
Abstract
Abstract
Small numbers of hiatus hernias are very large, cause other nonreflux symptoms as well, and have an attached morbidity and mortality through strangulation. Patients are elderly and unfit, and surgery has been troubled by recurrence. Mesh repair has been advocated in an attempt to reduce a perceived high revision rate. We describe the early results of a “composite” form of laparoscopic repair where no mesh has been used, with excellent early results in levels of symptom control, morbidity, mortality, and recurrence, and discuss the value of mesh repair as a primary operation against the recently recognized severe complications secondary to mesh repair failure. The technique requires five-port laparoscopy, primary nonabsorbable diaphragmatic repair, and fixation of the cardioesophageal junction, within a fundoplication, to the posterior crural repair and median arcuate ligament. Thirty-eight patients with a mean age of 70 years operated on during 1 year had a recurrence of 6% but of minimal size by objective measure between 4 and 19 months of operation. Mesh repair in the literature is poorly supported, highly complicated, and by these figures not required.
Introduction
GHH may cause typical symptoms of gastroesophageal reflux due to the failure of antireflux mechanisms. Patients, however, present with atypical symptoms such as chest pain, epigastric pain, dysphagia, dyspnea, vomiting, anemia, early satiety, and acute strangulation, in more than 50% of cases. 2 Frequently the atypical symptoms often precede strangulation and catastrophic complications.3,4 The aim of repairing GHH is to prevent anatomic recurrence, symptoms, and complications secondary to strangulation and volvulus. Substantial improvement occurs in quality of life.5,6
Numerous surgical techniques have been described over the years, with mixed reports of success.7–9 The current accepted principles of repair include reduction of the stomach or hernia contents, excision of the hernial sac, approximation of the pillars of the hiatus, and possibly gastropexy. 10 Edye et al. 7 have particularly advocated excision of the hernia sac in reducing the technical failure of paraesophageal hernia repair, as have Watson et al. 9 There is a frequent association between reflux and GHH, and so fundoplication has been frequently performed as part of GHH repair. 11
Recurrent herniation following repair of GHH has remained problematic. Hashemi et al. 12 reported a 42% recurrence rate in laparoscopic repair of large Type 3 hiatus hernia. A further confounding factor has been apparent in that anatomical recurrence may not necessarily be symptomatic. Therefore studies based only on symptomatic recurrence may significantly underestimate the true rate of herniation, as has frequently been noted in the literature.13–15
Recent techniques of surgical repair have described the use of mesh in an attempt to decrease recurrence rates. However, there are various complications that arise from the use of mesh, such as intralumenal erosion, ulceration, stricture, dysphagia, and perforation. Stadlhuber et al. 16 found 17 of 28 mesh repairs needing re-operations had developed mesh erosion, 6 developed stenosis, and 5 developed fibrosis. Esophagectomy was required in 6 cases and gastrectomy in 3 cases. There was no apparent relationship between the type of mesh utilized primarily (including biological). Tatum et al. 17 reported 2 cases of mesh esophageal perforation requiring total gastrectomy.
No ideal surgical technique of GHH repair has been reported. Preferably, the ideal operation should have low morbidity and recurrence rates, no requirement for the use of mesh, elimination of the risk of strangulation, and a sustained improvement in quality of life of the patient. In this study, we report a technique that may approach satisfaction of these criteria. We evaluated the early outcomes of a modified Menguy posterior esophagogastropexy fundoplication 18 in GHH performed by a single surgeon (G.L.F.) from May 2009 to April 2010.
Patients and Methods
A consecutive series of symptomatic patients with Types 3 and 4 GHH underwent laparoscopic repair by intention to treat between May 2009 and April 2010. The patients were prospectively recorded on a computer database (Excel®, 2003; Microsoft Corp.). The database has received institutional ethical approval from 1992 onward, with the most recent being CH62/6/2011-092. The data recorded included patient demographics, hernia size (as a percentage of stomach in the chest), contents of the hernia, Gastrointestinal Quality of Life Index including a reflux score, 19 a validated dysphagia score, 20 and Visick score, 21 recorded on a self-administered proforma. Preoperative motility disorder was graded according to categories based on a grading by Kahrilas et al. 22 Data cleaning was performed by the research assistant (S.E.F.) to verify the results against hospital and clinical records and to complete postoperative data collection. All patients underwent the modified laparoscopic composite fundoplication-gastropexy described herein.
Statistical analysis was by Graphpad Prime software (GraphPad Software, Inc., San Diego, CA), using the Wilcoxon paired-ranks test for Visik grading and Spearman one-tailed correlation coefficient for the observed change in quality of life scores.
