
Abstract
Abstract
Objective:
This study assessed the safety of direct trocar insertion (DTI) versus Veress needle followed by primary trocar insertion (VN).
Methods
Results:
Seven randomized studies consisting of 2940 women (VN, n=1525; DTI, n=1415) were identified. The data on the safety of two entry techniques were abstracted, integrated, and analyzed with the meta-analysis method and are presented as pooled relative risk (RR) with 95% confidence intervals (CI). There were 4 cases of a major complication in the VN group in contrast to none in the DTI group. Pooled results failed to show a statistically significant difference in the risk of major complications between the two groups. A significantly higher risk of minor complications was detected in the VN group (RR [95% CI]=10.78 [6.27–18.51]). Among minor complications, preperitoneal injuries (46.73 [11.55–189.10]) and omental injuries (4.51 [2.12–9.62]) were the two most common complications in the VN group. There were significantly increased risks of multiple insertions (more than two attempts) (2.99 [2.11–4.23]) and failed entry (2.21[1.07–4.56]) in the VN group.
Conclusion:
This meta-analysis suggests that the commonly used VN entry technique carries a significantly increased risk of minor complications. In addition, the likelihood of multiple insertions and failed entry are significantly higher in the VN group.
Introduction
The open laparoscopic access (Hasson) technique was designed to prevent vascular and visceral injury by direct visualization and division of abdominal wall layers. The Hasson method, however, is less frequently used as an alternative to closed techniques (VN, DTI) and is mainly used in high-risk patient populations such as patients with multiple abdominal surgeries, severe endometriosis, a history of pelvic inflammatory disease, or a prior tubo-ovarian abscess. Compared with other access methods, the Hasson technique is relatively time consuming and tends to cause a greater difficulty in maintaining a pneumoperitoneum due to gas leakage. In addition, the scientific data do not support the prevention of intraabdominal injury, especially bowel injury, by using this method.13–15 The direct optical access was designed to decrease the risk of intraabdominal injury by allowing the surgeon to visualize abdominal wall layers during trocar insertion. Similar to the Hasson entry, randomized studies comparing direct optical access with other entry techniques are limited.15,16
The DTI technique was first reported by Dingfelder 17 in 1978. The rationale for DTI, without prior pneumoperitoneum, is based on the difficulty of grasping and lifting the abdomen after it is distended with gas 12 and the fact that the VN accounts for many complications.7,8 Several meta-analyses and systematic reviews related to the DTI versus the VN have been published,9,11,18,19 but the study designs have limited the confidence in the data. Some of the limitations include the fact that laparoscopic entry is surgeon-dependent, possibly leading to selection bias and underreporting in retrospective and nonrandomized studies. Furthermore, many confounding variables, such as obesity, prior abdominal surgery or infections, and other comorbidities are difficult to adequately control for in nonrandomized studies. For these reasons, meta-analyses limited to randomized studies are needed.
We were only able to locate two meta-analyses of randomized studies comparing DTI with VN. In 2003 Merlin et al. 18 reported that major complications in the DTI group versus the VN group were inconclusive. Minor complications, however, were fewer with the DTI (relative risk [RR]=0.19, 95% confidence interval [CI] 0.09–0.40), predominantly because of a reduction in extraperitoneal insufflation. Three randomized studies were included in the meta-analysis with the pooled sample size of 665. Similarly, in 2008 Ahmad et al. 19 reported that DTI had the advantage of reduced extraperitoneal insufflation and failed intraperitoneal entry with an odds ratio (OR) of 0.06 (95% CI 0.02–0.23). Six randomized studies were included in this analysis; however, the entry technique described in one study 20 was a modified open access, instead of DTI. Another study 21 did not report detailed safety data but only efficiency (e.g., insertion time). The other four studies generated the pooled sample size of 1640.
The objective of this study, therefore, was to perform an updated, larger-scale meta-analysis of randomized clinical trials comparing the safety of the two closed laparoscopic entry techniques (VN versus DTI) and determine which of these methods is safer. The principal hypothesis was that the VN is equivalent to the DTI access in regard to safety.
