
Abstract
Abstract
Background:
Although the advantages of laparoscopic colectomy have been demonstrated, there are few data available on laparoscopic resection of transverse colon cancer. The purpose of this study was to assess operative outcomes, long-term survival, and disease recurrence after laparoscopic resection of transverse colon cancer.
Subjects and Methods:
Prospective data were collected from 58 patients with transverse colon cancer among 1141 colorectal cancer cases undergoing laparoscopic resection between February 2001 and July 2009. Cancers located in both flexures were excluded.
Results:
The surgical procedures included 39 extended right hemicolectomies, 11 extended left hemicolectomies, 5 transverse colectomies, and 3 total abdominal colectomies. The mean operating time was 216 minutes, and the mean operative blood loss was 111 mL. The average harvested lymph nodes were 35.8. The proximal and distal resection margins were 20.27 cm and 15.23 cm, respectively. Eight patients developed minor complications postoperatively, but these cases were controlled conservatively without interventions. One patient was converted to an open procedure because of severe adhesions. There were no surgery-related deaths. The mean follow-up period was 40.5 months. There were no local recurrences during the follow-up period. Systemic recurrence developed in four patients: two in the liver and two with peritoneal seeding. The overall and disease-free survival rates at 5 years were 84.6% and 89.3%, respectively.
Conclusions:
Compared with previously published multicenter studies such as the COST, COLOR, and CLASICC trials, the long-term outcomes of this study demonstrate that transverse colon cancer can safely be resected using the laparoscopic technique in experienced hands.
Introduction
Subjects and Methods
Prospectively collected data on 58 patients with transverse colon cancer, out of a total of 1141 colorectal cancer patients who underwent laparoscopic resection between February 2001 and July 2009, were included in this study. The cancers located in the hepatic or splenic flexure were excluded. All operations were performed by a single surgeon (S.-H.K.). Chest x-rays, colonoscopy, barium enema, and computed tomography (CT) of the abdomen were included in preoperative evaluations. Routine laboratory tests, electrocardiography, and carcinoembryonic antigen (CEA) levels were also assessed preoperatively. To confirm precise tumor locations, colonoscopy was performed with India ink tattooing on occasion. The age, gender, co-morbidity, cancer stage, tumor location, operative method, amount of blood loss, operative time, conversion rate, number of harvested lymph nodes, and the length of both resection margins were analyzed. Postoperative complications, operative mortality, local recurrence, and systemic recurrence were also evaluated. Contraindications to laparoscopic resection were as follows: (1) direct invasion detected by CT scans to adjacent organs such as the duodenum and pancreas, (2) presence of a non-movable fixed tumor on physical examination, and (3) acute obstruction due to cancer.
Postoperative follow-up was as follows: for 2 years after surgery, physical examination and CEA levels were evaluated every 3 months, and then chest X-rays and abdominal CT scans were performed every 6 months. Over the next 3 years, physical examination, CEA levels, chest X-rays, and abdominal CT were carried out every half-year. Five years after surgery, the above examinations were performed annually. Colonoscopy was performed annually during the follow-up period. Postoperative adjuvant chemotherapy was carried out for Stage 2 cancer using oral 5-fluorouracil, and the FOLFOX or FOLFIRI regimen was used in patients with Stage 3 and 4 cancer. Overall 5-year survival and 5-year disease-free survival were evaluated.
SPSS version 12.0 software for Windows was used for statistical analysis. A Kaplan–Meier curve was constructed for the survival graph.
Surgical techniques
The patient was positioned in Dan Allen stirrups. A camera scope was inserted through a paraumbilical 10-mm port. Pneumoperitoneum was established with carbon dioxide at a pressure of 8 mm Hg. One or two No.1 silk sutures were placed in the periumbilical skin to anchor the camera port and lift up the abdominal wall as described previously. 11 According to the location of the tumor, a extended right hemicolectomy, transverse colectomy, or extended left hemicolectomy (anastomosis between the mid-transverse colon and the upper sigmoid) was performed.
For extended right hemicolectomy, the dissection was started around the ileocolic vessels. Lymph node dissection, vascular ligation, and colonic mobilization were performed intracorporeally using a medial-to-lateral technique. When middle colic vascular dissection was performed, the line of dissection was in the upward direction, to stay above the superior surface of the pancreas. Omentectomy was accomplished by dividing the omentum vertically at the proposed line of resection. The division of the greater omentum from the greater curvature of the stomach proceeded with care so as not to injure the gastric wall. The lesion-bearing segment was exteriorized, and a side-to-side (functional end-to-end) anastomosis was performed. Prior to the anastomosis, both mesenteric edges were checked so as not to be twisted. The mesenteric defect was not repaired.
