
Abstract
Abstract
Background:
This article describes a novel, easy, and secure thoracoscopic intrathoracic esophagogastric anastomosis procedure that uses a circular stapler with transoral placement of the anvil for patients with esophageal cancer who underwent thoracoscopic esophagectomy.
Methods:
After the thoracoscopic esophagectomy, the esophagus was transected obliquely at the level of the upper posterior mediastinum using a linear stapler. The Orvil™ (Autosuture, Norwalk, CT) anvil was placed at the edge of the staple line of the esophageal stump, which was relatively at an acute angle to the stump. Next the gastric conduit was pulled through the esophageal hiatus into the right thoracic cavity. The shaft of a 25-mm circular stapler was inserted and placed into the gastric conduit from the gastrotomy. Circular stapling was undertaken in a conventional manner. The access opening on the stump of the gastric conduit was closed with a linear stapler intracorporeally.
Results:
The anastomotic procedure was completed in 20 patients. Intraoperative complications or conversions to open surgery from thoracoscopic surgery were not observed in any patient. There were no severe postoperative complications, such as anastomotic leaks or gastric conduit necrosis.
Conclusion:
The present study revealed that our novel thoracoscopic intrathoracic esophagogastric anastomosis was technically easy and safe with minimal morbidity.
Introduction
Reconstruction after esophagectomy must be technically safe and easy to undertake. In general, an intrathoracic esophagogastric anastomosis is thought to be superior to a cervical esophagogastric anastomosis in terms of a lower incidence of anastomotic leak and better cosmetic effect in patients who undergo open esophagectomy with two-field lymphadenectomy.4–6 However, in the reconstruction after thoracoscopic esophagectomy, esophagogastric anastomosis in the cervical portion has been preferred because intrathoracic esophagogastric anastomosis is technically difficult if using the thoracoscopic procedure.
We recently established a novel, easy-to-perform, and secure thoracoscopic intrathoracic esophagogastric anastomosis procedure that uses a circular stapler with transoral placement of the Orvil™ (Autosuture™, Norwalk, CT) anvil. This anastomosis procedure can be applied to the thoracoscopic Ivor Lewis esophagectomy. The present study demonstrates the surgical procedures and outcome of intrathoracic esophagogastric anastomosis in 20 patients with thoracoscopic esophagectomy.
Surgical Procedures
Patients
The intrathoracic esophagogastric anastomosis was applicable to patients with lower-third thoracic esophageal cancer who did not have apparent lymph node metastases in upper mediastinum or neck. These patients were suitable to undergo thoracoscopic Ivor Lewis esophagectomy without cervical lymphadenectomy because the incidence of metastasis to cervical lymph nodes is relatively low. Thoracoscopic intrathoracic esophagogastric anastomoses have been attempted for 20 patients (17 men and 3 women) after written informed consent was obtained between 2009 and 2010. The median age of the patients was 65 years (range, 52–77 years).
Hand-assisted laparoscopic procedures
Hand-assisted laparoscopic surgery was undertaken for mobilization of the lower esophagus and stomach with construction of a gastric conduit prior to thoracoscopic procedures. The patient was placed in the supine position with open legs, and three abdominal ports with a 7.5-cm transected incision were used. The greater-curvature side of the stomach was mobilized by dividing the short gastric vessels. The left gastric vein and artery were clipped and divided, followed by dissection of the lymph nodes around the root of the left gastric artery and celiac axis. After the posterior gastric artery was resected, the lower esophagus was mobilized circumferentially by a transhiatal approach. The anterior and posterior vagal nerves were not preserved in all cases. Finally, the abdominal esophagus was transected using the Endo GIA™ Universal system (Autosuture).
The stomach was pulled out through the incisional wound. A gastric conduit was constructed using the green stapler of the Endo GIA Universal system extracorporeally. The staple line of the gastric conduit was closed with 3-0 silk or Vicryl® sutures (Ethicon, Johnson and Johnson, Somerville, NJ). Pyloroplasty was carried out routinely using a finger-fracture method. The tip of the gastric conduit was temporarily attached to the tip of the lower esophagus and inserted into the lower mediastinum transhiatally.