Methods
Sources
Ovid MEDLINE®, Cochrane Library, Google Scholar, and Scopus were searched up to September 2011 using the terms “direct trocar,” “veress needle,” and “verres needle.” The literature search was restricted to human studies published in English. A parallel search using MeSH terms on PubMed was conducted and did not reveal any additional articles. In addition, we manually searched the reference lists of relevant review articles and meta-analyses but did not identify additional studies. Because of an inadequate quantity of data and because the existing data failed to show a benefit, the Hasson and direct optical access techniques were not included in this analysis and literature search. The definition for multiple trocar insertions was more than two attempted entries.
Study selection
The methodology conformed to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (formerly QUORUM) criteria. 22 The articles were extracted and assessed independently by two authors to identify the studies that met the following inclusion criteria: Randomized clinical trials conducted on humans, written in English, including both comparison groups of interest (DTI versus VN), and measuring one or both of the primary meta-analytic outcomes (major and minor complication rates of laparoscopic entry). Varying definitions of DTI entry techniques were used; hence, each article was carefully reviewed to ensure that the DTI techniques were performed as previously described. 17 Disagreements by authors over inclusion and exclusion of studies and interpretation of data were resolved by the senior author.
The methodological quality of the studies was assessed with the following criteria: Randomization scheme, adequacy of allocation concealment, and statistical power. Several other potential sources of qualitative heterogeneity among the studies were identified and recorded. These included characteristics of the study sample (e.g., inclusion of only nonobese patients or patients with no history of prior abdominal surgery), type of surgery (general or gynecologic), and geographical location of the study. Because quality-score weighting methods can be problematic and produce biased-effect estimates,23,24 a quality score was not used in this analysis for evaluation. Differences between the studies in the above-mentioned criteria, therefore, are described in tabular form, and none of the trials was excluded on the basis of quality assessment.
This meta-analysis was performed using SAS version 9.2 software. The primary outcomes assessed were major and minor complications (intraoperative and postoperative) of two laparoscopic entry techniques (DTI versus VN). Heterogeneity of estimated effects across studies was assessed by the Cochran's Q statistics to determine the suitability of studies to be pooled for the meta-analysis. The between-study heterogeneity was considered significant for a P value <0.10. 25 None of the selected studies reported effect size by either RR or OR. RR for individual studies along with pooled RRs and 95% CIs were calculated and reported by forest plot. Because of the small number of studies included in this meta-analysis, it is very difficult to determine publication bias by visual inspection of funnel plot, and hence a normal quantile plot was used for assessment of potential publication bias. Data falling on a straight line and within the 95% CI bands in a normal quantile plot would suggest no evidence of publication bias. 26
Results
Our literature review identified 117 articles that were reviewed independently by two authors for potential inclusion (Fig. 1). We excluded 101 articles after reviewing the abstract and title, leaving 16 articles for more detailed assessment. After reading the entire manuscript, nine studies were eliminated because they were either not randomized or the DTI technique was actually a modified open technique. Seven studies, therefore, were included in the meta-analysis with a total of 2940 subjects for analysis. The quality characteristics of the seven studies are summarized in Table 1.