For extended left hemicolectomy, because the left colic artery usually runs parallel to the inferior mesenteric vein, the inferior mesenteric vein is a good landmark for dissection in left colectomy. The dissection started from the right side of the inferior mesenteric vein with preservation of the inferior mesenteric artery. Dissection of the descending colon was carried out using the medial-to-lateral technique. The dissection was continued cephalad, and the pancreas was freed from the transverse colon mesentery. Once the lesser sac was entered, the dissection moved laterally. Complete lateral mobilization of the left colon up to the splenic flexure was performed. The sigmoid colon and its mesentery were usually mobilized to ensure a tension-free anastomosis. An extended wound was created at the paraumbilical or left upper quadrant port site, and anastomosis was performed using a linear endo-stapler.
For a transverse colectomy, the dissection was started around the origin of the middle colic vessels. The transverse colonic mesentery was carefully dissected off of the pancreas and duodenum below using a medial-to-lateral technique. Based on the surgeon's clinical judgment, either a splenic flexure or hepatic flexure mobilization was performed to prevent tension at the site of the anastomosis and to obtain enough of both resection margins. The lesion-bearing segment was delivered through the paraumbilical wound and divided extracorporeally. Prior to the anastomosis, the surgeon assessed the mesentery of the colon and made sure that they were not twisted. An anastomosis with a linear stapler or hand-sewn anastomosis was performed.
Results
Among the 58 patients, 31 were men and 27 were women, with a mean age of 62.7 years (range, 28–82 years). Co-morbidities included nine cases of hypertension, seven cases of diabetes mellitus, one case of pulmonary tuberculosis, and one case of liver cirrhosis.
The distribution of tumors according to TNM stage was as follows: Stage 0 in 6 patients, Stage I in 9, Stage II in 24, Stage III in 13, and Stage IV in 6. Stage 0 included cases of cancer confined to the mucosa of very large adenoma, and these cases were excluded from the survival analysis. Among the 58 patients, the tumor was located in the proximal transverse colon in 39 cases, in the distal transverse colon in 14 cases, and in the midtransverse colon in 5 cases (Table 1).
The types of operation performed included 39 extended right hemicolectomies, 11 extended left hemicolectomies, 5 transverse colectomies, and 3 total abdominal colectomies with an ileorectal anastomosis. The mean operating time and blood loss were 216 (range, 120–420) minutes and 111 (range, 30–800) mL, respectively. One case of left colectomy was converted to a conventional open surgical method because of severe adhesions. In two extended left hemicolectomies and one extended right hemicolectomy, the blood supply of the remnant colon was compromised with bowel color changes, resulting in a total colectomy with ileorectal anastomosis. The mean number of harvested lymph nodes was 35.8 (range, 5-80). The mean proximal and distal resection margins were 20.3 (range, 2.5–42) cm and 15.2 (range, 2–37) cm (Table 2). There were no injuries to the pancreas, duodenum, or spleen during the operations. Postoperative complications included 1 case of fungal peritonitis, 3 cases of chylous ascites, 1 case of anastomotic bleeding, and 3 cases of minor leakage of the anastomosis site, all of which were managed conservatively without any surgical intervention.
There was no postoperative mortality (Table 2). During a mean follow-up period of 40.5 (range, 1–88) months following curative resection, 2 patients developed distant metastases to the liver, and 2 developed peritoneal seeding. There was no local recurrence during the follow-up period. The systemic recurrence rate was 6.89%, and the local recurrence rate was 0% in this study. The overall survival rate at 5 years was 84.6% (Stage I, 100%; Stage II, 93%; Stage III, 83.9%) (Figs. 1 and 2), and the 5-year disease-free survival rate was 89.3% (Stage I, 100%; Stage II, 93.3%, and Stage III, 76.9%) (Table 3).
