
Abstract
Abstract
Introduction:
The indication and anatomic limits of pelvic lymph node dissection (PLND) have not been clearly defined. Therefore, we assessed whether the extent of PLND at robot-assisted laparoscopic radical prostatectomy (RALP) had any benefit on lymph node yield, staging accuracy, and biochemical recurrence (BCR) in patients with high-risk prostate cancer.
Patients and Methods:
Between July 2005 and July 2010, a retrospective analysis was performed on 200 patients with high-risk prostate cancer stratified by D'Amico classification. The study population was divided into different groups: patients in Group 1 had standard PLND, and Group 2 had extended PLND (ePLND). The clinicopathologic findings of patients and surgical outcomes of PLND with each procedure were measured. Kaplan–Meier and log rank tests were used to estimate BCR-free survival rates. Univariate and multivariate survival analyses were done with the Cox proportional hazard regression model.
Results:
Medians of 15 (interquartile range, 11–19) and 24 (interquartile range, 18–28) lymph nodes were dissected in Groups 1 and 2, respectively (P<.001). The incidences of lymph node metastasis were 5.2% (8/155) in Group 1 and 22.2% (10/45) in Group 2. Regardless of the extent of PLND, the patients with positive lymph nodes had a significantly lower BCR-free survival than those with negative lymph nodes. Twenty-five percent (7/27) of positive lymph nodes were in the internal iliac packet and common iliac packet. In particular, of the positive internal iliac nodes, 75% (3/4) of nodes were found in that location, exclusively.
Conclusions:
An ePLND that identifies patients with lymph node metastasis including the internal iliac packet during RALP provides an accurate pathologic staging and may have survival benefits in high-risk prostate cancer.
Introduction
Currently, a minimally invasive surgical approach such as robot-assisted laparoscopic radical prostatectomy (RALP) is being increasingly used as the standard treatment modality for prostate cancer. Even on high-risk prostate cancer, oncologic outcomes of RALP have been shown to be comparable to those of open radical prostatectomy.11–13 Moreover, recent reports have demonstrated that PLND during RALP provided a high lymph node yield and appeared to have minimal morbidity compared with the open technique.13–15
Therefore, we assessed whether the extent of PLND at RALP had any benefit on lymph node yield, staging accuracy, and biochemical recurrence (BCR) in patients with high-risk prostate cancer.
Patients and Methods
Between July 2005 and July 2010, 829 consecutive men underwent transperitoneal RALP with PLND using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) by a single surgeon (K.H.R.). There were 297 (35.8%) patients with high-risk prostate cancer stratified by the D'Amico classification. 16 Patients who had received neoadjuvant hormonal therapy or neoadjuvant radiation or had missing follow-up data were excluded. The remaining 200 patients were analyzed, retrospectively. The comprehensive database was approved by the Institutional Review Board (protocol number 4-2009-0131).
In order to evaluate outcomes of PLND, the study population was divided into different groups: patients in Group 1 had standard PLND (sPLND), and Group 2 had extended PLND (ePLND). Patients' characteristics (age, body mass index, prostate volume assessed by transrectal ultrasound, and adjuvant therapy), tumor characteristics (preoperative prostate-specific antigen [PSA], Gleason score, T stage, and lymph node metastasis), and surgical data (operation time, PLND time, intraoperative blood loss, resection margin, number of lymph nodes, and complications) were evaluated. The 2002 American Joint Committee on Cancer/TNM staging system and Gleason system were used for the pathologic staging and tumor grading. 17
Our standard technique of RALP was described previously by Park et al. 18 In our institute, robot-assisted ePLND has been performed in patients with high-risk prostate cancer since July 2008. The template of sPLND, as previously described by Walsh, consisted of obturator and external iliac nodal packets. 19 The template of ePLND encompassed additional tissue on the medial and lateral aspect of the internal iliac vessels as well as along common iliac vessels up to the ureteric crossing, as previously described by Thurairaja et al. 20
All patients underwent meticulous PLND before dissection of the prostate. 21 The ePLND was initiated by carefully incising peritoneum over the perceived area of the common iliac bifurcation that was guided by the ureters. The dissection proceeded distally on the proximal common iliac artery to the common iliac bifurcation. Nodal tissue around the bifurcation was harvested free. Next, lympadenectomy was performed along the medial aspect of the ureter while following the internal iliac artery to the level of the obligated umbilical artery. The lymphatic tissue around internal iliac vessels was submitted as the internal iliac specimen. Lymph node dissection was done along the external iliac artery from its origin down to the circumflex iliac vessels. The node of Cloquet distally and surrounding tissue were retrieved and sent separately. Then, all lymphofatty tissues surrounding the obturator fossa along the obturator muscle were removed, preserving the obturator nerve and vessels. Preprostatic fat was also removed until the endopelvic fascia was identified. In total, 11 packets per patient were labeled as common iliac, internal iliac, external iliac, obturator, inguinal node (node of Cloquet), and preprostatic fat pad. Specimens from different locations on each side were individually removed through an assistant port and sent for pathologic analysis in a grid-like specimen container. Endo bags were not used for lymph node extraction because the 12-mm assistant port would allow packet passage. Lymphatic channels were sealed by using clips and fibrin sealant agents to reduce the risk of lymphocele. Frozen section analyses were not routinely obtained.
The PLND-related postoperative complications were defined as neurovascular injuries, ureteral injuries, clinically significant lymphoceles, and thromboembolic sequelae requiring hospitalization and intervention. 22 After RALP, serum PSA measurement was performed every 3 months for the first year and semiannually thereafter. BCR was defined as a PSA level>0.2 ng/mL on two consecutive measurements.