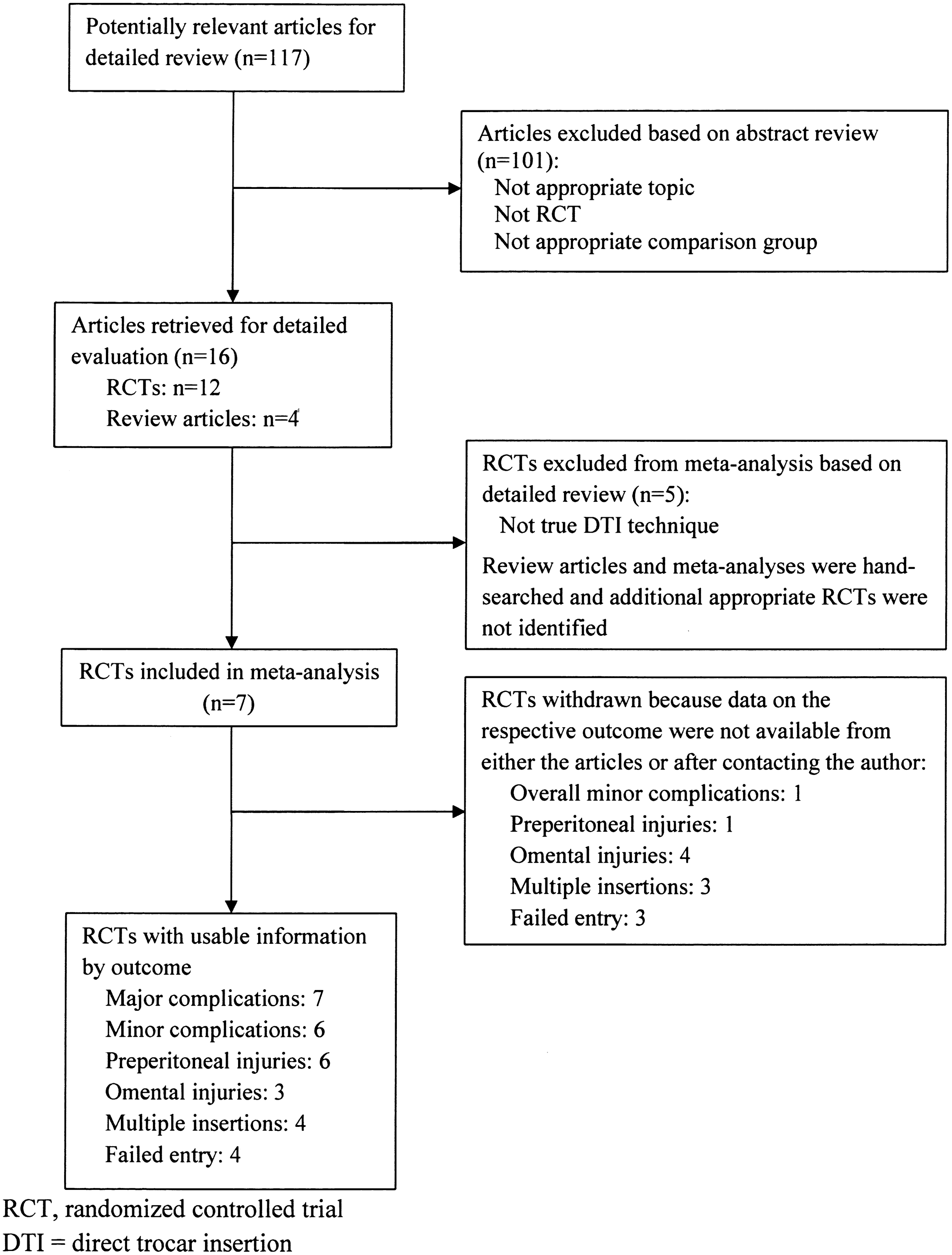
The flow diagram depicts the literature search and selection strategy for the meta-analysis. DTI, direct trocar insertion; RCT, randomized controlled trial.
Four studies (Tansatit et al., 21 Nezhat et al., 28 Agresta et al., 30 and Gunenc et al. 31 ) were excluded for the calculation of total n (%) in the prior Abd surgery column, P=.43.
Abd, abdominal; BMI, body mass index; DTI, direct trocar insertion; SD, standard deviation; SNOSE, sequentially numbered opaque sealed envelopes (which were opened in the operating room immediately before the surgery); VN, Veress needle followed by a blind primary trocar insertion.
The statistical testing for heterogeneity was not significant (Q=2.06, P>0.10); therefore, a fixed-effect model (Mantel–Haenszel) was used for RR calculations. There was no evidence of publication bias suggested by the normal quantile plot. All seven studies reported major complications as a primary outcome, with a pooled RR of 8.35 (95% CI 0.45–154.97), suggesting there was a nonsignificantly increased risk of major complications in the VN group.
Figure 2 demonstrates the pooled analysis for the six studies (n=2840) reporting minor complications as one of the primary outcome variables. The overall risk of a minor complication was significantly higher in the VN group with a pooled RR of 10.78 (95% CI 6.27–18.51). Common minor complications reported included subcutaneous emphysema, preperitoneal insufflation, omental injury, and omental emphysema. All minor complications were regrouped into two main subcategories: Preperitoneal injuries (preperitoneum insufflations and subcutaneous emphysema) or omental injuries (omental injuries and omental emphysema). Among those minor complications, only preperitoneal injury was recorded and reported in all of six studies. The six studies (n=2840) were pooled and analyzed for the risk of preperitoneal injury, as shown in Figure 3. This analysis revealed a significantly increased risk of preperitoneal injury in the VN group with a pooled RR of 46.7 (95% CI 11.5–189.1). The risk of omental injury was also significantly higher in the VN group with an RR of 4.51 (95% CI 2.12–9.62) based on the pooled analysis for three studies (n=1412) (Fig. 4).

