitted with adhesive small bowel obstruction (P<.001), one of whom required surgery (P=.006). In comparison with other reported case series,3–7 we did not encounter internal herniation in patients undergoing laparoscopic sigmoid colectomy or anterior resection.
Various techniques have been described to avoid this complication (Table 2). Elio et al. 6 proposed lateral closure of the mesenteric defect using continuous sutures or clips. Despite closure of the defect with LigaSure™ (Covidien)/clips in 5 cases, Trabaldo et al. 3 reported 2 cases with internal herniation.
Blanc et al. 5 suggested complete repositioning of the small bowel to the right of the mesocolon at the end of the procedure after dividing the ligament of Treitz at the D-J flexure. This technique may make the small bowel less susceptible to herniation through the mesocolic defect. A practice of omentum interposition medial to the mobilized left colon may also be helpful. 5
All of these techniques can be helpful provided the neo-splenic flexure is above and to the left of the D-J flexure. If the neo-splenic flexure is below and to the right of the D-J flexure, like following a left hemicolectomy, there will be an inevitable internal herniation of small bowel behind the colocolonic anastomosis.
In this scenario, a subtotal colectomy with ileo-descending anastomosis may avoid this problem at the expense of an excessive bowel resection.
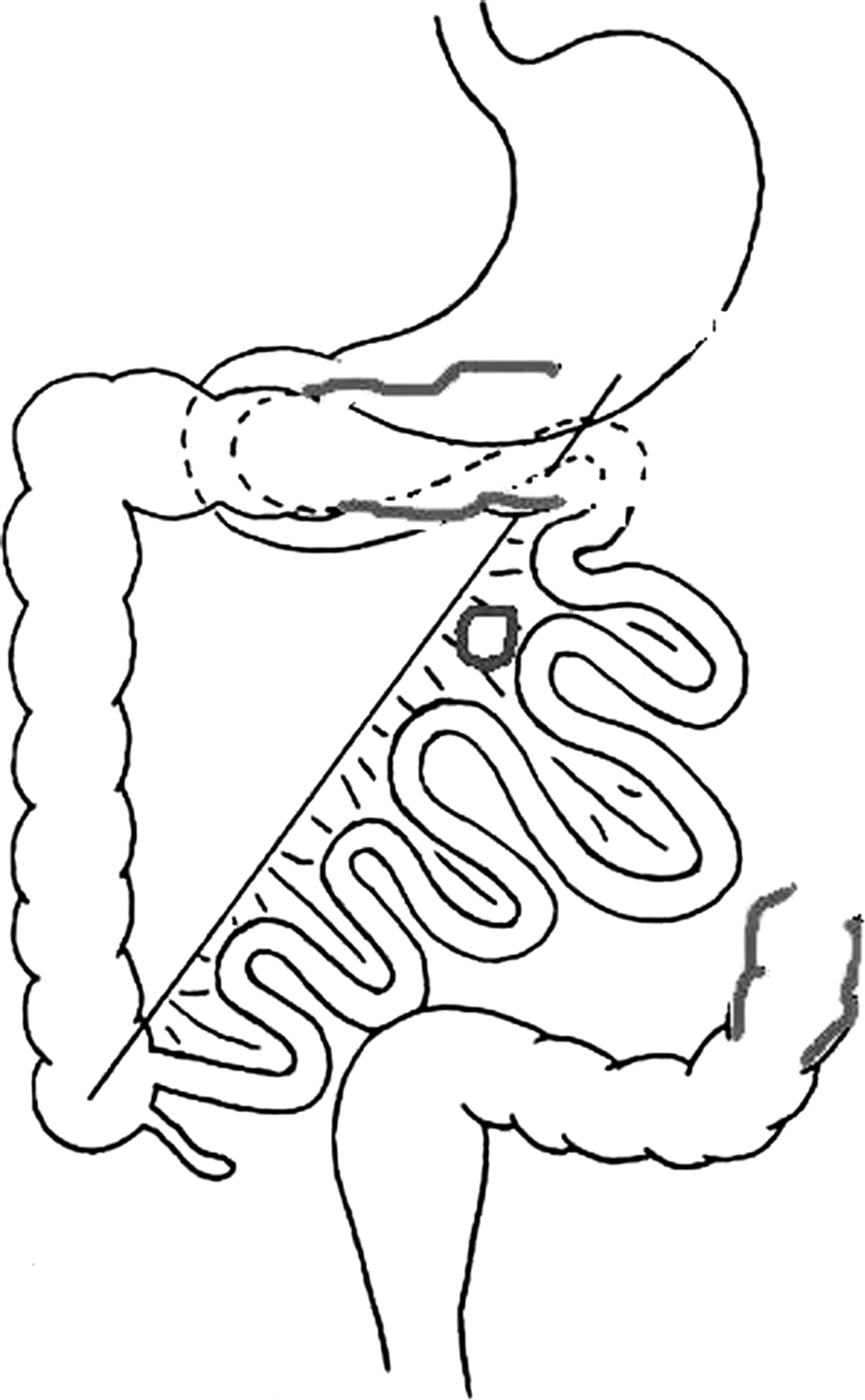
Alternatively, we recently modified a technique similar to the retro-colic gastrojejunostomy, where a window is created through the small bowel mesentery for passage of the transverse colon. 