
Abstract
Abstract
Background:
The role of laparoscopic resection in patients with clinical T4 colorectal cancer remains controversial. This study compared the outcome of laparoscopic resection for clinical T4 colorectal cancer with that of an open approach.
Subjects and Methods:
Forty-three consecutive patients undergoing surgery for colorectal cancer with suspected involvement of another organ (T4) by computed tomography and/or magnetic resonance imaging were reviewed. Twenty-four patients who underwent laparoscopic colorectal resection were matched with 19 patients who underwent an open approach. All available clinicopathologic variables possibly associated with the outcome were compared.
Results:
Two patients (8.3%) who underwent the laparoscopic procedure were converted to the open technique. Patients in the open group displayed more advanced pathologic T category (P=.008) and underwent more combined operation than patients in the laparoscopic group (P=.017). The R0 resection rate was 75% in the laparoscopic group and 52.6% in the open group (P=.135). Patients in the laparoscopic group displayed a tendency for lower estimated blood loss (P=.083), sooner bowel movement (P=.075), and shorter length of hospital stay (P=.089) than patients in the open group. No significant differences in postoperative complications were observed between the laparoscopic and open groups (20.8% versus 36.8%, P=.246). After a median follow-up of 27 months, the 3-year disease-free survival rate in the laparoscopic group was found to be not significantly different from that in the open group (76.7% versus 58.8%; P=.303).
Conclusions:
Laparoscopic colorectal resection for T4 colorectal cancer is feasible and has perioperative and short-term oncologic outcomes similar to those of an open approach. However, further studies with long-term follow-up are needed to resolve these issues.
Introduction
To our knowledge, this is the first comparative study on the possible benefits of laparoscopic surgery and an open technique in patients who have preoperatively suspected T4 colorectal cancer. This study compared the outcome of laparoscopic resection in patients with clinical T4 colorectal cancer with that of an open approach.
Subjects and Methods
Between January 2005 and December 2009, 43 consecutive patients undergoing potential curative surgery for a suspected T4 colorectal cancer were reviewed from a prospective database. All of the operations were performed by two surgeons (J.W.H. and H.R.K.) already proficient in colorectal laparoscopic and open procedures. Twenty-four patients who underwent laparoscopic colorectal resection were matched with 19 patients who underwent an open approach over the same period. This study was reviewed and approved by the appropriate institutional review board.
The preoperative clinical staging tools used included a physical examination, colonoscopy or double-contrast barium enema, abdominopelvic computed tomography (CT), chest X-ray or CT, positron emission tomography scanning, complete blood cell count, liver function test, and serum carcinoembryonic antigen (CEA) level. In the case of rectal cancer, endorectal ultrasound, pelvic magnetic resonance imaging (MRI), or both were performed to assess the extent of local tumor invasion. T4 disease was suspected preoperatively in cases with a perforated tumor and/or invasion of adjacent organs on the above-mentioned preoperative imaging study.
All patients were given a preoperative mechanical bowel preparation. Conventional open surgery was performed in 19 patients as described elsewhere 2 ; the technique of laparoscopic resection has also been previously described.3–6 A medial-to-lateral approach with an extracorporeal stapled anastomosis was performed for right-sided resections, whereas a medial-to-lateral dissection with intracorporeal double-stapled anastomosis or hand-sewn coloanal anastomosis was used in left-sided colon resections or rectal resections. The completeness of resection was determined for each patient based on the operative and pathology reports and was classified as follows: R0 (negative gross and pathologic margins), R1 (negative gross margins with positive microscopic margins), and R2 (positive gross margins).
Disease staging was determined based on final pathological features according to the 7th International Union against Cancer TNM staging system. Postoperative adjuvant treatment was dependent on the patient's general condition or compliance and the preference of the physician. The patients were followed at 3-month intervals for 2 years, at 6-month intervals for the next 3 years, and annually thereafter. For patients who did not return for observation after 1 year, information was obtained via a letter or telephone call. On a semiannual basis or when suspicion of recurrence arose, the follow-up examination included a clinical history, physical examination, serum CEA level, chest X-ray or CT, abdominopelvic CT or MRI, colonoscopy, and positron emission tomography scanning if available. The determination of recurrence was made by clinical and radiological examinations or by histological confirmation.
Statistical evaluations were performed using SPSS (version 14.0 for Windows; SPSS Inc., Chicago, IL). Differences between the two groups were analyzed using the chi-squared test, Fisher's exact test, or the Mann-Whitney U-test, as appropriate. Survival rates were calculated using the Kaplan–Meier method, while survival curves were compared using the log-rank test. A P value of ≤.05 was considered statistically significant.
