
Abstract
Abstract
Objective:
To compare transperitoneal and retroperitoneal approaches of laparoscopic pyeloplasty (LP) for ureteropelvic junction obstruction (UPJO) with meta-analysis.
Materials and Methods:
All randomized controlled trials (RCTs) and controlled clinical trials (CCTs) comparing transperitoneal LP (TLP) and retroperitoneal LP (RLP) were included systematically using Medline, Embase, and The Cochrane Library. Outcomes were success rate, complications, operative time, conversion, presence of a crossing vessel, and length of hospital stay. Two reviewers independently extracted data and assessed quality. Meta-analysis used both fixed and random effects models with dichotomous data reported as relative risk and continuous data as a weighted mean difference with 95% confidence intervals.
Results:
One RCT and eight CCTs were identified (reporting 776 participants). Meta-analysis showed that TLP was associated with an operative time reduction of about 40 minutes (weighted mean difference −43.85, 95% confidence interval −58.06 to −27.63; P<.00001) and significantly lower conversion rate (relative risk [RR] 0.39, 95% confidence interval 0.21–0.74; P=.004) compared with RLP. The two approaches were similar in terms of presence of a crossing vessel (RR 1.24, 95% confidence interval 0.83–1.86; P=.28), length of hospital stay (weighted mean difference −0.24, 95% confidence interval −0.75 to 0.26; P=.35), success rate (RR 1.03, 95% confidence interval 0.97–1.09; P=.76), and complications (RR 0.83, 95% confidence interval 0.17–1.26; P=.61).
Conclusions:
LP as a minimally invasive treatment for UPJO can be performed through both the transperitoneal and retroperitoneal approaches, and either approach is associated with a high success rate and a low complication rate, although TLP provides a shorter operative time and lower conversion rate.
Introduction
LP can be performed via a transperitoneal or retroperitoneal approach based on the surgeon's preference and experience. Other factors such as previous surgery, laparotomy, morbid obesity, and the crossing vessels can also affect the choice. 2 The main advantages of the retroperitoneal approach are as follows: no colonic reflection and low risk of injury to intraperitoneal organs or later development of intraperitoneal adhesions, no risk of spillage of infected urine intraperitoneally, and also familiar anatomy to urologists with direct access to the UPJ. 3 However, the unique anatomic orientation, more delicate maneuvering, and a relatively restricted working space are the limitations. In addition, the transperitoneal approach is the first laparoscopic route for most surgeons that they have learned, so the familiarity of the process makes it easier to learn. As a result, which approach is better—transperitoneal or retroperitoneal—remains unclear. To our knowledge, there are only a few studies with controversial results comparing the two LP approaches, and so far there has been no meta-analysis about this issue.
Materials and Methods
Search strategy
The relevant trials that compared transperiteonal LP (TLP) with retroperitoneal LP (RLP) for UPJO were obtained from the electronic databases Medline, Embase, and The Cochrane Library, reference lists of urology textbooks and review articles, and abstracts of conference proceedings. All the potential articles were required to include the following terms in their titles, abstracts, or key word lists: “transperitoneal,” “retroperitoneal,” “laparoscopic pyeloplasty,” or “ureteropelvic junction obstruction” (or UPJO).
Data extraction and quality assessment
Two reviewers (Y.J.W. and Q.D.) independently extracted data and assessed study quality using the checklist developed for the Cochrane renal group. 4 Discrepancies were resolved by discussion and arbitration by a third party if necessary. The following variables were recorded: authors, year of publication, geographical region, number of patients, operative time, presence of a crossing vessel, length of hospital stay, days of convalescence, conversion, success rate, and complications related to the surgeries (such as urine leak on removal of the catheter, persistent leakage from the drain site, acute urinary retention, deep venous thrombosis, and postoperative ileus). When important data were not reported, we tried to contact the authors.
The reviewers assessed types of studies, concealment of allocation, completeness of follow-up and blinding of investigators, participants, and outcome assessors. They screened identified titles and abstracts independently. Potentially relevant trials were retained, and the full text was examined.
