
Abstract
Abstract
Background:
This article reports our early experience with the use of lidocaine patches for pain control in the immediate postoperative period after laparoscopic gynecologic surgery.
Subjects and Methods:
A prospective, double-blind, placebo-controlled clinical trial was conducted on 40 patients undergoing a gynecologic laparoscopy who were randomized to receive either topical patches of 700 mg of lidocaine (n=20) or placebo patches (n=20). The patch was divided evenly into four smaller patches, which were applied at the four port sites and changed every 12 hours for 36 hours after surgery. Postoperative pain was evaluated using the visual analog scale (VAS) score and the Prince Henry and 5-point verbal rating pain scale (VRS), and the analgesic requirement was also evaluated at 1, 6, 12, 24, and 36 hours after surgery.
Results:
The VAS score for wound pain was lower in the lidocaine patch group at 1 and 6 hours after surgery than the control group (P=.005 and <.0005, respectively). The VAS scores for postoperative pain were lower in the lidocaine patch group at rest 1 hour after surgery (P=.045). The 5-point VRS score for postoperative pain was lower in the lidocaine patch group at 6 and 12 hours after surgery (P=.015 and .035, respectively) than in the control group.
Conclusions:
Topical lidocaine patches at the laparoscopic port sites reduced postoperative pain, particularly postoperative wound pain after gynecological laparoscopic procedures.
Introduction
Pain after gynecologic laparoscopic surgery results from shoulder pain induced by an irritation of the diaphragm by dissolved carbon dioxide and port site pain caused by the holes in the abdominal wall.2,3 Because benign gynecologic laparoscopic surgeries usually have a relatively short operation time and less irritation of the bowel, the primary pain after such surgeries may be port site wound pain. The shoulder pain associated with peritoneal insufflation can be reduced by carbon dioxide emissions from the intraperitoneal cavity using a laparoscopic suction tool and by the application of intraperitoneal local anesthetics. 4 On the other hand, for port site pain control, there are few data with effective outcomes.
Systemic analgesics continue to be the main source of postoperative pain control but may cause side effects, such as nausea, vomiting, delayed intestinal movement, and discomfort. Topical analgesics are applied locally and directly to painful areas, and their sites of action are local to the site of application. The pharmacological activity of topical analgesics, which is, in contrast to systemic analgesics, directed locally to the site of application, helps minimize the risk of significant adverse effects and drug–drug interactions. 5 Although the mechanism of action of topical analgesics may be largely within the peripheral nervous system, their effect on the peripheral processing of pain transmission may lead to a decrease in the central pain mechanisms. If less pain-producing information arrives from the periphery for central processing, it is likely that fewer central mechanisms will be activated. 6
The 5% lidocaine patch is a targeted peripheral analgesic approved by the Food and Drug Administration for the treatment of postherpetic neuralgia. 7 The efficacy of the lidocaine patch in other neuropathic and nonneuropathic pain conditions has also been demonstrated.8,9 However, there are few reports on the effect of a lidocaine patch on acute postoperative pain, especially port site wound pain. Moreover, little attention has been paid to laparoscopic-specific wound pain control. Besides, the use of a lidocaine patch to reduce the postoperative pain has several advantages in terms of simplicity, and it is a low-cost and noninvasive method, with few systemic effects. It also provides regular and continuous administration, in contrast with single-shot port site administration of local anesthetics.
Therefore, this study examined the effectiveness of 5% topical lidocaine patches for postoperative pain, including port site wound pain, after gynecologic laparoscopic surgery.
Subjects and Methods
This randomized, double-blind, placebo-controlled study included 40 women, 21–51 years old, who underwent elective gynecological laparoscopic procedures (laparoscopic-assisted vaginal hysterectomy, n=20; laparoscopic myomectomy, n=20) at Cheil General Hospital and Women's Healthcare Center (Seoul, Korea) between January 2010 and March 2010. The patients were status I–II according to the criteria of the American Society of Anesthesiologists. Patients with an allergy to any drug or who had renal insufficiency, taken any analgesic within a 24-hour period before surgery, or a gastroduodenal ulcer were excluded. The Institutional Review Board approved the study, and informed consent was obtained from all patients.
The 40 consecutive patients undergoing laparoscopic-assisted vaginal hysterectomy and laparoscopic myomectomy were assigned randomly to one of two groups using a computer-generated random number table. The study patches were sealed in an opaque envelope labeled with the randomization numbers and given to the surgeon at the end of surgery. Each consenting patient received a consecutive randomization number. No person was aware of the group assignment until all the patients had been included and assessments were completed.
