
Abstract
Abstract
Purpose:
Obesity has been considered a potential risk factor for complications during laparoscopic surgery. The purpose of this study is to retrospectively investigate the association of various obesity indices and intraoperative factors in laparoscopic donor nephrectomy.
Patients and Methods:
This study included 70 and 44 patients who underwent laparoscopic donor nephrectomy by a transperitoneal approach and retroperitoneal approach, respectively. We measured fat thickness and fat areas on preoperative computerized tomography (CT) images. The median value of fat thickness or of the subcutaneous fat area, visceral fat area, perirenal fat area, or total fat area among subjects was used as a cutoff to define fatty and non-fatty groups. The operative time and estimated blood loss were then compared between the two groups.
Results:
In the transperitoneal approach group, there was no statistically significant difference in any of the indices or intraoperative factors between the fatty and non-fatty groups defined using any of the fat parameters. In the retroperitoneal approach group, patients in the fatty group categorized by perirenal fat thickness and visceral fat area had significantly greater estimated blood loss than those in the non-fatty group. Also, in the retroperitoneal approach group, patients in the fatty group categorized by perirenal fat area had significantly greater estimated blood loss and longer operating time than those in the non-fatty group (P=.02 and P=.014, respectively).
Conclusions:
The results indicate that the visceral fat, and in particular the perirenal fat area measured using CT scan imaging, influences operating time and estimated blood loss after retroperitoneal approach surgery but not in transperitoneal approach surgery. In donors with a high volume of perirenal fat, the transperitoneal approach may be recommended for laparoscopic nephrectomy.
Introduction
Meanwhile, degree of obesity has been reported to be associated with increased difficulty of laparoscopic nephrectomy, as reflected by a trend toward longer operative times and more intraoperative complications.1,2 Acceptance of obese individuals as living kidney donors is controversial because of possible increased risk of surgical complications. 3 A longer operating time places patients at an increased risk for elevated creatine phosphokinase activity and an increased percentage change in donor creatinine level. 4 Thus, care should be taken in choosing laparoscopic nephrectomy with severely obese donors until longer follow-up data are available. 5
Although body mass index (BMI) is widely used as an index of adult obesity, BMI does not distinguish between fat and muscle weight or between visceral and subcutaneous fat. We hypothesized that indices of body fat mass that were quantitatively measured on computerized tomography (CT) images could reflect intraoperative factors better than BMI. In this study, we evaluated these indices as predictors of operative difficulty.
Patients and Methods
This study included 70 and 44 patients who underwent donor nephrectomy by a transperitoneal approach and retroperitoneal approach, respectively. All surgeries were performed from 2003 to 2010 by two senior urologists specializing in urologic laparoscopic surgeries. The operative procedures and perioperative outcome have been described, previously.6,7 We changed the standard approach from a retroperitoneal approach to a transperitoneal approach in June 2005 because we considered that a transperitoneal approach was technically easier because of the wider working space and the greater number of anatomical landmarks. Since then, we used a retroperitoneal approach only when donors had a history of upper intra-abdominal surgery. In both the transperitoneal approach and the retroperitoneal approach, the dissection of perirenal tissue, renal vessels, and the ureter was performed in a pure laparoscopic manner. At the time of extraction of kidney, the hand-assisted approach was applied to minimize cold ischemic time.
The following indices of obesity were defined in this study. The perirenal fat thickness, which was defined as the distance from the renal capsule to the lateroconal fascia on the line extending to the renal vein, was measured on a CT image at the level of the renal hilum. The subcutaneous fat thickness at the midline of the abdomen was also measured on the same CT image at the same level. In addition, the subcutaneous fat, visceral fat, perirenal fat, and total fat areas were measured on the same slice. These fat areas were measured using the Synapse® Vincent® volume analyzer system (Fujifilm, Tokyo, Japan) (Fig. 1). We defined fat tissue as tissue with a Hounsfield number between −150 and −50. The total, visceral, and perirenal fat areas were measured, and the subcutaneous fat area was calculated by subtracting the visceral fat area from the total fat area. These factors were used to categorize the subjects into the fatty and non-fatty groups with each median value. In addition, donors were divided in the analysis into two groups according to BMI: <25 kg/m2 and ≥25 kg/m2. The operative time and estimated blood loss were compared between the dichotomized groups for each index of obesity.