Thoracoscopic procedures
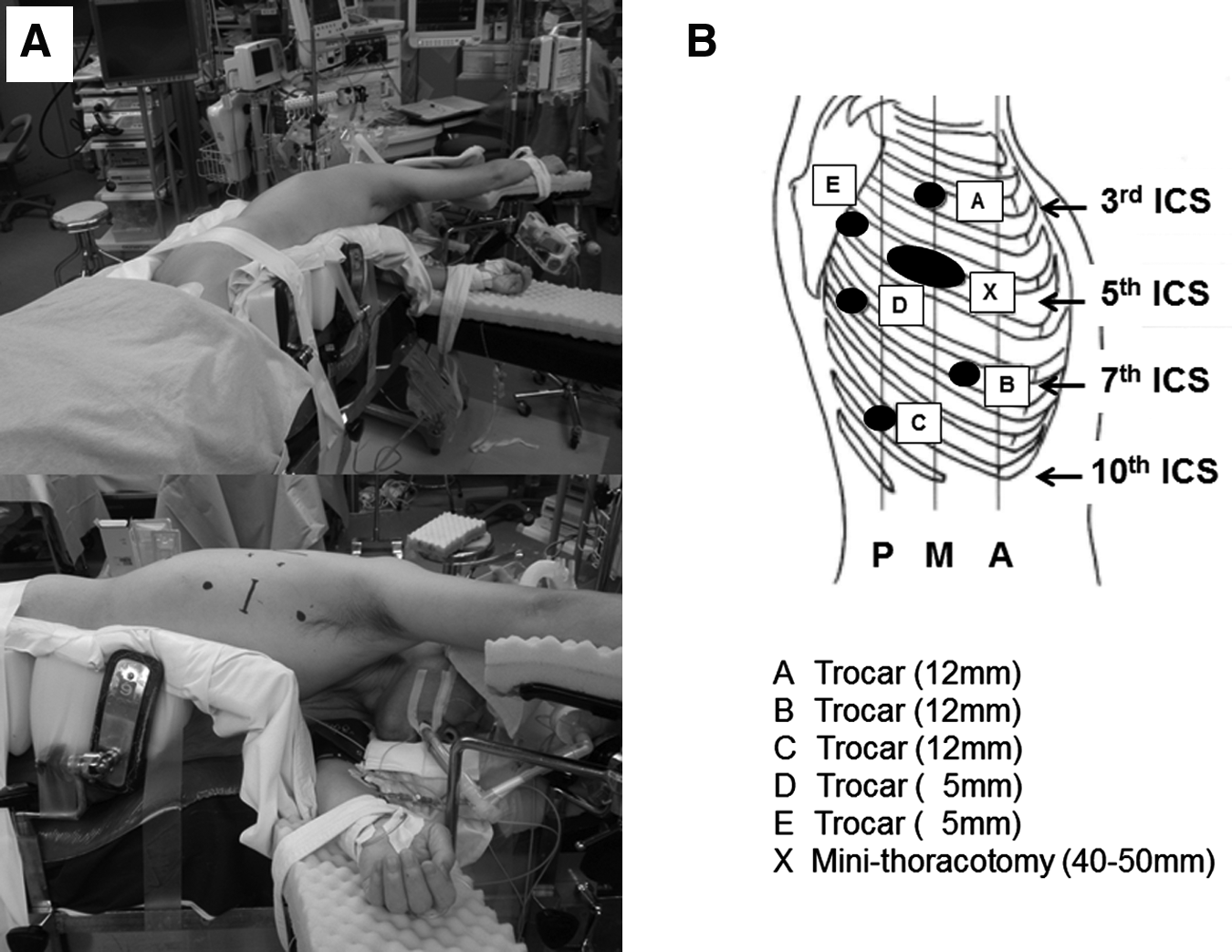
The patient was repositioned to the left semiprone position (Fig. 1A). It was possible to perform thoracoscopic esophagectomy with precise lymphadenectomy and easy and safe esophagogastric anastomosis in the optimal position (e.g., left lateral decubitus position, prone position) by rotating the operating table. First, the patient was positioned in the left lateral decubitus position. Five thoracic trocars and a small incision (4–5 cm) in the fifth intercostal space were introduced in the right chest (Fig. 1B). After the arch of the azygos vein was divided using the Endo GIA Universal system, the upper thoracic esophagus was mobilized circumferentially, and paraesophageal lymph nodes and nodes along the right and left recurrent laryngeal nerves were dissected. The thoracic duct was essentially resected. Subsequently, the patient's bed was rotated to be in the prone position to perform mobilization of the mid- to lower thoracic esophagus as well as dissection of the mid/lower paraesophageal, tracheobronchial, and subcarinal nodes. The left lateral decubitus position was preferred to undertake lymph node dissection for the upper posterior mediastinum (in particular for nodes along the left recurrent laryngeal nerve chain) because retraction of the trachea by the surgical assistant is a crucial part of the procedure (similar to open surgery). Conversely, the prone position was thought to be optimal for extended lymph node dissection of the mid- to lower posterior mediastinum because the right lung is lowered by gravity in the prone position. The mid-/lower posterior mediastinum in the prone position became wider with minimal retraction and was easier to dissect than in the left lateral decubitus position. Finally, the esophagus was transected obliquely at the level of the upper posterior mediastinum using the Endo GIA Universal system for the hemi-double stapling technique (DST) that we prefer to perform for the esophagogastric anastomosis (Fig. 2). The specimen was removed through the small thoracic incision.