Results
The demographic and perioperative data for all 43 patients are summarized in Table 1. The laparoscopic and open groups were well matched in terms of age, gender, body mass index, American Society of Anesthesiologists score, history of abdominal surgery, clinical staging, and preoperative chemoradiation in rectal cancer. However, significant differences were found in terms of location of tumor and preoperative CEA level between the two groups.
Values in parentheses are percentages unless indicated otherwise.
Values are expressed as the median (range).
ASA, American Society of Anesthesiologists; CEA, carcinoembryonic antigen.
Details of the operating procedures and perioperative data are given in Tables 2 and 3, respectively. Small bowel segmental resection was the most frequent procedure of combined surgery in both groups (Table 2). There was no postoperative mortality within 30 days of operation and no intraoperative complications in either group. Two patients who underwent the laparoscopic procedure were converted to the open technique because of duodenal invasion in right-sided colon cancer (n=1) and tumor infiltration into the pelvic sidewall in cases with rectal cancer (n=1). The patients in the open group displayed a higher percentage of undergoing combined resections (P=.017), large tumor (P=.003), and pathologic T4 disease (P=.008) than those in the laparoscopic group. However, no significant differences were found in terms of diverting stoma, completeness of surgery, differentiation, pN category, or pM category (Table 3).
Values in parentheses are percentages unless indicated otherwise.
Values are expressed as the median (range).
Lower estimated blood loss, quicker bowel movement, and shorter length of hospital stay were observed in the laparoscopic group compared with the open group, but the differences did not reach statistical significance (Table 4). Overall postoperative complications and clinical anastomotic leakage were similar between the groups. Two of the 3 patients with leakages were managed conservatively, whereas 1 patient required Hartmann's procedure after open anterior resection.
Values are expressed as the median (range) unless indicated otherwise.
Values in parentheses are percentages.
During the median follow-up time of this series, which was 27 months (range, 4–72 months), the 3-year overall survival and disease-free survival rates were 74.7% and 68.4%, respectively (Fig. 1). The 3-year disease-free survival rate in the laparoscopic group was not significantly different from the rate in the open group (76.7% versus 58.8%; P=.303; Fig. 2).
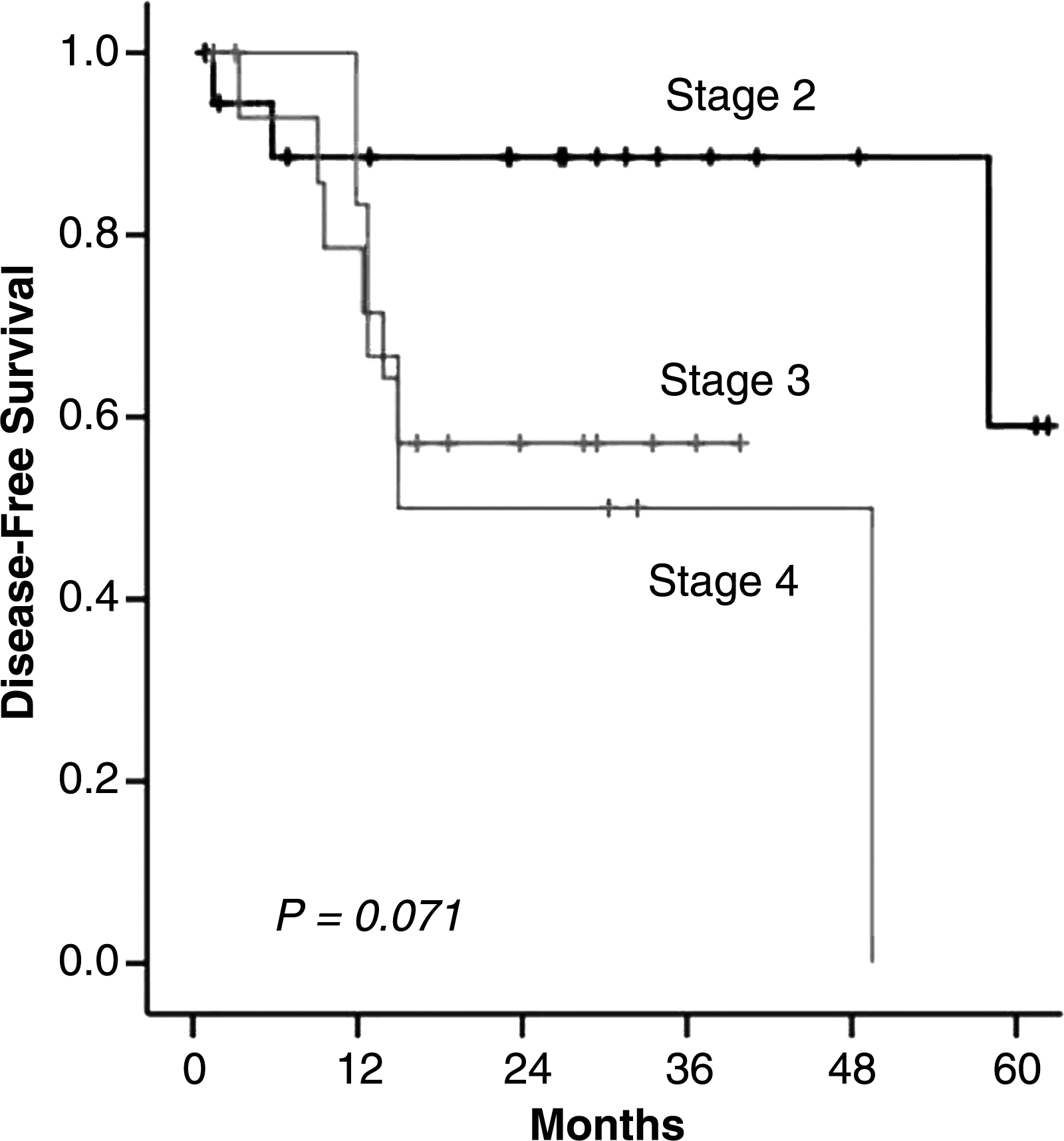
Disease-free survival according to pathologic TNM stage.