Data analysis
A formal meta-analysis was made of all trials comparing the efficacy and safety of TLP and RLP. Relative risk (RR) values were calculated for dichotomous data, and weighted mean difference values were calculated for continuous data, with 95% confidence intervals. Pooled estimates of efficacy were calculated using a fixed-effects model (Mantel–Haenszel), but a randomized-effects model (DerSimonian and Laird) was used according to heterogeneity. Statistical heterogeneity of treatment effects between studies was formally tested with Cochran's test for heterogeneity (P<.1). The I2 statistic was also examined. We explored possible sources of heterogeneity (participants, treatment, study quality). In addition, sensitivity analysis was applied by removing individual studies from the dataset and analyzing the effect on the overall results. All meta-analyses were performed using RevMan software (version 5.1; Cochrane IMS).
Results
Of 62 potentially relevant studies, 52 studies were excluded after their abstracts were reviewed (15 studies were reviews, 25 studies were not controlled trials, and 12 studies did not compare TLP with RLP). Ten articles were retrieved for more detailed evaluation, but one was excluded that assessed the differences between various techniques of laparoscopic LP, 5 leaving nine trials for reviewing.
Study characteristics
The nine trials were conducted in seven countries, reported on 776 participants, and were published in 2003–2011 (Table 1).
DJ stent, double J stent; IVU, intravenous urography; NA, not available (insufficient information provided); 99Tc-DTPA, technetium-99 diethylenetriamine-pentaacetic acid; UPJ, ureteropelvic junction.
Baseline characteristics about age and sex of patients were reported in all the included trials. Three trials2,7,9 compared the differences between TLP and RLP groups and found no statistical significance. All except one 9 of the included trials reported the operative sides, presence of a crossing vessel, and that of renal stone. Two trials2,7 found them not significantly different. All the patients were assessed preoperatively by routine laboratory investigations, ultrasound, intravenous urography, and diuretic renogram. Renal function (serum creatinine, split renal function), radiographic results, and symptoms were assessed to judge the success rate. The success was defined as shown in Table 1.
Because a randomized controlled trial (RCT) was very rare on this topic, we included eight controlled clinical trials (CCTs) in the meta-analysis. Accordingly, the main limitations were obvious in the study design, which pertained to no randomization and the procedure for concealing the treatment allocation, although some trials reported that the participants were allocated in the order of medical visit or admission to the hospital. Only the RCT 2 stated that the randomization was performed by closed envelopes. In addition, outcome measures, such as operative time and length of hospital stay, varied. Not all the nine included studies presented outcomes as a mean (standard deviation) value, which was considered a minimum requirement for any meta-analysis, and this limited the analysis of these outcomes to trials providing complete information. The trials' designs were heterogeneous with regard to LP techniques, double J stent placement approaches, outcome assessment, and study designs.
Perioperative outcomes
Table 2 summarizes the results of meta-analysis of perioperative outcomes. The statistically significant differences in pooled estimates suggest a benefit of TLP over RLP for operative time and conversion rate, and no statistically significant differences were noted between TLP and RLP for length of hospital stay, presence of a crossing vessel, and complications. There was significant heterogeneity for hospital stay (I2=64%). Sensitivity analysis showed that the significant heterogeneity could be attributed mainly to the trial reported by Canon et al. 9
RLP, retroperitoneal laparoscopic pyeloplasty; TLP, transperitoneal laparoscopic pyeloplasty.
Efficacy outcome (success rate)
Of the nine trials, eight2,6–10,12,13 reported on the success rate of the procedure. Subgroup analysis was done by classifying the studies by study type (RCT and CCT). Pooled analysis showed no differences between the two approaches of LP either in subgroups (RR 1.03, 95% confidence interval 0.97–1.09) or in total effect (RR 1.03, 95% confidence interval 0.97–1.09) (Fig. 1).