This forest plot depicts the relative risk (RR) of overall minor complications of the Veress needle entry technique. LCL, lower confidence limit; UCL, upper confidence limit. The studies included were Borgatta et al., 27 Nezhat et al., 28 Byron et al., 29 Agresta et al., 30 Gunenc et al., 31 and Zakherah. 32
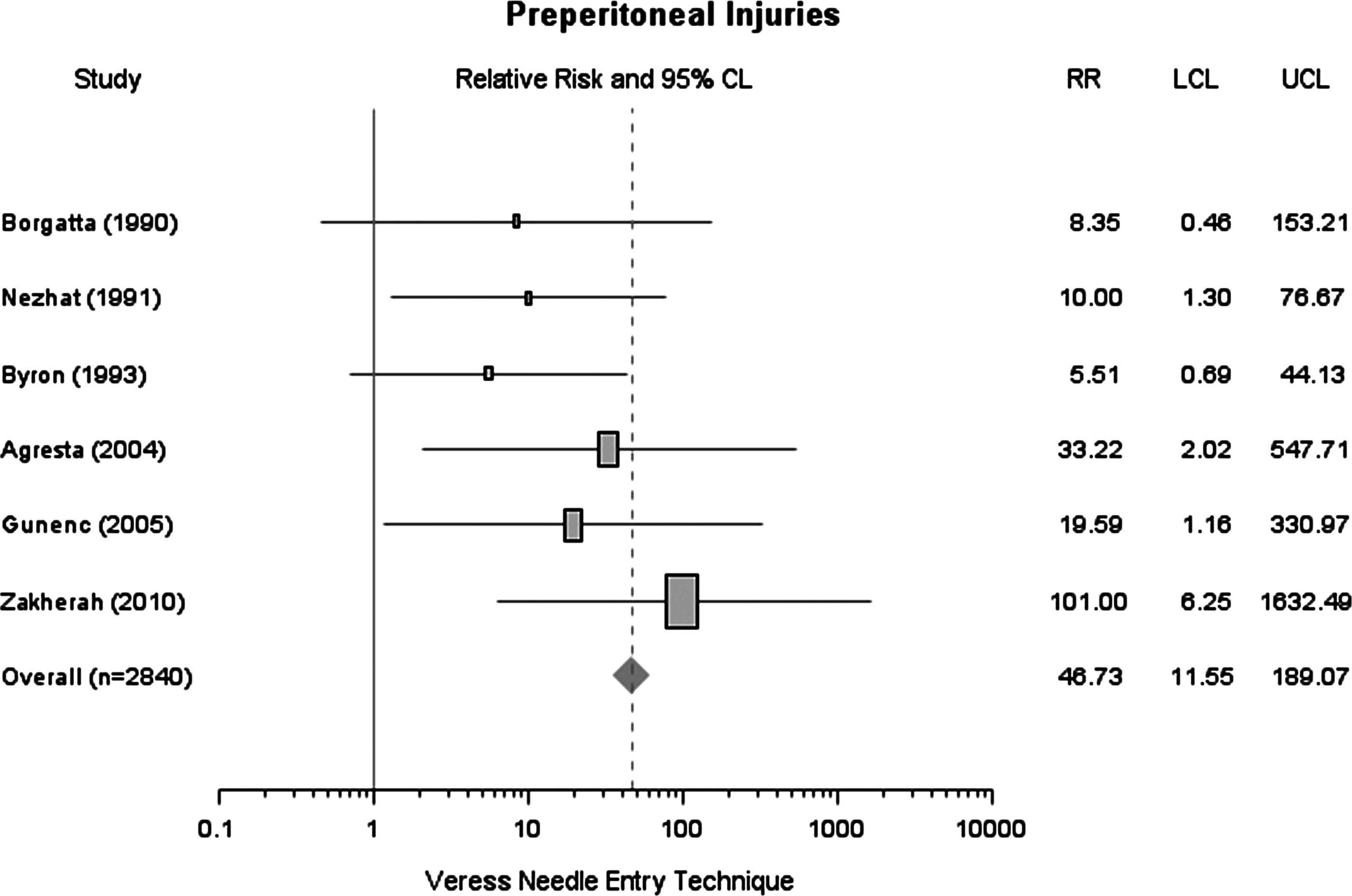
This forest plot depicts the RR of preperitoneal injuries (preperitoneal insufflation and/or subcutaneous emphysema) of the Veress needle entry technique.