9 The transverse colon is anastomosed to the descending colon on the left side of the small bowel mesentery. This may be performed using an intracorporeal or extracorporeal technique. The edge of the window is sealed around the transverse colon using stitches (Figs. 2–4). 10 This technique may be performed during the primary surgery or as a salvage procedure for obstruction, in place of resorting to a Hartman's procedure. 3 We recently performed this technique in 3 patients, and we have had no incidence of internal hernia. The technique was completed extracorporeally in 2 cases (Fig. 5) and intracorporeally in 1 patient (Fig. 6).

The section of bowel, including the lesion to be removed, is shown in black, and the sections to be anastomosed together are shown in gray.
A transmesenteric defect is created.
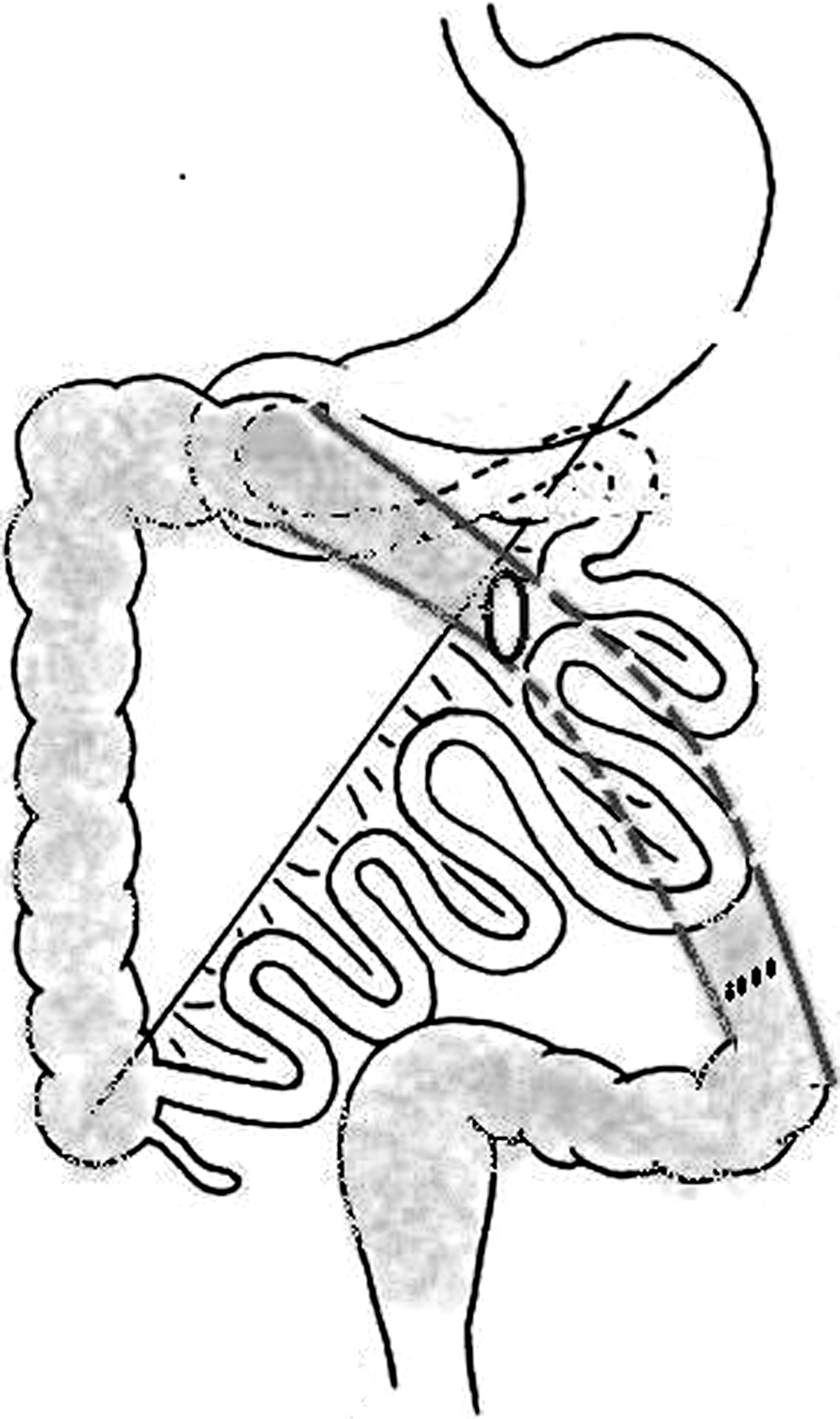
Completion of a transmesenteric colocolonic anastomosis.
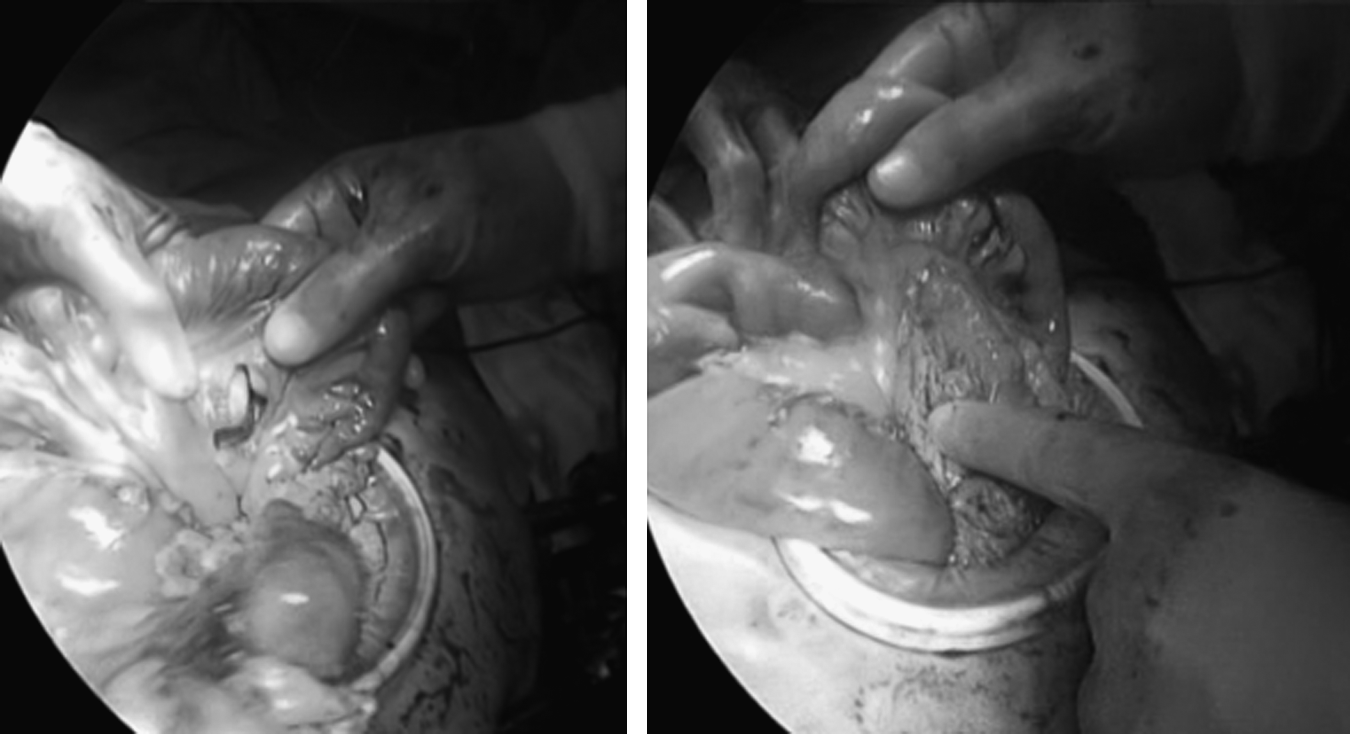
Extracorporeal transmesenteric anastosmosis.