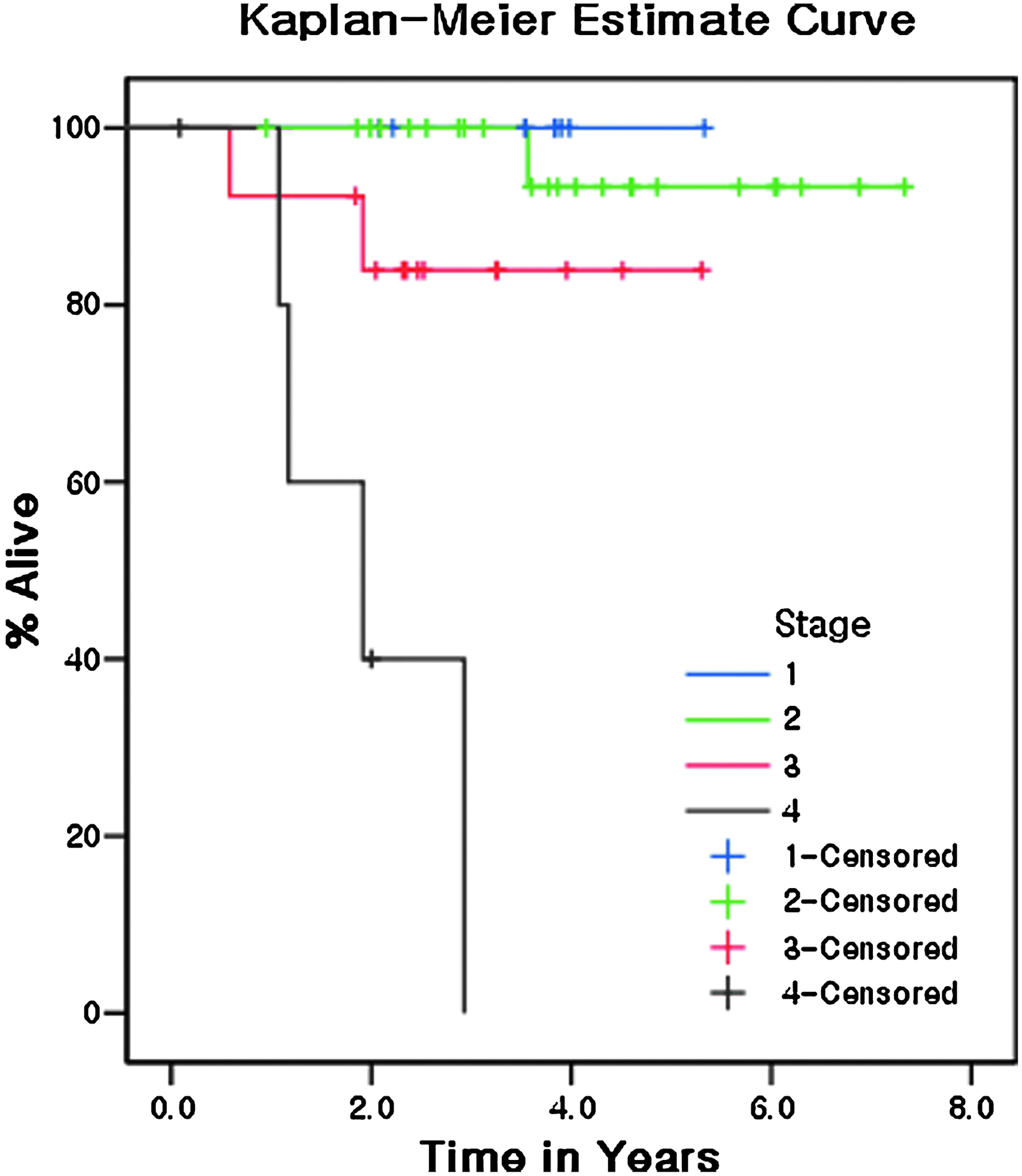
Five-year overall survival after laparoscopic transverse colon cancer resection in all stages (except Stage 0).

Five-year disease-free survival after laparoscopic transverse colon cancer resection for patients with Stages I, II, and III cancers.
Discussion
Several randomized studies demonstrated that laparoscopic colectomy provides early recovery with shorter hospital stays, improved cosmesis, minimized pain, reduced bleeding, and the least use of pain medications.5,12–14 In addition, a multicenter prospective randomized trial reported no difference in oncologic outcomes between laparoscopic and open colon cancer resection.3,4,6 Furthermore, laparoscopic surgery preserves immune function better than conventional open surgery.15,16 In spite of the many advantages of laparoscopic cancer surgery, carcinoma of the transverse colon often presents a surgical challenge due to the anatomical difficulties of dissection around the middle colic vessels with lymphatic drainage.9,10 However, there have been intense efforts to use the laparoscopic technique for transverse colon cancer resection. There have been two reports regarding laparoscopic transverse cancer resection supporting its feasibility since 2007.9,10 In this study, tumors located at the hepatic or splenic flexure were excluded because the definition of regional lymph nodes is different for the transverse colon (pericolic, middle colic) and both flexures (pericolic, middle colic, ileocolic, right or left colic). 7 This aspect might affect surgical outcomes from an oncological viewpoint.