This forest plot depicts the RR of omental injuries (omental injury and/or emphysema) of the Veress needle entry technique.
The risk of multiple insertions, seen in Figure 5, which includes four studies (n=1664), was significantly higher in the VN group with a pooled RR of 2.99 (95% CI 2.11–4.23). The rate of failed entry among four studies (n=1628) was likewise higher in the VN group with a pooled RR of 2.21 (95% CI 1.07–4.56) (Fig. 6).
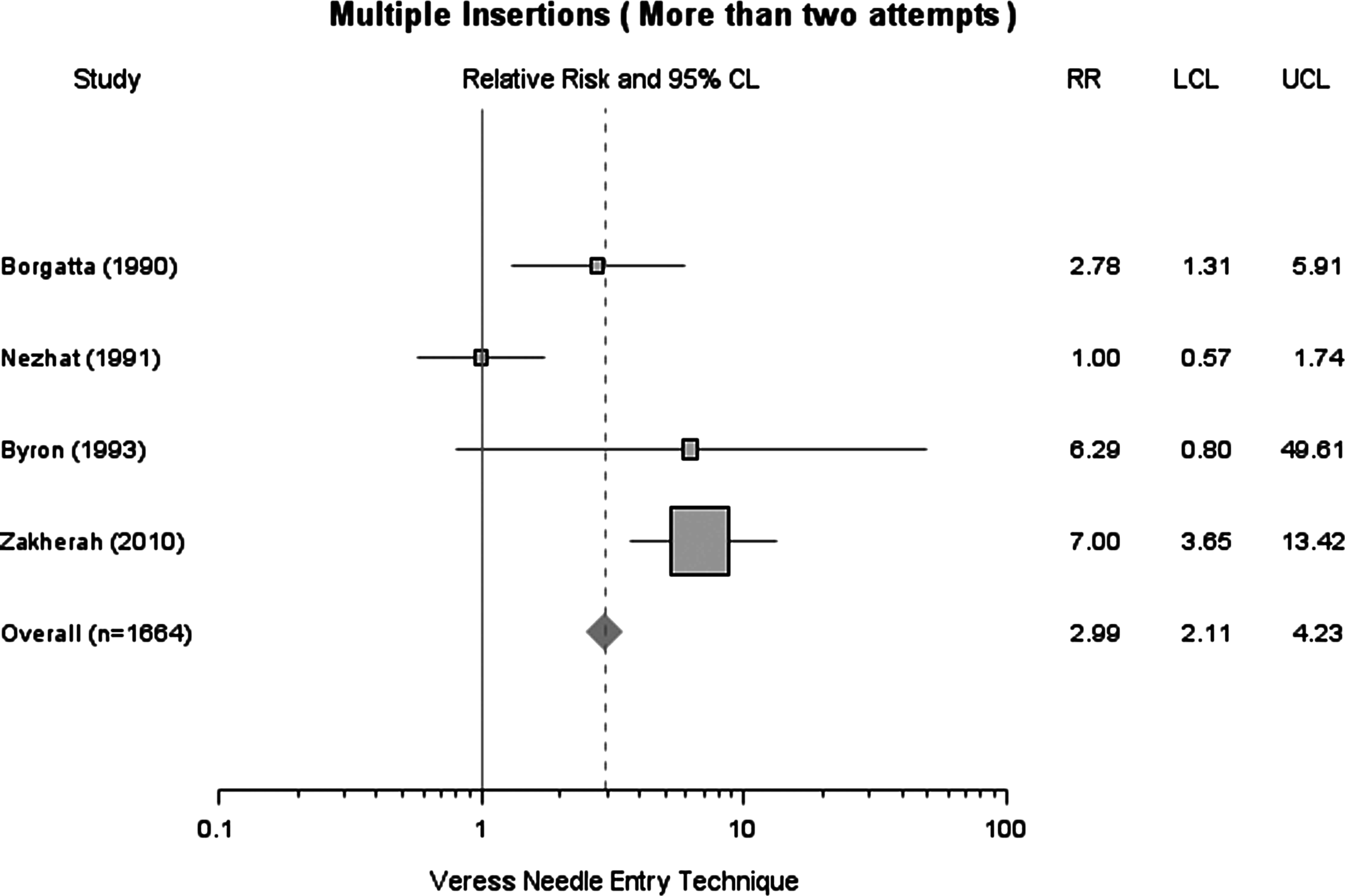
This forest plot depicts the RR of multiple insertions of the Veress needle entry technique.