Technique
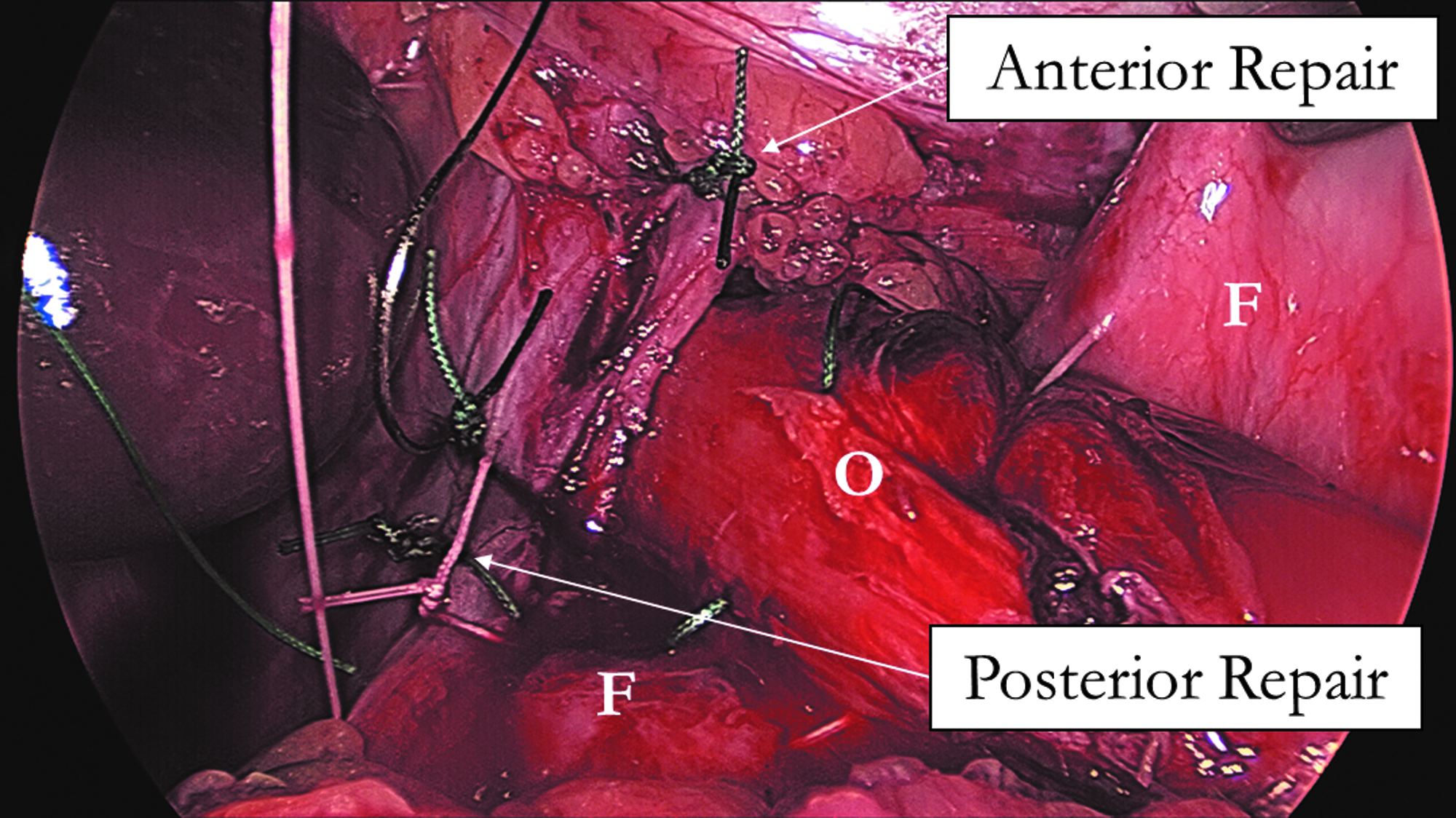
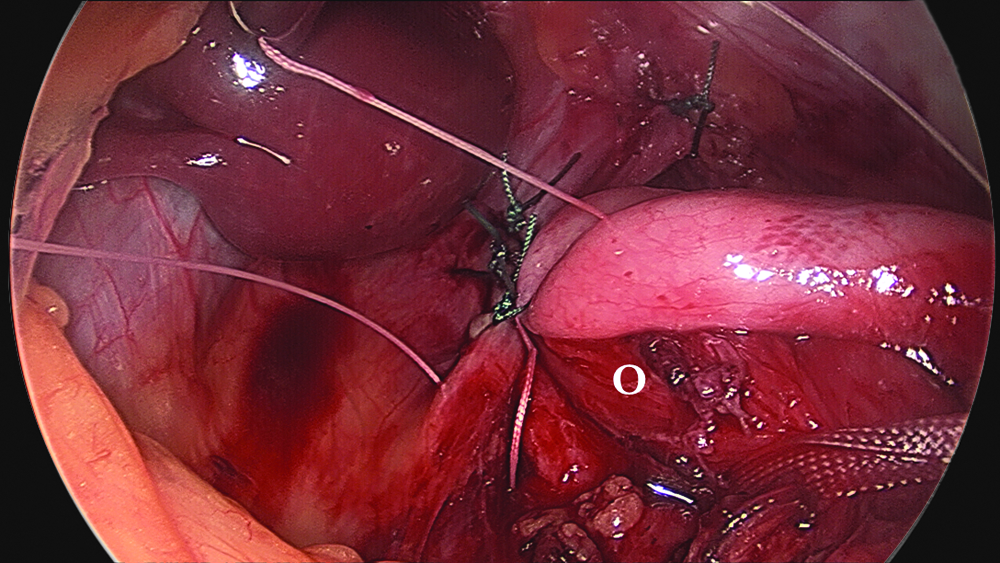
The technique was standardized for all patients and comprised a laparoscopic five-port approach in lithotomy with fixed liver retraction. The hernia was reduced, the sac was excised, and the esophagus was mobilized circumferentially and extensively in the chest to enable up to 3 cm of tension-free intra-abdominal esophagus (Fig. 1). The pillars of the crura were repaired posteriorly (Fig. 2), and at least one suture was placed anteriorly in the central tendon of the diaphragm in all patients. A composite fundoplication esophagogastropexy was performed, with three sutures passing through the anterior stomach to the esophagus and then to the posterior fundic wrap incorporating the posterior crural repair and median arcuate ligament (Fig. 2). Further fundophrenopexy sutures were placed anteriorly and laterally between the stomach and the diaphragm. The repair was calibrated with a 56 Fr bougie in the main, and in small females with 52 Fr bougie.
Repair of the diaphragmatic crura, with deep sutures to white line. F, fundus; O, esophagus.
Repair with composite approach incorporating two layers of stomach esophagus (O) and crural pillars.
Tension in the hiatal repair and the length of tension-free abdominal esophagus was recorded as judged by the surgeon.
Objective measures of esophagitis and recurrence were taken postoperatively by endoscopy between 6 weeks and 3 months postoperatively. Those who declined a postoperative endoscopy were asked to have a barium meal. Symptom proformas were completed predominately by self-administration at clinic visits but occasionally by post or phone.
Results
In total, 38 patients with a mean age of 70.7 years (range, 54–93 years) underwent operations from May 2009 to April 2010. There were 27 female patients. Hiatus hernia types were 33 Type 3 GHH and 3 Type 4 GHH (2 were not recorded). Follow-up consultation was on average 9 months (range, 4–19 months) after operation. The average amount of herniated stomach preoperatively was 68% (range, 30%–100%). The hiatus was