All procedures were performed by a single surgeon using the same technique, under general anesthesia. No premedication was used. Anesthesia was induced with thiopental sodium (5 mg/kg), and tracheal intubation was facilitated with rocuronium (0.6 mg/kg). Anesthesia was maintained with sevoflurane (1.5%–2.5%) in 60% nitrous oxide/oxygen. Ventilation was controlled mechanically and adjusted to maintain an end-tidal CO2 value of 35–45 mm Hg throughout surgery. Additional rocuronium was administered as needed. A residual neuromuscular blockade was antagonized with pyridostigmine at 10 mg and glycopyrrolate at 0.4 mg.
The lidocaine group was administered a 700-mg, 5% lidocaine patch (Lidogesic®; ICURE Pharmaceutical, Inc., Sungnam City, Korea) (10×14 cm) that was divided evenly into four smaller patches (5×7 cm) and applied to the four port sites after surgery. Before the lidocaine patches were applied, each port site was covered with sterile Steri-Strip™ (3M™, St. Paul, MN) tape (2×2.1 cm) to avoid direct wound contamination. The lidocaine patches were changed every 12 hours for 36 hours after surgery by a member of the surgical team who was not involved in this study. The placebo (control) patients received patches without lidocaine (ICURE Pharmaceutical, Inc.) (10×14 cm) under the same treatment schedule. The surgeon was not involved in any aspect of the data collection.
All patients received an intravenous injection of fentanyl (25 μg) 10 minutes after surgery. During the postoperative period, the routine management for pain reduction after surgery was not used.
Data were collected by study personnel who were unaware of the patients' randomization at 1, 6, 12, 24, and 36 hours, postoperatively. The primary outcome measure was the visual analog scale (VAS) score for postoperative wound pain and postoperative pain at rest and during ambulation. The other data collected included the Prince Henry Verbal Rating Scale (VRS) and 5-point VRS pain score for postoperative pain, shoulder pain, site of the most severe pain, and analgesic requirements.
Pain was monitored using a 10-cm vertical VAS score (from 0=no pain to 10=the most severe pain), as well as the Prince Henry VRS (no pain on coughing, score=0; pain on coughing but not on deep breathing, score=1; pain on deep breathing but not at rest, score=2; slight pain at rest, score=3; and severe pain at rest, score=4) and 5-point VRS (no pain on normally walking, score=0; pain on normal walking but not on slow walking, score=1; pain on slow walking but not on sitting, score=2; pain at sitting but not at rest, score=3; and pain at rest, score=4). The degree of postoperative pain at rest and postoperative wound pain, which is defined as superficial, localized abdominal wall port-site incisional pain, was assessed using the VAS pain score at 1, 6, 12, 24, and 36 hours postoperatively. The degree of postoperative pain during ambulation was also assessed using the VAS pain score at 6, 12, 24, and 36 hours postoperatively. In addition, the degree of postoperative pain was assessed using the Prince Henry and 5-point VRS pain scores. Shoulder pain was recorded at 1, 6, 12, 24, and 36 hours postoperatively. The site of the most severe pain was also recorded as the shoulder tip, the port site, inside the abdomen, pelvis, and back at the same time interval. The pain assessment was carried out by the same observer in all cases. If the patients requested additional pain control at any time, the VAS score was immediately recorded, and additional rescue pain control was administered if the VAS score was >5. Rescue pain control drugs consisted of ketorolac tromethamine (Tarasyn®, Bedford Laboratories, Bedford, OH; 15 mg, ½ ampule, intravenous injection), followed by meperidine (Demerol®; Hospiral, Inc., Lake Forest, IL) (½ ampule, 25 mg, intravenous injection) if the first rescue pain control was insufficient. The analgesic requirements were also evaluated at 1, 6, 12, 24, and 36 hours after surgery. At 36 hours, the patients were asked to rate the satisfaction with pain control (5-point scale: very satisfied, somewhat satisfied, neither satisfied nor dissatisfied, somewhat dissatisfied, and very dissatisfied).
Postoperative nausea and vomiting were evaluated the same time interval (nausea on a scale of no=1, mild=2, moderate=3, and severe=4; vomiting, no or yes).