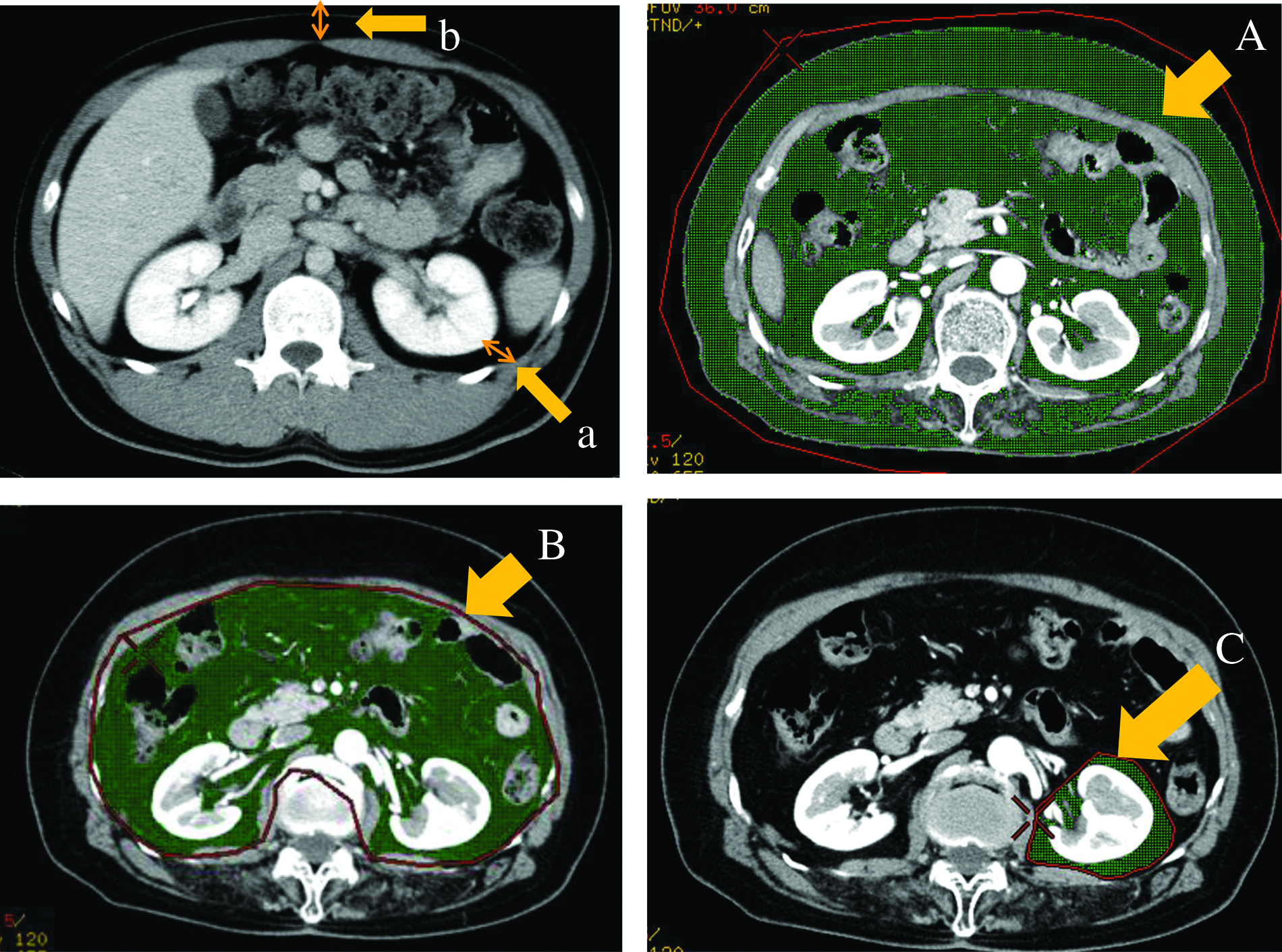
Perirenal fat thickness was defined as the distance (arrow labeled a) from the renal capsule to the lateroconal fascia on the line extending to the renal vein on a computerized tomography image. Subcutaneous fat thickness was measured (arrow labeled b) at the midline of the abdomen on the same computerized tomography image. Total fat (arrow labeled A), visceral fat (arrow labeled B), and perirenal fat (arrow labeled C) areas as shown in green were measured on the same slice as fat thickness was measured. The subcutaneous fat area was calculated by subtracting the area of B from the area of A.
Two-group comparisons were performed by the Mann–Whitney U test, and P values <.05 were considered statistically significant. All the statistical analyses were performed using IBM SPSS® Statistics version 19.0 (IBM Japan, Tokyo).
Written informed consent was obtained from all donors for possible use of the clinical data at admission. This retrospective study was approved by the Ethics Review Board of Akita University Hospital (Akita, Japan).
Results
The characteristics of patients treated with a transperitoneal or retroperitoneal approach are shown in Table 1. The values of perirenal fat thickness, visceral fat area, and perirenal fat area in the transperitoneal approach group were significantly greater than those in the retroperitoneal approach group. Comparisons of operative time and blood loss between fatty and non-fatty donors according to various indices in transperitoneal laparoscopic donor nephrectomy (LDN) are shown in Table 2. The donors in the non-fatty group had a longer operating time than those in the fatty group when the groups were categorized by subcutaneous fat thickness, although this difference was not statistically significant (P=.086) (Table 2). There was no statistically significant difference in the other intraoperative factors between the fatty and non-fatty groups defined by the other index of fat thickness or the four indices of fat (Table 2).
BMI, body mass index; SD, standard deviation.