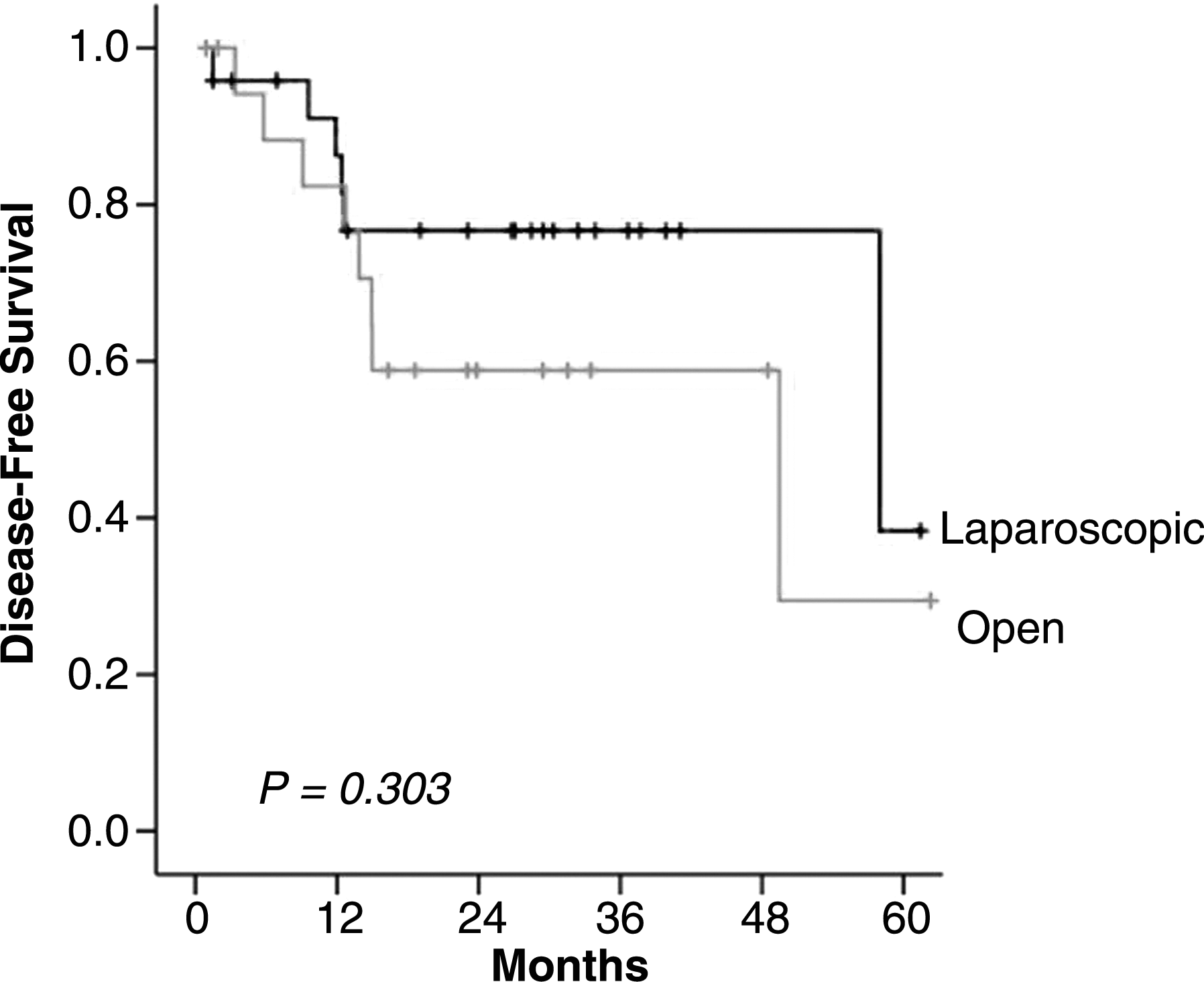
Disease-free survival according to operative method.