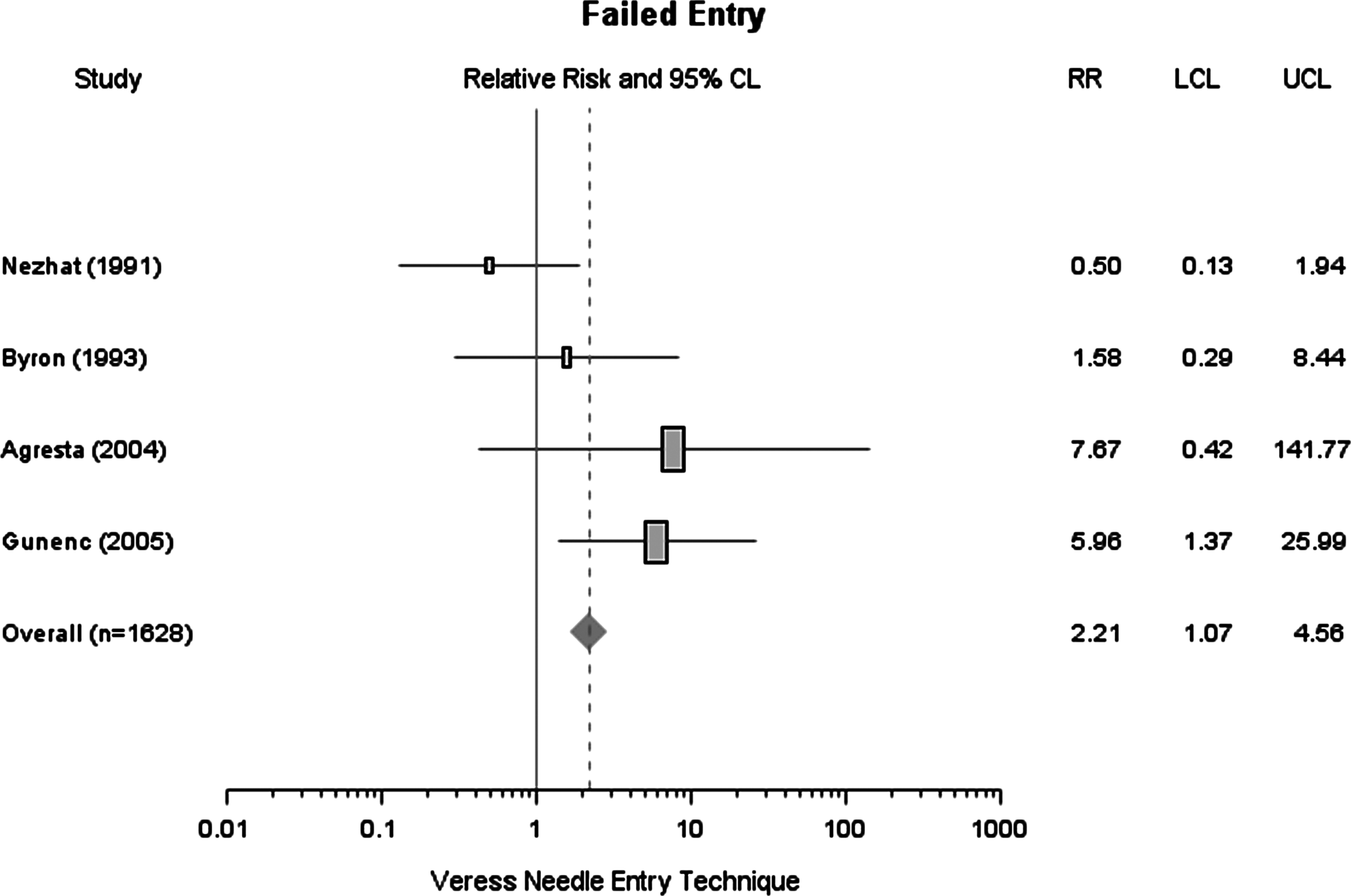
This forest plot depicts the RR of failed entry of the Veress needle entry technique.
