
Abstract
Abstract
Colonic gas explosion, although rare, is sometimes a fatal iatrogenic complication in endoscopic procedures or laparotomic surgery, but it has not been reported during port incision of laparoscopy. We report a case of gas detonation in a patient with pneumatosis intestinalis and pneumoperitoneum, on opening the peritoneum with a diathermy for umbilical trocar insertion. Based on our experience, in cases of pneumoperitoneum, surgeons need to avoid using a diathermy in opening the peritoneum.
Introduction
Pneumatosis intestinalis (PI) is defined as the presence of gas in the bowel wall, which may be associated with pneumoperitoneum either as a benign condition or following perforation of a viscus.6,7 Most PI with benign conditions can be managed nonoperatively; however, sometimes it is quite difficult for surgeons to decide whether a patient needs emergency laparotomy. To manage patients with uncertain diagnoses, diagnostic laparoscopy can be performed as an adjunct to confirm bowel necrosis or hollow visceral perforation. 8
We report a case of gas detonation in a patient with PI and pneumoperitoneum, when we opened the peritoneum with a diathermy for umbilical trocar insertion.
Case Report
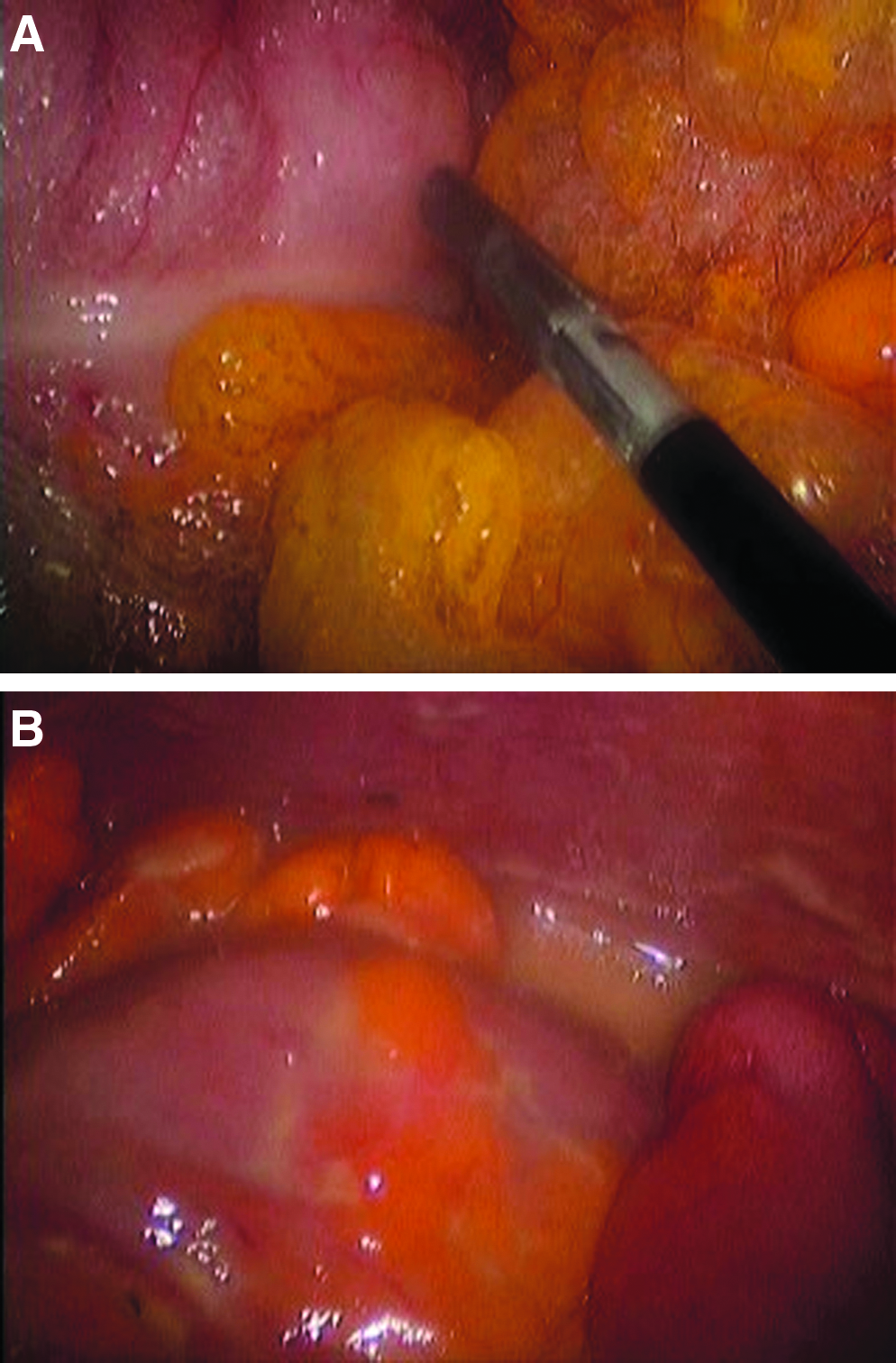
A 75-year-old woman with a past medical history of rheumatoid arthritis visited our emergency department because of generalized abdominal pain and melena for 7 days. Physical examination revealed tenderness over the whole abdomen, and her hemodynamic status was relatively stable. Laboratory tests revealed leukocytosis (13.9×109/L), mild anemia (hematocrit, 10.0 g/dL), and an elevated C-reactive protein level of 26.7 mg/L. The abdominal computed tomography scan showed generalized bowel distention, intramural air of the right colon, and massive intraperitoneal air (Fig. 1); an emergency laparoscopy was performed. When the peritoneum was opened with the diathermy for umbilical trocar insertion, a loud “pop” was heard, and the surgeon was blinded momentarily; a surgical glove of the operator was also burnt from the explosion. Luckily, the vital signs of the patient were stable. Laparoscopic exam revealed marked cystic changes in the right colon wall, partial ischemic changes in the transverse colon, and some yellowish thick discharge, but no bowel perforation was detected (Fig. 2). Loop ileostomy was conducted, and the patient was permitted diet on postoperative day 7 and was discharged uneventfully. Ileostomy repair was performed 2 months later.

Abdominal computed tomography scan taken on admission, showing generalized bowel distention, intramural air in the right colon, and massive intraperitoneal air.
Discussion
Colonic gas explosion, although rare, is one of the most fatal iatrogenic complications during therapeutic colonoscopy and laparotomic surgery. Three factors are necessary to trigger an explosion of colonic gas: presence of fuel (hydrogen, methane) produced by the fermentation of nonabsorbable carbohydrates in the colon by colonic bacteria, the presence of oxygen, and a heat source (electrocautery or argon plasma coagulation).4,9 The presence of an explosive mixture in the gas of the unprepared colon has been reported to be as high as 42.8%. 