The proximal esophagus was transected obliquely using a linear stapler.
Circular stapling techniques were used for esophagogastric anastomosis. The Orvil, an orogastric tube with an attached pretilted anvil head, was passed transorally by one of the surgical assistants in a standard manner. At that moment, in general, the left lateral decubitus position was preferentially chosen by rotating the operating table for easy transoral placement using the Orvil. A small esophagotomy was performed at the ventral edge of the staple line of the esophageal stump, which was relatively at an acute angle to the stump as a result of oblique transection of the esophagus (Fig. 3A). The orogastric tube was pulled through the esophagotomy by the surgeon and withdrawn through the thoracic incision until the anvil was positioned within the end of the esophageal stump (Fig. 3B). The suture attaching the anvil to the orogastric tube was cut, and the orogastric tube was separated from the anvil (Fig. 3C). Finally, placement of the anvil for connection to the 25-mm circular stapler was completed (Fig. 3D).
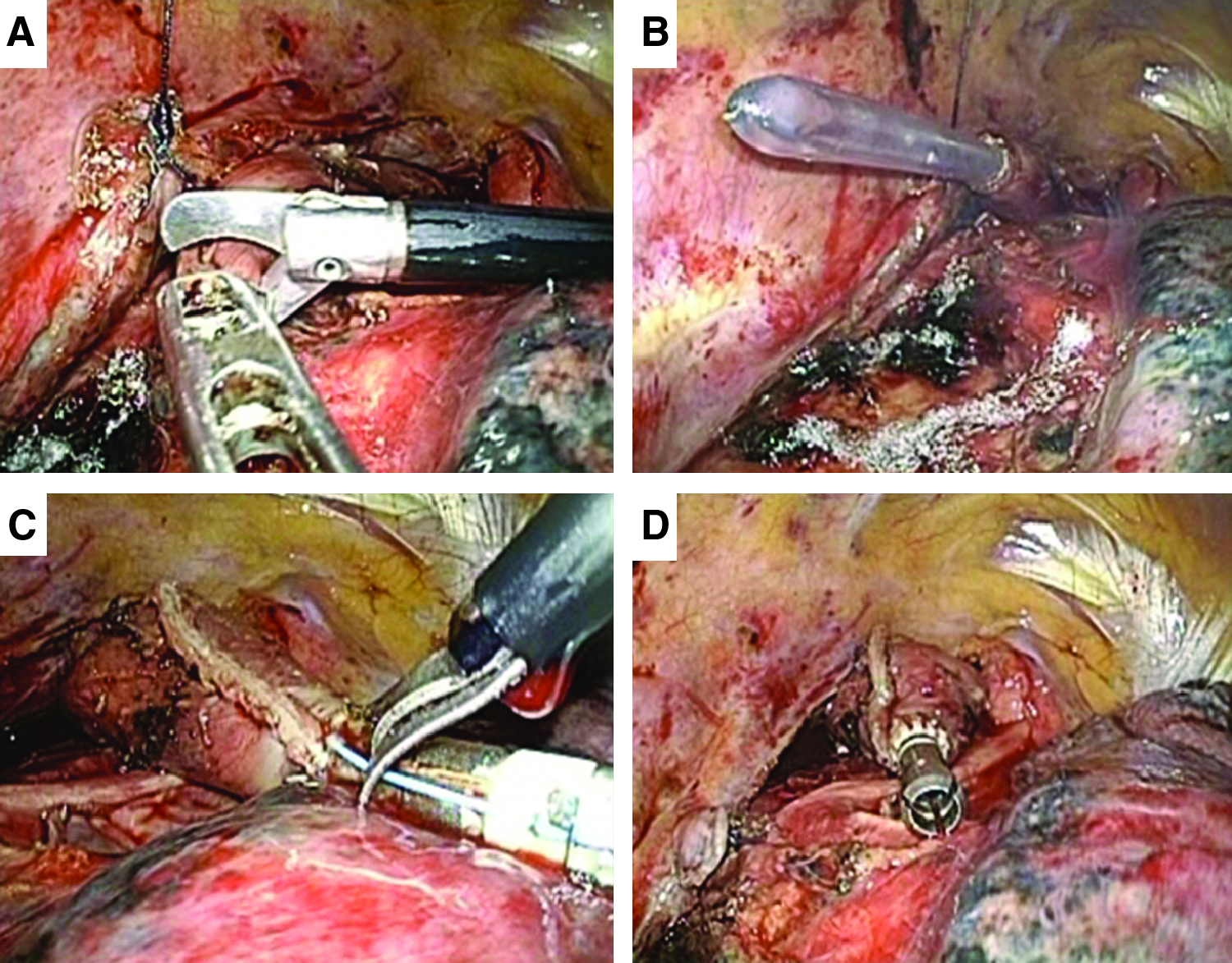
Thoracoscopic techniques for placement of the anvil.