In addition, dermal reactions at the application site, such as erythema or rash, contact dermatitis, and systemic side effects of the lidocaine patch, such as hypotension, bradycardia, cardiovascular instability, headache, and dizziness, were reported. The patients and the investigators who collected the postoperative data were blinded to the randomization.
Based on previous experience from our department using the same trial method, it was assumed that a difference of 2 in the VAS pain score in postoperative wound pain would be clinically relevant (standard deviation of 2). Power analysis suggested that at minimum 16 patients per group were required for a β=0.2 and α=0.05 (two-sided). Twenty patients in each of the two groups were enrolled to compensate for potential dropouts.
All patients were assessed according to their demographic data, including body weight, operation time, morbidity, time between surgery and the first ambulation, individual pain scores, and the requirement of analgesics. The data were analyzed using SPSS version 16 (SPSS, Chicago, IL). Measures were tested with the Shapiro–Wilk test for normal distribution. An independent-samples t test and a Mann–Whitney U test were used for parametric and nonparametric analysis, respectively, to compare the differences between the two groups for each of the individual variables. To control the overall significance level at .05, we used the Bonferroni's adjustment to each test result. Proportions were compared using the Fisher's exact test. The numerical data are expressed as the mean±standard deviation values or median (range) as appropriate. A P value<.05 was considered significant.
Results
A flow diagram of patient distribution is displayed in Figure 1. Forty patients were enrolled. There were no significant differences between the two groups with regard to age, weight, disease, surgery type, operation time, ambulation time, and mean hospital stay (Table 1).
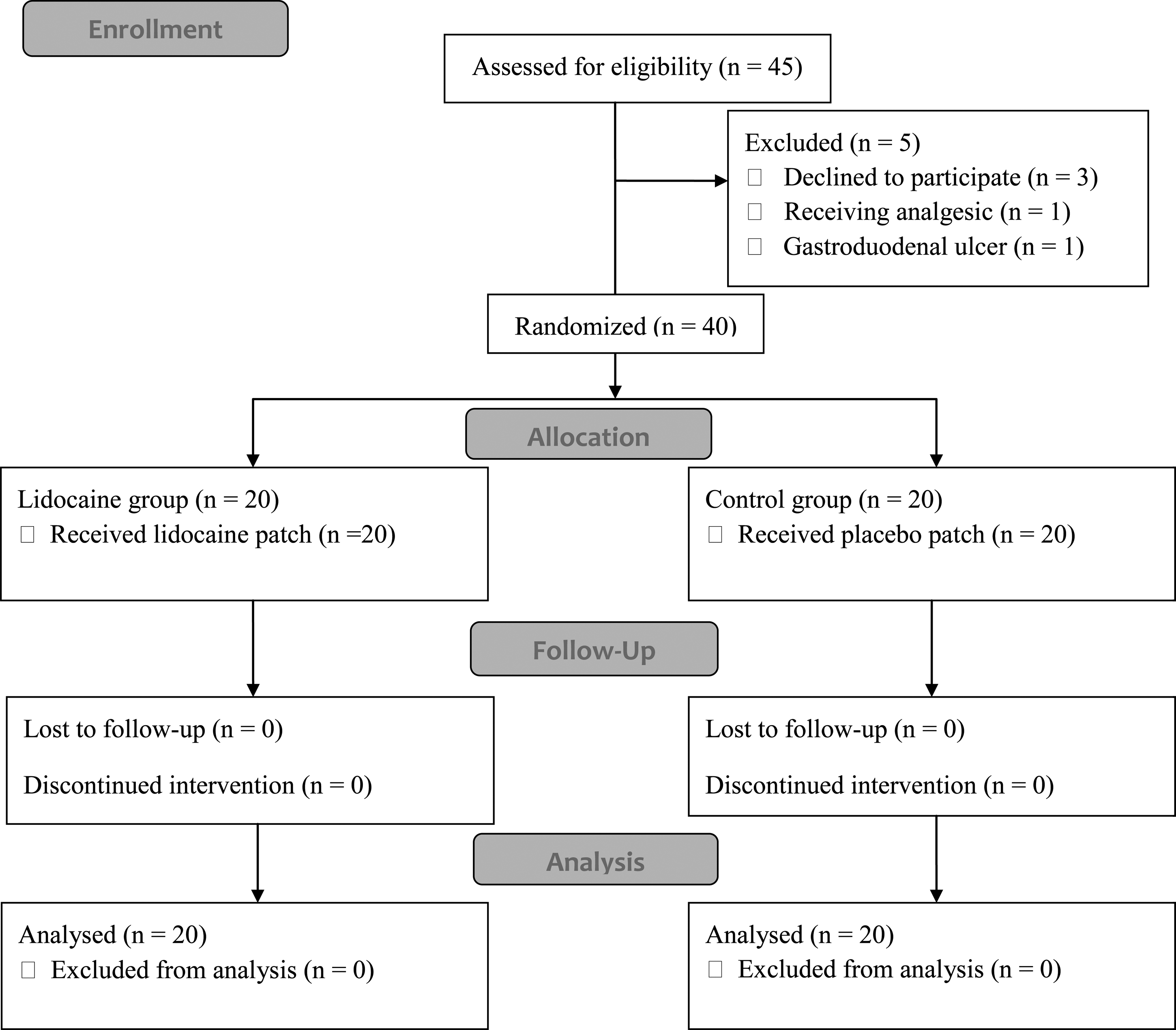
Flow diagram of patient distribution.