Comparisons of operative time and blood loss in retroperitoneoscopic donor nephrectomy between fatty and non-fatty donors defined according to the various indices are shown in Table 3. The patients in the fatty group had a longer operating time than those of the non-fatty group when the groups were categorized by BMI, although there was no statistically significant difference between the two groups (P=.053) (Table 3). There was also no statistically significant difference in estimated blood loss between the two groups when the groups were defined by BMI. The patients in the fatty groups categorized by perirenal fat thickness, total fat area, or visceral fat area had significantly greater estimated blood loss than those in the non-fatty group (P=.028, .018, and .001, respectively) (Table 3). Furthermore, patients in the fatty group categorized by perirenal fat area had significantly greater estimated blood loss (P=.02) and longer operating time (P=.014) than those in the non-fatty group. There was no statistically significant difference in any of the other intraoperative factors between the fatty and non-fatty groups when these groups were defined by subcutaneous fat thickness or subcutaneous fat area (Table 3).
Discussion
Obesity has been considered as a risk factor influencing operative difficulty and complications in several urological operations.8–10 Several studies have reported a correlation between operating time or blood loss and BMI in laparoscopic nephrectomy.11–13 Transperitoneal laparoscopic renal surgery for obese patients with a BMI of 30 kg/m2 or greater had longer operative times and increased blood loss compared with the same procedure in non-obese patients. 14 Similarly, laparoscopic nephrectomy for obese donors with a BMI in the range of 35.2–53.9 kg/m2 had a longer operating time than that in non-obese donors with a BMI in the range of 18.4–29.0 kg/m2. 15 Meanwhile, no statistically significant differences were observed in operating time and estimated blood loss in transperitoneal laparoscopic nephrectomy between the obese group with a BMI greater than 30 kg/m2 and the non-obese group. 16 In our study, the values of visceral fat area and perirenal fat area in donors who underwent transperitoneal laparoscopic nephrectomy were significantly greater than those in donors who had undergone retroperitoneoscopic nephrectomy. Although we do not know the reason why such a significant difference was found between the two groups, the decision to use a transperitoneal laparoscopic or retroperitoneal approach was based on the historical background rather than the clinical data or surgeons' preference. Nevertheless, there was no statistically significant difference between any indices and intraoperative factors in transperitoneal laparoscopic nephrectomy.
In a series of retroperitoneoscopic radical nephrectomies in Japanese patients, Inoue et al. 17 reported that a BMI of 25 kg/m2 or greater was a risk factor for longer operating time and greater estimated blood loss than a BMI of less than 25 kg/m2. In our institution, there was no statistically significant difference between the fatty group and non-fatty group dichotomized by BMI of 25 kg/m2 in any of the intraoperative parameters of retroperitoneoscopic donor nephrectomy. Instead, donors in the fatty group categorized by perirenal fat area had significantly greater estimated blood loss and longer operating time than those in the non-fatty group.
Although many reports have addressed the issues regarding the association between obesity and intraoperative factors, the results are still controversial.11–17 One of the reasons for the different results may be the use of the BMI as an index for adult obesity, which does not always reflect body fat mass. Ode et al. 18 reported that there are certain body types, such as patients with increased muscle mass, in whom BMI is poorly predictive of percentage body fat. Furthermore, BMI may not be suitable for Japanese people as an index for evaluating obesity. There are relatively few adult Japanese people who meet the World Health Organization's definition of obesity: BMI greater than 30 kg/m2. In this study, we defined the fatty group as BMI greater than 25 kg/m2 for this reason, and there was no association between BMI and intraoperative factors. Instead of BMI, the fat area indices, especially the perirenal fat area, showed an association with intraoperative factors, suggesting that these indices more adequately predict the surgical difficulty than BMI, at least in Japanese patients.
Many surgeons may have a feeling that the visceral fat, especially perirenal fat, influences operative difficulty in LDN. In support of this view, Anderson et al. 19 reported that a significant positive relationship existed between perirenal fat measurement and operative time in hand-assisted LDN. In this study, however, there was no statistically significant difference between any indices and intraoperative factors in the transperitoneal approach group, whereas patients in the fatty group categorized by perirenal fat area in the retroperitoneal approach group had significantly greater estimated blood loss and longer operating time than those in the non-fatty group. These results suggested that perirenal fat influenced the operative difficulty in the retroperitoneal approach but not in the transperitoneal approach. This may have been because fat constricted the working space and disturbed the visualization or dissection of renal vessels in the retroperitoneal approach. In donors with a high volume of perirenal fat, therefore, a transperitoneal approach may be preferable for LDN.
Conclusions
The results indicate that the visceral fat, especially perirenal fat measured using CT images, influences the operating time and estimated blood loss when using a retroperitoneal approach but not when using a transperitoneal approach for donor nephrectomy. In donors with a high volume of perirenal fat, a transperitoneal approach may be preferable for LDN.
Footnotes
Disclosure Statement
No competing financial interests exist.