The gastric conduit was pulled through the esophageal hiatus into the right thoracic cavity after placement of the Orvil. The stump of the gastric conduit was pulled through the small thoracic incision (4–5 cm). A small gastrotomy (3 cm long) was made on the stump of the gastric conduit. The shaft of a 25-mm circular stapler (EEA™ 25-3.5 XL Circular Stapler; Autosuture) was inserted and placed into the gastric conduit from the gastrotomy in preparation for reconstruction of the intrathoracic esophagogastric anastomosis (Fig. 4). The trocar of the circular stapler was extended to penetrate the anastomotic portion that was on the greater-curvature side of the gastric wall 5–10 cm apart from the stump of the gastric conduit (Fig. 5A). The trocar was thoracoscopically connected to the anvil placed in the esophagus. Circular stapling was carried out in a conventional manner, thereby completing the esophagogastric anastomosis (Fig. 5B, C). The access opening on the stump of the gastric conduit was closed at approximately 4 cm apart from the esophagogastric anastomotic portion with the Endo GIA Universal system intracorporeally (Fig. 5D). The staple line of the gastric conduit was closed with 3-0 silk sutures to prevent contact of the staples with the trachea, bronchus, and lungs. The greater omentum of the gastric conduit was wrapped around the esophagogastric anastomotic portion. The closed stump of the gastric conduit was sutured to the cranial side of the pleura of the thoracic wall for fixation of the gastric conduit (Fig. 6). An intraoperative gastroendoscopy was done to ensure the completion of esophagogastrostomy without anastomotic leaks. During circular stapling after placement of the Orvil, the prone position was chosen as the optimal position by rotating the operating table because the right lung frequently interferes with anastomotic procedures in the left lateral decubitus position. The prone position facilitates easier and secure anastomotic procedures because the right lung does not interfere with such procedures. Finally, a 32-Fr. chest tube was placed for postoperative chest drainage.

The shaft of a 25-mm circular stapler was inserted and placed into the gastric conduit from the gastrotomy.