graded as very large in 36 patients. There was no mortality. There was one conversion to laparotomy (obese, Type 4 hernia, 100% gastric herniation). Tension-free hiatus repair was possible in 28 patients; some tension was recorded present in 4 cases and not recorded in 6 patients. The diaphragm was adequately repaired in all patients. No patient had a short esophagus, and adequate length of abdominal esophagus was always easily obtained. Complications were recorded in 3 patients (1 bronchitis, 1 severe cardiorespiratory requiring prolonged ventilation support in the laparotomy patient, and 1 postoperative vomiting).
Small anatomical recurrences were confirmed by endoscopy in 2 patients, both having esophagitis. Esophagitis occurred in 3 patients in total. The recurrences took the form of minor telescoping of the cardio-esophageal junction (1 cm) upward, leaving the fundoplication subdiaphragmatic. Follow-up has been declined by 2 patients or relatives, because of frailty. No patient has required recurrent hernia repair, and all esophagitis has been controlled by medical means.
Symptom assessment was obtained using QOL questionnaires using the Gastrointestinal Quality of Life Index (Table 1). The score recorded no dysphagia. However, using the validated scoring system of Dakkak and Bennett, 20 the average preoperative dysphagia score was 36.5, and the average postoperative dysphagia score was not significantly different, at 37.8 (no dysphagia=45). The average preoperative modified Visick score was 2.9, and the average postoperative modified Visick score was significantly improved to 1.6 by 6 months (P=.0084 Wilcoxon).
Quality of life (QOL) at 6 months: Spearman correlation coefficient, one-tailed (P=.0058).
Standard deviation in parentheses.
By Wilcoxon paired-ranks test.
Quality of life was quite impaired in patients preoperatively. Scores improved significantly postoperatively; however, 5 patients suffered worsening scores. In the 3–6-month review there was no record for 3 patients. One patient was lost to follow-up, and 2 refused further interview because of frailty and dementia.