Discussion
The major findings in this study are that laparoscopic resection for colorectal cancer can be achieved with low rates of conversion and morbidity even in patients with preoperatively suspected T4 tumor and that this is associated with acceptable perioperative outcomes and disease-free survival rates when compared with open resection.
The potential benefits of laparoscopic colorectal surgery compared with open surgery include faster recovery, lower morbidity, less pain, and a shorter hospital stay, and these can be achieved without compromising oncologic outcomes.7–11 In the present study, we aimed to determine whether or not these advantages could be applied to patients with T4 cancers. We found that the conversion rate to open surgery after laparoscopy was 8.3%, and the laparoscopy-related postoperative complication and leakage rates were 20.8% and 4.2%, respectively, which compare favorably with the results of open surgery despite a lack of statistical significance.
It is well recognized that T4 tumors increase the risk of conversion to open surgery after laparoscopic surgery. The current conversion rates for colorectal cancer range from 7% to 50%,8,12,13 whereas the rate steeply climbs if T4 lesions are included. Actually, in several randomized trials for laparoscopic colorectal surgery, all patients with a preoperatively suspected and/or intraoperatively detected T4 tumor were systematically converted.8,14 The present study found that conversion was required in only 2 (8.3%) patients with a suspected T4 tumor in selected cases, and the reason for this was invasion of the tumor to adjacent organs. One patient with lower rectal cancer who received preoperative chemoradiotherapy was converted to open abdominoperineal resection after laparoscopic surgery, and he experienced perineal wound disruption during hospitalization and developed presacral recurrence at 12 months postoperatively. In rectal cancer, preoperative chemoradiotherapy has the potential to increase curative resection despite being a laparoscopic approach. In our study, despite the anticipated technical difficulties, the procedure was completed laparoscopically in four of five middle to lower rectal cancers that received preoperative therapy. The other patient with right-sided colon cancer directly invading the duodenum was converted to open right hemicolectomy and duodenal segmental resection. In right-sided colon cancer, duodenal and/or pancreas invasion cases are the most demanding and difficult for laparoscopic resection, and therefore such invasiveness constitutes a real obstacle. Bretagnol et al. 1 and Pokala et al. 15 have suggested similar guidelines for duodenal invasion of tumor or fistulous disease, another condition that is difficult to manage laparoscopically. In the present study, only 6 of 15 right colon tumor patients with preoperatively suspected T4 disease were chosen and underwent laparoscopic surgery. Taken together, demanding conditions such as fistulization, duodenal or pancreatic invasion, complex pelvic irregularities, bladder invasion, or multiple previous surgeries may be best taken directly to open surgery, or laparoscopic inspection may be attempted with a high suspicion that they would be converted to open surgery cases.
Undoubtedly, if there is any uncertainty in preoperative imaging or intraoperatively, then surgeons should not hesitate to convert laparoscopy to open surgery. The current imaging accuracy for detecting tumor invasion is documented to be between 47.5% and 80%. 16 The current 7th International Union against Cancer TNM staging system has subdivided T4 lesions into pT4a (tumor penetrates the surface of the visceral peritoneum) and pT4b (tumor directly invades or is adherent to other organs or structures). In our study, pathologic invasion of T4 confirmed at operation was noted in 51.1% of the 43 patients; moreover, the incidence of pT4 was significantly higher in the open group than in the laparoscopic group. The current limited accuracy of preoperative imaging modality has been one of the obstacles for choosing an adequate operative method.
We have presented a relatively small comparative study of patients with clinical T4 colorectal cancer. To our knowledge, this is the first report on the efficacy of laparoscopic T4 colorectal resection compared with an open approach. Despite the limitations of this study resulting from small sample size and non-randomization, we conclude that laparoscopic T4 resection by experienced surgeons is technically feasible in selected cases and has perioperative and short-term oncologic outcomes similar to those of an open approach. Further randomized studies with long-term follow-up are needed to resolve these issues.
Footnotes
Acknowledgments
This study was supported by a grant (CRI11070-1) from the Chonnam National University Hospital Research Institute of Clinical Medicine.
Disclosure Statement
No competing financial interests exist.