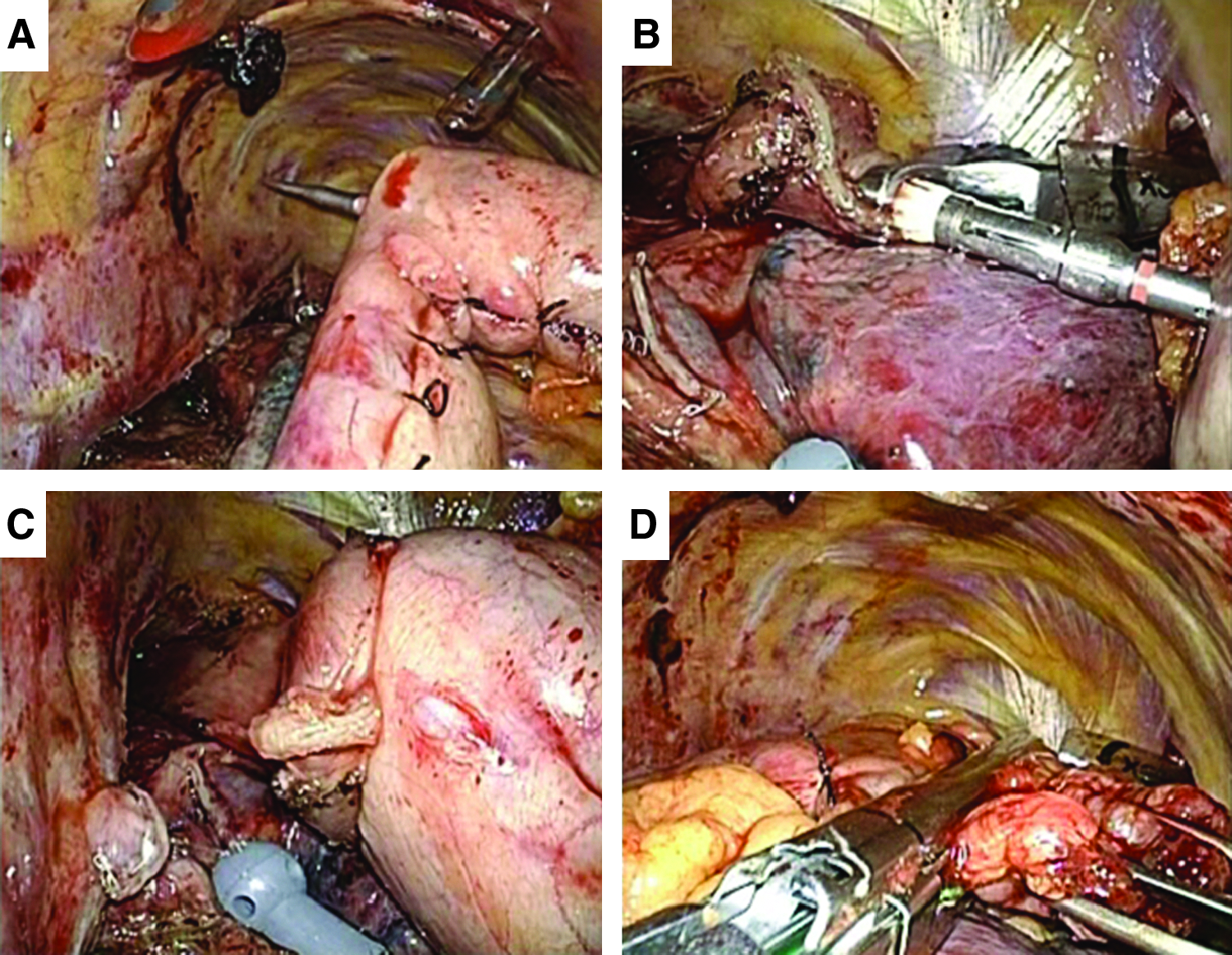
Reconstruction of the esophagogastric anastomosis.
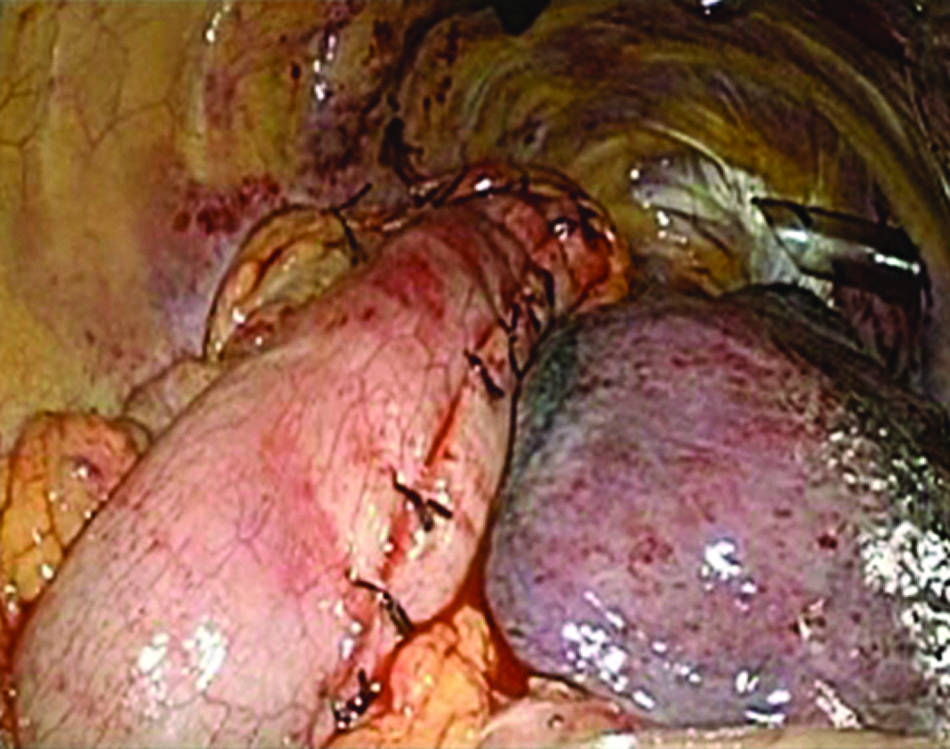
Completion of the thoracoscopic intrathoracic esophagogastric anastomosis.