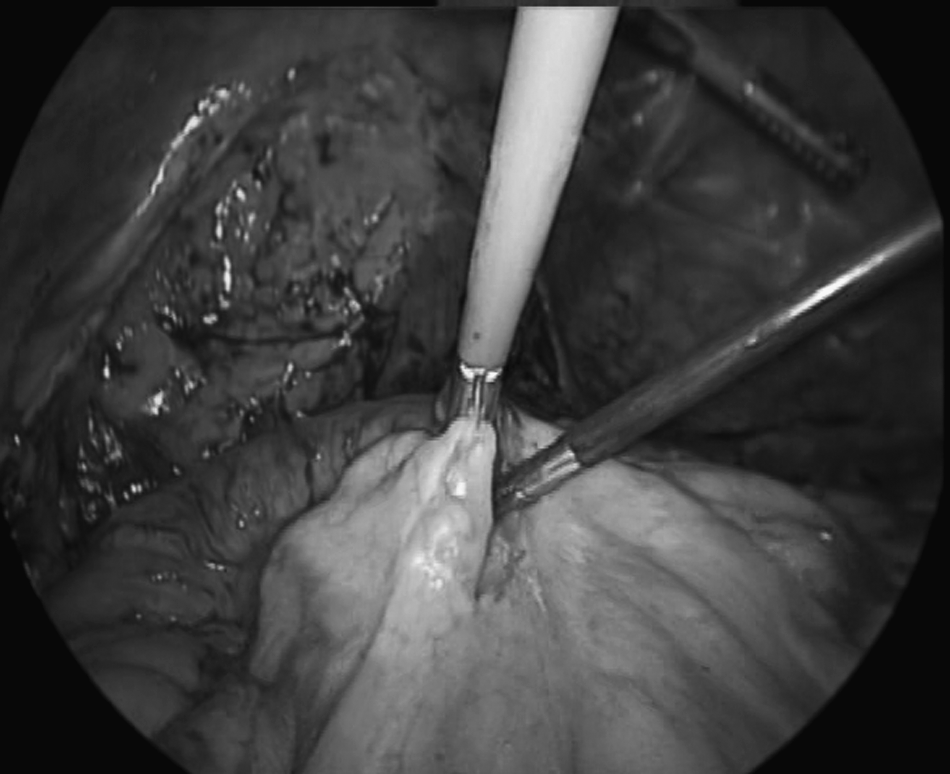
Intracorporeal creation of the mesenteric defect.
Conclusions
In the authors' opinion, when a left-sided colonic resection is performed, if the small bowel cannot be repositioned to the right side of the mesocolon and the colocolonic anastomosis, the risk of internal hernia is inevitable with an increased risk of intestinal obstruction. Classic laparoscopic left hemicolectomy, in particular, carries a higher risk of internal herniation. Laparoscopic subtotal colectomy or fashioning the colocolonic anastomosis through the small bowel mesentery may minimize this risk. Internal herniation of the small bowel should be suspected in all cases of small bowel obstruction following a laparoscopic left colonic resection, especially left hemicolectomy. Performing a CT scan and early surgery (laparoscopy or laparotomy) may avoid further morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.