Data are mean±SD values or number.
CIS, Carcinoma in situ; LAVH, laparoscopic assisted vaginal hysterectomy; LM, laparoscopic myomectomy.
The lidocaine patch group reported a significantly lower VAS score for postoperative wound pain at 1 and 6 hours after surgery than the control group (P=.005 and <.0005, respectively) (Fig. 2). The VAS score for postoperative pain at rest was lower in the lidocaine patch group at 1 hour after surgery than in the control group (P=.045). The VAS score for postoperative pain during ambulation was not significantly different from that of the control group. The 5-point VRS score for postoperative pain was lower in the lidocaine patch group at 6 and 12 hours after surgery than the control group (P=.015 and .035, respectively), and the Prince Henry VRS score for postoperative pain was not significantly different from that of the control group. The mean pain scores decreased gradually in a time-dependent manner. There was no significant difference in shoulder pain and the site of the most severe pain (port site, back, shoulder, or inside the abdomen) between the two groups at all observation times.
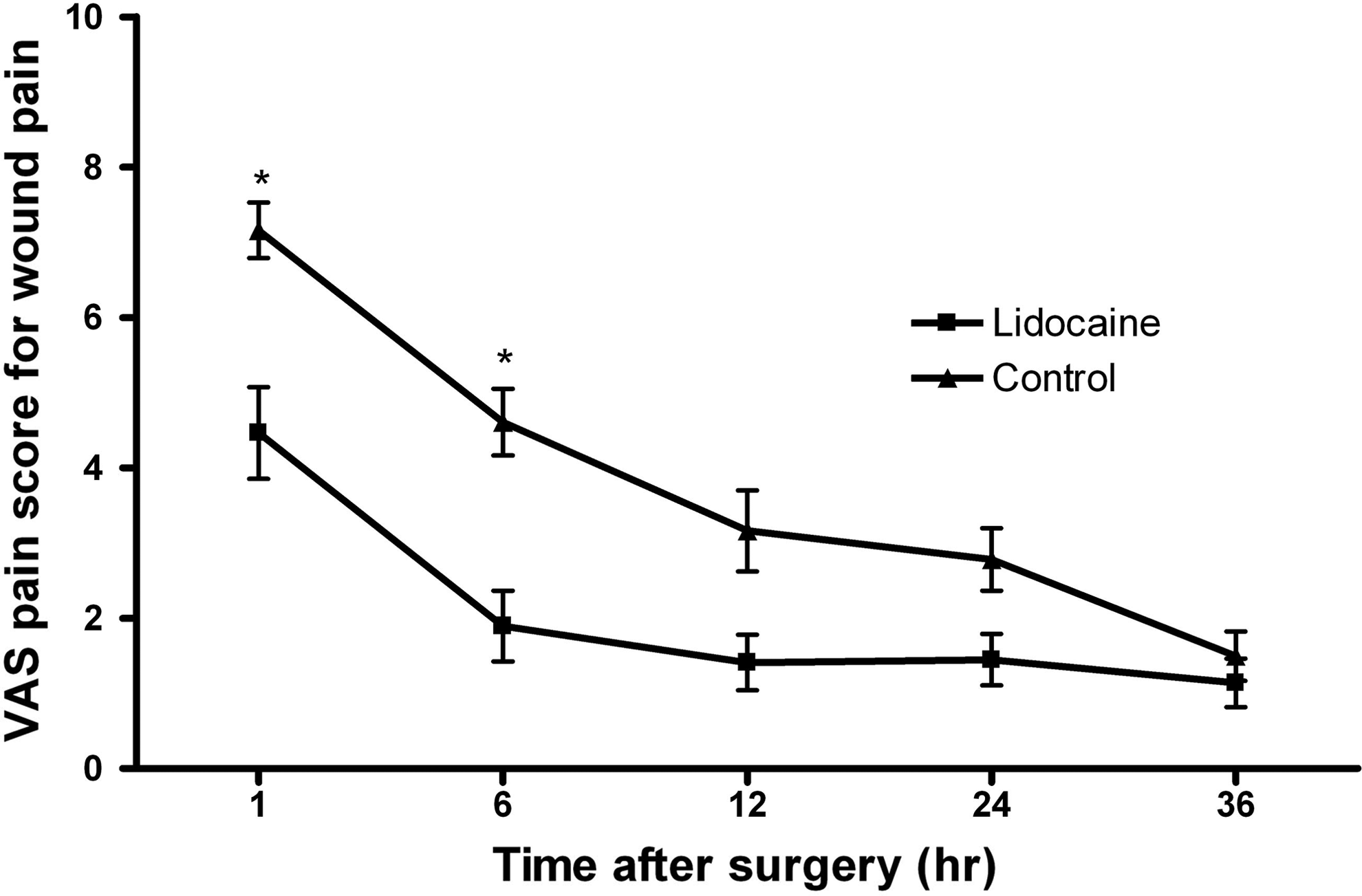
Visual analog scale (VAS) pain score for wound pain at the port sites. The comparisons were performed at 1, 6, 12, 24, and 36 hours after surgery. Data are mean±SD values. *P values are statistically significant at <0.05.
There was no significant difference in the requirement of analgesics between the two groups. The median amounts of ketorolac administered in the lidocaine patch group and the control group were 7.5 mg (range, 0–60 mg) and 20 mg (range, 0–60 mg), respectively (P=.117) (Table 2). The median amounts of Demerol administered in the lidocaine patch group and the control group were 0 mg (range, 0–25 mg) and 0 mg (range, 0–50 mg), respectively (P=.077) (Table 2). There was no significant difference in the satisfaction with pain control between the two groups. The postoperative nausea and vomiting were similar in the two groups at 1, 6, 12, 24, and 36 hours after surgery.