Results
The thoracoscopic intrathoracic esophagogastric anastomosis was completed in all patients (n=20). Intraoperative complications or conversions to open surgery from thoracoscopic surgery were not observed in any patient. Severe postoperative complications, such as hemorrhage, anastomotic leak, gastric conduit necrosis, pyothorax, and incisional wound infection, were not observed in any patient. Postoperatively, 1 patient (5%) experienced temporary anastomotic stenosis, which was successfully treated by endoscopic balloon dilation several times in the outpatient clinic. Four patients (20%) complained of slight reflux symptoms after surgery, but these symptoms were well controlled with the use of proton-pump inhibitors.
Discussion
We developed a novel thoracoscopic intrathoracic esophagogastric anastomosis using a circular stapler with transoral placement of the anvil. The anastomotic procedure was completed in 20 patients. Intraoperative complications or conversions to open surgery from thoracoscopic surgery were not observed. Moreover, there were no severe postoperative complications such as anastomotic leak.
Most general surgeons, thoracic surgeons, and gastrointestinal surgeons are familiar with intrathoracic circular stapling for reconstruction after esophagectomy in open surgery. Intrathoracic circular stapling techniques are safe and easy to perform and facilitate esophagogastric anastomosis even in the upper posterior mediastinum. Therefore, we applied these circular stapling techniques to minimally invasive esophagectomy. However, placement of the anvil into the esophageal stump seems to be a major technical concern if the circular stapler is used in thoracoscopic surgery. Recently, the Orvil system was developed specifically for transoral delivery of the anvil head. The pretilted anvil head enables easy passage through the hypopharynx and upper esophageal sphincter during transoral delivery. The Orvil was originally developed for laparoscopic Roux-en-Y gastric bypass to simplify reconstruction of the gastrojejunostomy. 7 In our experience, although some mechanical maneuvers (extension of the patient's neck and deflation of the endotracheal tube balloon) were necessary to facilitate transoral delivery of the anvil head, it was successfully placed transorally using the Orvil system in all patients without problems or esophageal injury.
We prefer to perform esophagogastric anastomosis using the hemi-DST. Therefore, the esophagus was transected obliquely using a linear stapler at the level of the upper posterior mediastinum, and esophagogastric anastomosis was undertaken at the edge of the staple line of the esophageal stump (which was at a relatively acute angle to the stump). The left semiprone position enabled technically easy and safe esophagogastric anastomoses using the Orvil system by choosing the optimal position (e.g., left lateral decubitus and prone positions) by rotating the operating table. The left lateral decubitus position was preferentially chosen by rotating the operating table for easy transoral placement using the Orvil system. During circular stapling, the prone position was chosen for easier and secure anastomotic procedures because the right lung did not interfere with such procedures.
Recently Nguyen et al. 8 reported their experiences using the Orvil system for transoral placement of the anvil in preparation for a circular-stapled esophagogastrostomy during thoracoscopic Ivor Lewis esophagectomy. Their procedures were similar to our procedures. In their study, however, patients were positioned only in the left lateral decubitus position, and the esophagus was divided at the level of the azygos vein, which might be at a relatively lower level of the esophagus compared with our study. Moreover, the incidence of anastomotic leaks or gastric conduit leaks reached 9.8% in their study, which was relatively higher than that in the present study. We feel that several ingenuities in our procedures, such as the left semiprone position in which the prone and left lateral decubitus positions are available as well as the hemi-DST, may improve our results.
In conclusion, novel thoracoscopic intrathoracic esophagogastric anastomosis using the circular stapler with transoral placement of the anvil was technically easy and safe with a low prevalence of morbidity. Further study will be needed for validation, but this novel procedure is feasible and reliable as minimally invasive surgery for patients with thoracic esophageal cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.