There was no change in the frequency of preoperative and postoperative dysphagia. Preoperative esophageal body peristalsis was graded according to the categories of Kahrilas et al. 22 for ineffective esophageal peristalsis (IEM) in 35 patients. Nonspecific abnormality of motility was found in 30 patients, graded normal in only 3, minor in 9, and moderate to severe in 23.
Postoperative worsening of dysphagia was unrelated to the presence of any level of IEM (1 normal preoperative motility, 4 mild abnormality, and 3 moderate/severe abnormality).
Discussion
There was a low recurrence rate using this method of GHH repair (5.3%, 2 of 38 patients). There was no requirement for surgical revision, and the small number of symptomatic patients was well controlled on medication for heartburn and esophagitis. There was a high rate of IEM, being a concern for dysphagia theoretically but not seen often empirically.
Recurrence following GHH repair has infrequently required re-operation,5,6,16,23–25 with adequate patient satisfaction and symptom improvement. In our previous experience small recurrence has been found to be a stable situation over years. 26
Therefore the number of patients requiring reoperation when mesh has not been used primarily is small despite the high number of objectively diagnosed recurrences elsewhere, and resection has rarely been required.23,25,27
Reports at meetings in both the United States and Australia have anecdotally highlighted the difficulty of revision surgery in the presence of mesh 28 (personal communications to G.L.F. at the 2011 Royal Australasian College of Surgeons Meeting, Adelaide, Australia). Re-operation in the presence of hiatal mesh has also been reported as highly morbid,16,17,29 and in the largest report of fundoplication-mesh revision 9 of 28 patients required resectional surgery. Another report has also recommended avoiding mesh repair for this reason. 30
Our own experience using Teflon® (Dupont) pledget reinforced fundoplication was repeatedly complicated by lumenal penetration even when the mesh was not used in a high-tension and mobile area, but simply on the gastric fundoplication.31,32 The delay to presentation was often longer than a decade, indicating mesh at the hiatus may present complications at a delayed time period, so studies of less than 5 years may greatly underestimate potential problems. Indeed, one may speculate that the incidence of mesh-related complication is yet to reach a zenith.
Biological prostheses have been used in the hope that mesh-related complications may not occur.14,33 Such procedures have not proven adequately durable in a randomized study, and even mesh arm recurrence rates are higher than we report when not using mesh, increasing with duration of time from operation (54% at 58 months).14,33
It would therefore seem that the use of mesh, synthetic or biological, may expose many patients to severe complications, 95% of whom would never seem to have had any need of mesh. A primary operation similar to the one described herein would appear to offer lower recurrence rates, further decreasing the already low re-operation rates, and expose a minimal number of patients to the risk of severe mesh-related complication and poor outcome.
So-called “short esophagus” can be avoided in this situation by adequate esophageal mobilization, which by these results can be seen feasible. It is the senior author's view that short esophagus is very uncommon in GHH and used to reflect esophageal shortening by esophagitis prior to the use of proton pump inhibitors.
Perhaps therefore either a selective approach to mesh repair at the primary operation, or those requiring re-operation could undergo mesh repair selectively at that stage, may reduce the total numbers of patients put at mesh-complication risk. Although small randomized studies have shown good results in a few patients, 13 larger studies of more than 500 cases have been disappointing, resulting in a likelihood of reoperation. 27
A modified “Menguy” approach was chosen because of the ability to fix the esophagus posteriorly and because the Hill operation in these circumstances had suggested low recurrent hernia in GHH patients during the open era. Additionally. it was evident the stomach became “fixed” further away from the hiatus—theoretically, therefore, not relying so greatly upon absolute hiatal integrity for stability. The value of these operations will only became apparent (or not) by persistent review.
The study had several limitations of general applicability. The number of patients in the study was moderately small and was based on a single surgeon's experience, which standardized the method of repair, but had yet to show universal value in many hands. The follow-up period was short, and continued monitoring over a longer time period and with more patients may show an increase in recurrence rates, and possibly revision surgery, although it has frequently been reported most recurrences occur within 2 years.
Conclusions
The outcome of a technique of GHH repair using objectively diagnosed recurrence is reported. There was a low recurrence rate using the modified Menguy technique and minimal complications especially when performed by laparoscopy. There was no case of short esophagus. It appeared this technique could be used in patients with IEM without undue dysphagia. There has been a significant improvement in quality of life and Visick scores postoperatively. This method of GHH repair has shown early promise as a safe and effective method of performing GHH repair without the risk of using mesh. The risk of mesh repair for all does not appear justified.
Footnotes
Disclosure Statement
No competing financial interests exist.