10 As therapeutic colonoscopy with electrocautery is widely used around the world, colonic gas detonation continues to occur on rare occasions.1,4 Therefore, to minimize this complication, good bowel preparation, the use of non–substrate-containing bowl preparations, suction of all pockets of colonic gas before diathermy, and insufflations using carbon dioxide instead of air have been recommended.1,4,9 Although much less frequent during laparotomic surgery, the occurrence of a massive colonic explosion during diathermy colotomy has been reported. Under bowel obstruction, the gas composition may change to include explosive concentrations of hydrogen and methane. 3 However, in most instances, colonic explosion has occurred after apparently adequate bowel preparation.2,11–13 Because some degree of colonic gas distension at laparotomy is usual, even in the absence of colonic occlusion, Altomare and Memeo 2 recommended never to use diathermy during colostomy to let gas escape. During laparoscopy, there is a possibility of instruments perforating the bowel resulting in release of flammable gases into the peritoneal cavity, increasing the chance of ignition by faulty electrical instrumentation. 14 There have been several reports of explosion during laparoscopy in which nitrous oxide was used as the insufflating gas. 15 Carbon dioxide is the gas used today for insufflation of the peritoneal cavity, having an advantage of a quenching effect on flammability.
PI is a secondary finding caused by an underlying disease. Mucosal integrity, intraluminal pressure, bacterial flora, and interluminal gas have an interactive role in the formation of the pneumocysts. 7 For patients diagnosed radiologically with PI, appropriate medical treatment should be adopted according to preexisting illness. The difficult task of determining the need for operative intervention is compounded by the presence of pneumoperitoneum, a finding that has been traditionally associated with perforation or bowel ischemia. In fact, the literature contains several studies of PI with pneumoperitoneum in which celiotomy was unnecessary.6–8 However, to manage patients with uncertain diagnoses, diagnostic laparoscopy can be an option to confirm bowel perforation or bowel necrosis.
To the best of our knowledge, there has not been any report of gas detonation in a patient with PI and pneumoperitoneum. At the same time, although the diagnostic approach has been frequently used in various surgical emergencies, gas detonation has not been reported during port incision of laparoscopy.
As mentioned above, fuel, oxygen, and heat source are the three factors necessary for explosion to occur. In our case, the fuel was present from the PI in the form of pneumoperitoneum, the source of oxygen may be atmospheric air, and the heat source was the diathermy used for opening the peritoneum.
Conclusions
Using diathermy on a distended colon has the potential of gas explosion, and one should avoid the use of diathermy to open the peritoneum in laparoscopy or laparotomy, where there is free gas in the peritoneal cavity.
Footnotes
Disclosure Statement
No competing financial interests exist.