Discussion
Veress needle entry
The Veress needle was developed in 1938 and remains the most commonly used technique for establishing a pneumoperitoneum. 9 The VN technique began with a blind insertion of the Veress needle followed by the introduction of several needle safety tests to confirm the pneumoperitoneum. The Veress needle is then removed after successful gas insufflation, followed by a blind insertion of the primary trocar.
Access-related major complications are rare during laparoscopic surgery; hence, this meta-analysis was underpowered to detect a significant difference in this safety outcome. Conclusive evidence about major complications related to the DTI relative to the VN would require a multicenter randomized controlled trial with over 10,000 patients in each study arm. 18 Although this is unlikely to be cost-effective or feasible, possible associations and trends identified through meta-analyses such as the current study, therefore, can be valuable. Although no statistically significant difference was identified in major complications between the VN and the DTI techniques, all four major complications occurred in the VN group. These complications included two hepatic injuries, one misdiagnosed ileal perforation, and one mesenteric laceration. A meta-analysis of 51 studies including retrospective, prospective, and randomized trials was performed and included 134,917 VN, 21,547 open, 16,739 DTI, and 679,847 unidentified entry techniques. 9 The results of this study identified a total of 10 deaths. An important finding was that all five entry-related deaths were in the VN group; the other five deaths were reported in the nonspecified group with three attributed to gas embolism and two to undiagnosed bowel perforation (trocar related). This analysis also reported that entry-related bowel and vascular injuries are rare with estimated prevalences of 0.4/1000 (VN) versus 0.5/1000 (DTI) and 0.4/1000 (VN) versus 0/1000 (DTI), respectively. 9
It was originally hypothesized that the Veress needle would cause less major injury to intraabdominal structures, such as bowel and vessels, because of the smaller diameter of the instrument. 9 This assumption has not been supported by either previous studies 9 or the current meta-analysis. Veress needle–related major injury to the great vessels is still the main cause of death during laparoscopic procedures. 33 This analysis revealed that the VN technique was associated with a statistically significantly increased risk of preperitoneal injuries and omental injuries. The increased risk with the VN technique was generally caused by incorrect placement of the Veress needle.
Different needle safety tests have been described, including the aspiration test, injection test, recovery test, saline drop test, and initial intraperitoneal pressure test. 34 The pressure test is most reliable to determine both correct and incorrect needle positioning. Other tests may yield false-positive or false-negative results, which may lead to complications due to unrecognized incorrect needle placement. 34 In the current analysis only one study clearly described the technique utilized for confirmation of needle positioning, with that being the pressure test. 29 Preperitoneal insufflation may also result in increased difficulty with subsequent insertion of the primary trocar, contributing to multiple insertions, failed entry, and longer operating times. Consistent with this, the VN group, compared with the DTI group, had a significantly increased risk of multiple insertions and failed entry. Of the women with multiple insertions (more than two attempts), the risk of preperitoneal insufflation was 50%. 35
The VN compared with the DTI technique consists of three blind steps, two blind entries, and one blind gas insufflation. Because the Veress needle is normally removed prior to the primary trocar insertion, a needle injury can remain undetected for a prolonged period of time. Blind gas insufflation may further explain a higher incidence of preperitoneal insufflation, subcutaneous and omental emphysema, or a gas embolism in the worst-case scenario.