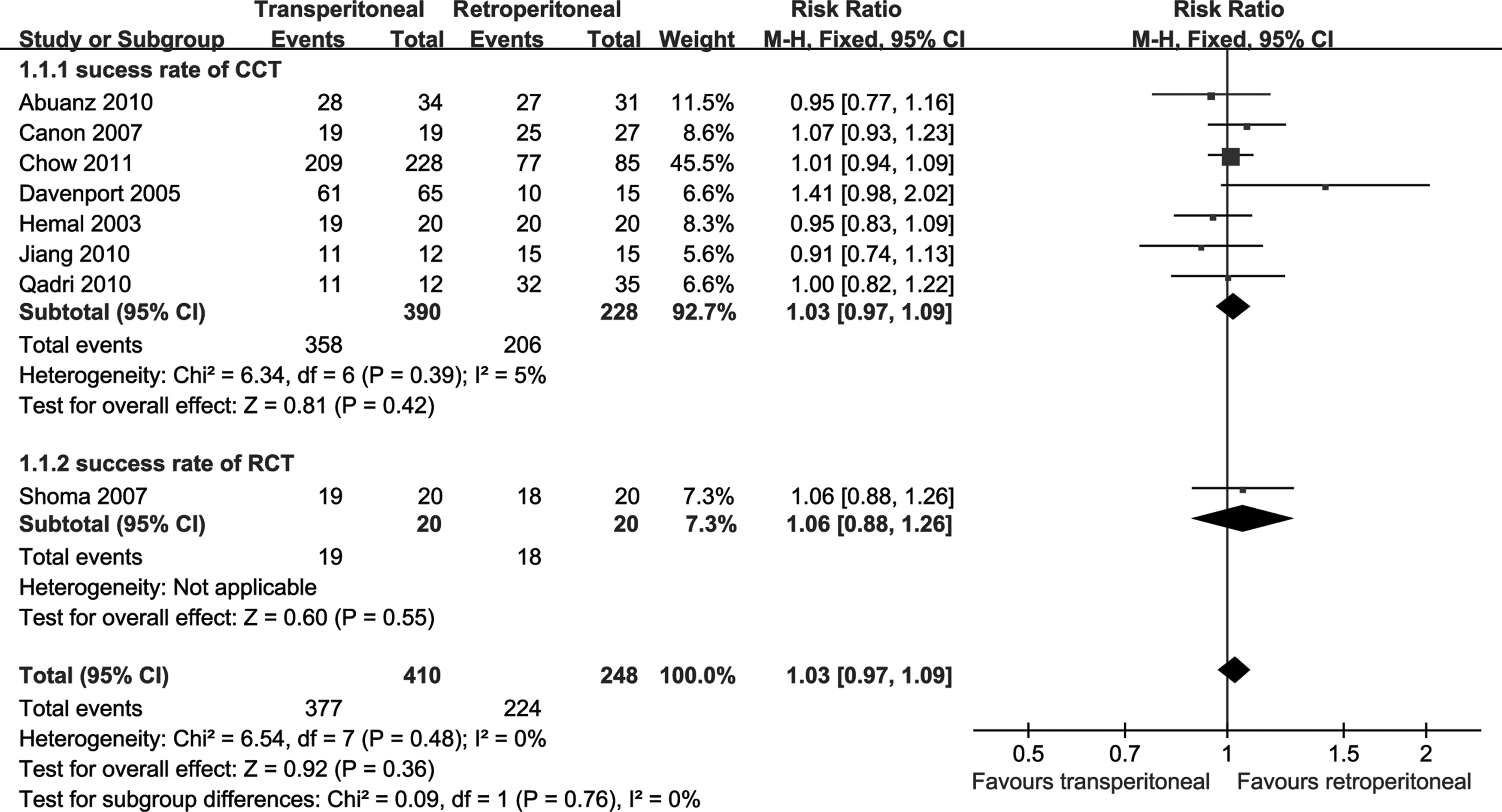
Meta-analysis of success rate between retroperitoneal laparoscopic pyeloplasty and transperitoneal laparoscopic pyeloplasty (all available data). The lower and upper confidence interval (CI) values refer to 95% CIs. CCT, controlled clinical trial; M-H, Mantel–Haenszel; RCT, randomized controlled trial.