Data are median values (range).
No wound problems, contact dermatitis, and systemic side effects of the topical patches were reported in either group.
Discussion
This study demonstrated that 5% topical lidocaine patches reduced the level of postoperative pain, particularly wound pain, after gynecologic laparoscopic surgery. Topical 5% lidocaine patches did not cause a dermal reaction or systemic side effects.
Surgical treatment for benign gynecologic tumors has shifted from laparotomy to laparoscopy because of the less peritoneal injury and tissue trauma, less perioperative morbidity, less postoperative pain, and shorter hospital stays compared with a laparotomy. 1 Although gynecologic laparoscopic surgery is less invasive, a high incidence of postoperative abdominal pain has been reported. 10
Pain after laparoscopy can be differentiated into abdominal and shoulder pain 2 and is multifactorial in origin. Wound pain arising from the port sites, the surgical procedure, and the pneumoperitoneum itself may contribute to abdominal pain. Shoulder pain after laparoscopy is attributed to stretching of the subdiaphragmatic fibers of the phrenic nerve due to the increased concavity of the diaphragm, induced by the pneumoperitoneum and the resulting loss of visceral surface tension. 3 In the present study, all patients reported the site of most severe pain to be in the port site during the observation period. Therefore, wound pain control is very important for postoperative pain control. A 5% lidocaine patch reduced the level of postoperative wound pain at 1 and 6 hours after surgery.