Most laparoscopic studies have excluded carcinomas of the transverse colon, presumably for the following reasons: (a) difficulty of lymph node dissection along the middle colic vessels; (b) mobilization of the transverse colon involves dissection around the pancreas, which is vulnerable to injury; (c) difficulty in handling the omentum laparoscopically; (d) full mobilization of the splenic flexure together with an intact omentum is required for a left colectomy for distal lesions, which is a difficult laparoscopic procedure requiring expert skills; and (e) after removal of the tumor-bearing segment, the bowel ends should be checked to ensure that there is no tension at the site of anastomosis, which is sometimes difficult to determine by laparoscopy. The optimal surgical choice is controversial, because of the extent of resection of the lymph-bearing area and the blood supply to the anastomotic area with no tension.17,18
Our approach to tumor removal depended on tumor location in the transverse colon. For lesions located in the proximal transverse colon, an extended right hemicolectomy was performed. For distal lesions, an extended left hemicolectomy was the procedure of choice. For midtransverse colon lesions, especially in patients with long redundant transverse colons, transverse colectomy was considered as the appropriate approach. In all cases, partial omentectomy was carried out. Care was always required to prevent tension at the site of the anastomosis.
The proximal margin in 2 cases of left colectomy and the distal margin in 6 cases of right colectomy was less than 5 cm. However, given that a margin of 5 cm unstretched in situ has been noted to shrink to under 2 cm, 19 our cases in which the margin was measured in a fixed specimen might be acceptable. Four cases where proximal or distal resection margins were less than 5 cm were early-stage (Stage 0 or I), 2 were Stage IV with palliative resection, and 2 were Stage II cancer. The Stage II cancer patients had no local or systemic recurrence during 34 months and 72 months of follow-up, respectively.
With regard to oncological outcomes, the mean number of harvested lymph nodes in this study was 35.8. This result was quite superior to those of previous trials, such as the COST study (median number, 12), the COLOR trial (median number, 10), and the Transatlantic trial (mean number, 11.8±7.4) (a meta-analysis) 20 (Table 4). We achieved acceptable oncological outcomes by meticulous dissection around the middle colic vessels. Complete tumor resection with the large number of lymph nodes harvested facilitated accurate cancer staging and was conducive to optimal adjuvant treatment after laparoscopic transverse colon surgery. A limitation of this study was that we did not compare laparoscopic surgery with open resection for transverse colon cancer. A comparative study with open resection during the same period of time may be needed. In contrast to previous laparoscopic transverse colon cancer studies,9,10 however, our study had a long follow-up duration (mean, 40.5 months; median, 39.1 months). Also, the present study did not include the cancers in both flexures because of vascular supply and lymphatic drainage differences. These were different oncologic factors compared with the previous two studies.9,10 The 3-year overall survival rate of this study was 88.1% (Table 1). The 3-year overall survival rates of the COST, CLASICC, and COLOR trials21–23 were 86%, 68.4%, and 81.8%, respectively. The 5-year overall survival rate of the present study was 84.7% (Fig. 1). The 5-year overall survival rate was 76.4% for the COST study, 73.8% for the COLOR trial, and 55.7% for the CLASICC trial (Table 3). In terms of disease-free survival at 3 and 5 years, the 3-year disease-free survival rate in this study was 93.4%. Comparable rates in the COST, CLASICC, and COLOR trials were 81%, 66.3%, and 74.2%, respectively. The 5-year disease-free survival rate in this study was 89.3% (Fig. 2). The 5-year disease-free survival rate was 69.2% for the COST study, 66.5% for the COLOR trial, and 57.6% for the CLASICC trial (Table 3).