Discussion
In this systematic review we found that RLP was as effective as TLP in management of UPJO. We evaluated the benefits, harms, and costs of the two approaches of LP. TLP was associated with an operative time reduction of 40 minutes and significantly lower conversion rate compared with RLP. No differences between the approaches with regard to length of hospital stay, intraoperative presence of a crossing vessel, and the rate of success and complications. The clinical implications of these findings need further research as the present level of evidence is based on trials with marked methodological and clinical heterogeneity because of the inclusion of non-RCTs and different LP techniques, double J stent placement approaches, and outcome assessment.
The mean operative time was longer for RLP. There are probably two reasons. First, the effect of the relatively narrow working space may lead to prolongation of the operative time required for intracorporeal suturing, especially with the early experience with laparoscopic repair of UPJO. Second, the lack of retroperitoneoscopic experiences and the unique anatomic orientation also contributed to the long duration of operation. However, with the experiences of retroperitoneoscopy increasing, a significant decrease in operative time can be achieved. It has been estimated that trainees must perform approximately 40 cases before they can consistently produce good outcomes. 9 In the same way, this is possibly not much different from the initial learning curve for conventional LP.
This pooled analysis of literature has also shown that RLP presented a higher conversion rate. The main causes for converting to open surgery in the articles analyzed were as follows: inflammation and adhesion around the ureter, tension at the anastomosis, massive hydronephrosis with limited working space, and some other reasons such as portal hypertension, perineal fibrosis, and achondroplasia. Similarly, the higher conversion rate of RLP was probably relevant to the inability of managing the complicated situation under the unfamiliar retroperitoneoscopic space during the procedure.
No difference was found between the two approaches in length of hospital stay, presence of a crossing vessel, rates of success, and complications. The outcomes of rates of success and complications were similar to those of other analyses of surgical intervention for UPJO.14,15 However, the outcomes of length of hospital stay and presence of a crossing vessel were not reported consistently across the studies. None of the trials reported on health-related quality of life. One trial reported on cost implications, but no results about comparing the two approaches were obtained. 8
Some limitations of this review should be noted. First, because of a lack of standard definition of “success,” the decision on whether a LP is a success can be difficult to make. The definition of success varied across the included studies. Most studies defined success of a procedure as improvement in radiographic findings (stable or less hydronephrosis, patent UPJ, and nonobstructed diuretic renal scan with improved or stable split renographic clearance). However, some studies did not give the definition that brought assessment bias.8,12,13 Second, there was a lack of standardization of trials' performance. To achieve a fairer comparison between the two approaches, both procedures should be performed by the same surgeon. Although our analysis showed that the operative time for TLP was significantly shorter by 43.85 minutes, there were only two trials reporting that both TLP and RLP were performed by the same experienced surgeons with the same team (Shoma et al. 2 and Qadri and Khan 10 ), which would bias the results in favor of TLP and reduce external validity. In addition, dismembered pyeloplasty was performed by most trials, but the other pyeloplasty techniques were still used in three trials.8,11,12 Besides, the variable number of ports and the approach of double J stent placement would produce a performance bias. Third, there was a lack of standardization of outcome measures. The length of follow-up varied across the studies. The longest follow-up was up to 18–72 months, but the shortest one was only 7.1–7.9 months. Some trials had incomplete follow-up 9 and missing information, 12 leading to potential reporting bias. Finally, because some non-RCTs were included, selective bias and systematic bias were unavoidable.
Conclusions
As the trend toward minimally invasive surgery continues, it is necessary to consider the potential benefits of TLP and RLP for all urologists. This meta-analysis suggests that there was no difference between the transperitoneal and retroperitoneal approaches of LP, especially in terms of success rate. The data reveal that LP as a minimally invasive treatment for UPJO can be performed through either the transperitoneal or retroperitoneal approach, and either approach is associated with a high success rate and a low complication rate. As a result, it is hard to tell which is better. The ultimate decision should be up to the surgeon's preference and experience. Because the results and recommendations may be potentially flawed by the clinical and methodological heterogeneity, more high-quality, rigorous randomized trials are needed to examine the effect of the two approaches in management of UPJO and to make significantly clinical recommendations.
Footnotes
Disclosure Statement
No competing financial interests exist.