The analgesic action of local anesthetic agents is related to the suppression of the activity of peripheral sodium channels within sensory afferents. This results in a decrease in ectopic, paroxysmal discharges and ultimately pain transmission. Local anesthetics also reduced the expression of mRNA for certain types of sodium channels.5,11 In addition, local anesthetics induce antinociception by inhibiting the release and action of proteolytic and inflammatory agents, which are released into the tissues after a surgical injury and stimulate the nociceptors, thereby activating and maintaining the level of postoperative pain. 12
The 5% lidocaine patch is composed of a soft, stretchy adhesive patch (10×14 cm) containing 5% lidocaine (700 mg) and is used for the topical treatment of pain associated with postherpetic neuralgia. 7 It is also effective in osteoarthritis, 13 low back pain, 9 diabetic polyneuropathy, 8 and carpal tunnel syndrome. 14
Two recent studies demonstrated the effect of lidocaine patches for postoperative pain after laparoscopic ventral hernia repair 15 and radical retropubic prostatectomy. 16 Habib et al. 16 reported that the 5% lidocaine patch reduced the pain scores in patients undergoing a radical retropubic prostatectomy under general anesthesia. The lidocaine patch group reported significantly less pain that interfered with walking, deep breathing, and mood than the placebo group. However, the patch did not reduce the level of opioid consumption, duration of hospital stay, and return of bowel function. Saber et al. 15 evaluated the use of a lidocaine patch for pain control in the immediate postoperative period after laparoscopic ventral hernia repair. In their study, the lidocaine patch reduced the postoperative pain score at discharge, but there were no significant differences in the postoperative analgesic requirement. These results are similar to those in the present study. The present study showed that the application of 5% lidocaine patches on the port site reduced the level of postoperative wound pain after gynecologic laparoscopic surgery. In addition, the application of 5% lidocaine patches on the port site also reduced the level of postoperative pain at rest. On the other hand, the postoperative analgesic requirement, duration of hospital stay, ambulation time, and satisfaction with pain control were similar in the two groups.
Ideal postoperative pain control effectively reduces the level of pain while minimizing the dose and adverse drug effects. Lidocaine patches deliver the drug directly to the site of pain, minimizing the systemic drug exposure and adverse effects. The amount absorbed is related directly to the skin surface area covered and the duration of lidocaine patch application. At least 95% (665 mg) of the lidocaine remains in a used patch, with absorption being 3±2% of the dose applied to healthy volunteers. 7 None of the known systemic effects of lidocaine, such as altered central nervous system or cardiovascular function, has been reported in patients using the 5% lidocaine patch. The most frequently reported adverse reaction was mild-to-moderate skin redness and rash or irritation at the patch application site. However, this reaction was associated with both lidocaine and vehicle patches.7,17 There were no wound complications related to the application of the patch or systemic side effects of the topical patches in this study.
Pain relief with a lidocaine patch is due to local action at the pain site rather than systemic lidocaine administration. Lidocaine blocks the voltage-gated sodium channels on the excitable membranes, thereby preventing the generation and conduction of nerve impulses and providing analgesic relief. 15
Animal studies suggest that systemic lidocaine might exert its analgesic effect by selectively suppressing the C-afferent fiber-evoked activity in the spinal cord 18 or by suppressing spontaneous activity in damaged peripheral neurons.19,20 As there is minimal systemic absorption of lidocaine from the 5% lidocaine patch, it is unclear if these mechanisms are relevant to the mechanism by which the patch exerts its analgesic effect.
The lidocaine patch also exerts its analgesic effect without producing local anesthesia. The skin underneath the patch continues to have normal sensation. The formulation was suggested to deliver sufficient amounts of lidocaine to block the sodium channels, reducing both the generation and conduction of peripheral pain impulses in damaged or dysfunctional nociceptors, but not sufficient to block the sodium channels on large myelinated A-β sensory fibers. 11
The onset of pain relief with the lidocaine patch has been reported to occur as early as 30 minutes after application in patients with post-therapeutic neuralgia. 21
The difference between the groups with regard to the pain score at the port sites decreased gradually with time and was no longer statistically significant 12 hours after surgery. In general, the pain scores at rest were relatively higher at 1 and 6 hours than at 12, 24, and 36 hours. This dependence of postoperative pain on time emphasizes the importance of postoperative pain control in the immediate and short term after laparoscopic surgery. Postoperative control of pain at 1 and 6 hours after surgery might require more powerful analgesics. The effective strategies for the diverse postoperative control of pain should account for time dependency.
In conclusion, lidocaine patches offer an effective, safe, and feasible alternative for managing postoperative pain, particularly wound pain after laparoscopic gynecologic surgery. However, a prospective, randomized, controlled, double-blinded study with a larger sample size will be needed to confirm the results of this preliminary study before lidocaine patches can be widely recommended for pain control after laparoscopic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.