Collectively, we observed similar or superior outcomes compared with previous multicenter prospective randomized trials21,23,24 in overall and disease-free survival at 5 years. In particular, for Stage III cancer, our 5-year overall survival rate was 83.9%, and our 5-year disease-free survival rate was 76.9% (Fig. 2). The COST and COLOR trials reported 5-year disease-free survival below 60% and 5-year overall survival of approximately 60%–70% for Stage III cancer (Table 5). With regard to stage distribution, Stage II (41.3%) and Stage III (22.4%) cancers in this study were in the similar proportion to the laparoscopic group of Stage II (31%) and Stage III (26%) in the COST trial.6,21
Our recurrence rates were 0% for local recurrence, 0% for wound recurrence, and 6.9% for systemic recurrence. The COST study 21 reported a 2.3% local recurrence, 0.9% wound recurrence, 10.1% distant metastasis, and 19.4% overall recurrence rate in the laparoscopic surgery group. The COLOR trial 23 found that among 534 patients who underwent laparoscopic procedures, local recurrence developed in 4.9%, distant recurrence occurred in 10.4%, and wound recurrence in 1.3%, with an overall recurrence rate of 16.6%. In the CLASICC trial, there was 7.3% local recurrence, 11.3% distant recurrence, 2.5% wound recurrence, and 21.1% overall recurrence rate in the laparoscopic arm. 22 We believe the reason our oncologic data were superior to those in other studies is that we has performed the technique of “complete mesocolic excision” and “central vascular ligation” (Fig. 3). This technique, named first by Hohenberger et al., 25 is a type of aggressive surgery intended to remove the entire colonic mesentery and therefore all potential sites of nodal and intravascular tumor spread. They showed that in the first era after the implementation of this technique, the 5-year overall survival has increased by 15% (from 48.1% to 63.7%). In Korea and other Asian countries, it is the generally accepted surgical principle in colon cancer surgery, and the excellence of our result also might be caused by this principle.
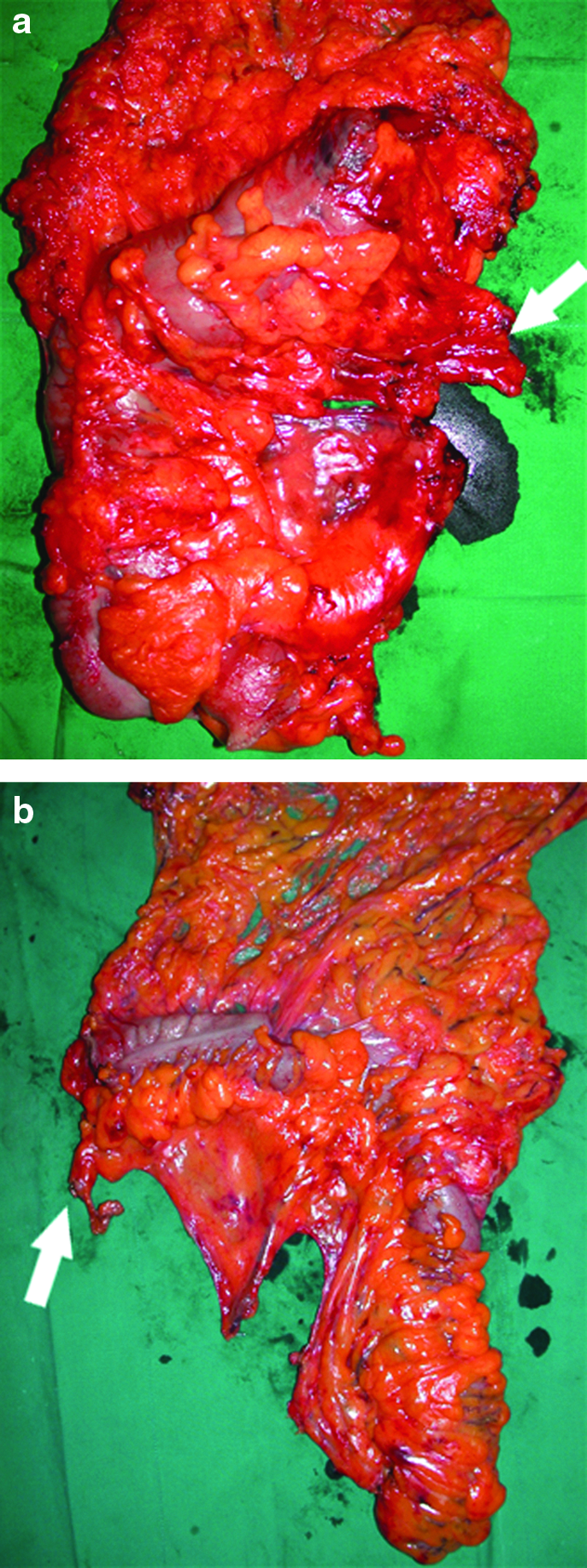
The technique of complete mesocolic excision and central vascular ligation:
In experienced hands, transverse colon cancer can be safely resected by laparoscopic surgery with acceptable long-term outcomes. Large-scale, multicenter, prospective, randomized trials comparing conventional open surgery with laparoscopic surgery for transverse colon cancer are now needed.
Footnotes
Disclosure Statement
We have no source of support in the form of equipment, drugs, or grants.