DTI
The DTI technique, without pre-insufflation, is probably the least used entry technique. It requires elevation of the anterior abdominal wall with the nondominant hand while inserting the primary sharp trocar directly and blindly towards the peritoneal cavity. Once the tip of the trocar has been inserted through the skin incision, the trocar is pushed through the fascia and the muscle layer by a continuous twisting motion with constant downward pressure, so that the surgeon can easily realize when the trocar has pierced the peritoneum and entered the peritoneal cavity. The CO2 gas stopcock must be kept open during the insertion, to relieve the negative intraabdominal pressure as soon as the vented trocar tip enters the sealed peritoneal space. It is postulated that the viscera falls off its parietal apposition prior to contact with the advancing primary trocar. Once the successful trocar placement is verified by a laparoscope, CO2 gas is insufflated under direct visualization at a pressure of 15 mm Hg.29,30,36
Compared with the VN technique, the DTI reduces the number of blind steps from three to one. Besides the obvious advantage of less blind entries, this also theoretically reduces the complications related to the blind air insufflation used in the VN technique, hence less preperitoneal insufflation, subcutaneous or omental emphysema, needle-related vascular or visceral injuries, gas embolism, or delayed diagnosis of a bowel injury. More extensive subcutaneous emphysema could extend along contiguous fasial planes to the neck; such a finding can be a reflection of the development of mediastinal emphysema, which, if severe, may lead to pneumothorax and cardiovascular collapse. 37 In addition, this entry method does not rely on a secondary confirmation test, but emphasizes focus on the surgical technique, anatomical knowledge during laparoscopic entry, and immediate confirmation by direct visualization. 38 The DTI also results in a lower risk of multiple insertions and failed entry.
Previous abdominal surgery
Although previous abdominal surgeries would be a confounding variable, there was no significant difference between the two groups regarding the number with a prior abdominal surgery: 213 (28%) in the VN cohort and 216 (30%) in the DTI cohort. Despite prior abdominal surgery being a risk factor for laparoscopic entry complications, none of our selected studies did subgroup analyses for this. Whether DTI can significantly reduce the risk of complications in those who have a history of prior abdominal surgery, therefore, remains a question to be answered.
Obesity
Obesity is another risk factor for complications related to laparoscopic entry. Body mass index, however, was only reported in four out of the seven selected studies (n=1898, 65% of the total sample size) with an average body mass index of less than 30 kg/m2. Hence, the results of this meta-analysis should be interpreted with caution in the obese patient population. Theoretically, obesity may account for a higher incidence of preperitoneal placement, multiple insertions, and failed entry in the VN group due to increased thickness of the abdominal wall and more blind insertions and gas insufflation. Despite this suggestion, the study conclusions cannot be generalized to obese patients.
Adequate allocation concealment seeks to prevent selection bias in randomized studies. Only one study in this analysis clearly described allocation concealment, 29 and hence this is a limitation. Although unclear allocation concealment in randomized controlled trials tends to bias results in favor of a beneficial effect, this is done for subjective, as opposed to objective, outcomes. 39 Because the complications of laparoscopic entries are determined objectively by direct visualization, it is less likely that unclear allocation concealment introduces a significant bias exaggerating the complication of one technique over the other. In addition, no studies conducted secondary analyses comparing the safety of the two entry techniques in subgroups of low-risk and high-risk patients. Because both obesity and prior abdominal surgery are risk factors of laparoscopic entry complications, it would be helpful to know the proportion of these high-risk patients in each study arm of the included studies. This piece of information, however, is lacking in several studies.
Currently, no laparoscopic entry technique is without the potential of a complication. Furthermore, successful and safe laparoscopic entry depends largely upon a surgeon's experience, comfort level, and individualized techniques. For these reasons, it is important that surgeons do not abruptly or hastily abandon the entry technique they are comfortable with. To identify or develop the safest approach for laparoscopic entry remains a challenge. The goal of this meta-analysis, therefore, was to reevaluate the safety of the most widely used VN technique, which may not be the safest approach for laparoscopic entry. Multiple blind insertions and air insufflations certainly carry the risk of complications. The DTI technique was introduced as a safe alternative to the Veress needle entry technique to reduce Veress needle–related complications, which has been suggested by previous studies9,36 along with several meta-analyses of randomized studies,18,19 including the current report.
Footnotes
Disclosure Statement
No competing financial interests exist.