The independent t test, Mann–Whitney test, Fisher's exact test, and chi squared test were used to compare the clinicopathologic characteristics between the two groups of patients. Kaplan–Meier and log rank tests were used to estimate BCR-free survival rates. Univariate and multivariate survival analyses were done with the Cox proportional hazard regression model. All analyses were performed with SPSS version 13.0 software for Windows (SPSS, Chicago, IL), and a two-tailed P value of<.05 was considered statistically significant.
Results
Table 1 summarizes the clinical characteristics and surgical results of patients treated with RALP and PLND. There were no significant differences in age, body mass index, prostate volume, adjuvant therapy, and clinical and pathologic T stage between the two groups. Preoperative PSA, Gleason score on needle biopsy, and surgical specimen in Group 2 were significantly higher than those of Group 1 (P=.001, .003, and .001, respectively). The median operation time including PLND was 190 (interquartile range [IQR], 165–211) and 196 (IQR, 180–224) minutes, respectively (P=.027). Duration of PLND was also significantly longer in Group 2 (P<.001). Blood loss and hospital stay were similar in the two groups. A total of six complications that were related to PLND occurred after surgery. There were no significant differences in complications between the two groups. No vascular injuries, thrombotic events, urine leaks, or deaths were seen. Medians of 15 (IQR, 11–19) and 24 (IQR, 18–28) lymph nodes were removed in Group 1 and Group 2, respectively (P<.001). The incidence of lymph node metastasis was 5.2% (8/155) in Group 1 and 22.2% (10/45) in Group 2.
P<.05 was defined as a significant difference.
BMI, body mass index; IQR, interquartile range; OP, operation; PLND, pelvic lymph node dissection; PSA, prostate-specific antigen.
Median follow-up was 24 (IQR, 15–34) and 13 (IQR 10–17) months in Groups 1 and 2, respectively. Overall BCR-free survival is shown in Figure 1A. Thirty-four patients (22.1%) in Group 1 and 16 (35.6%) in Group 2 had BCR. Regardless of the extent of PLND, the patients with positive lymph nodes had a significantly lower BCR-free survival than those with negative lymph nodes (Fig. 1B and C).
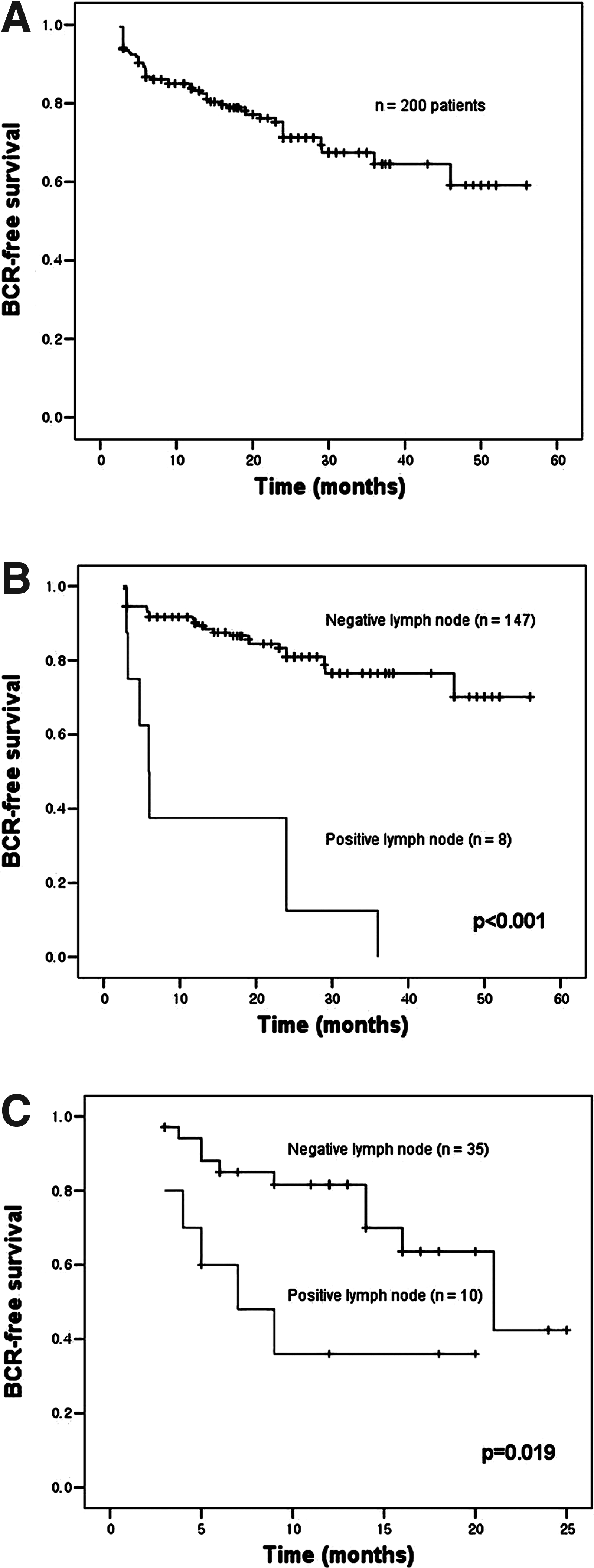
Biochemical recurrence (BCR)-free survival stratified by extent of pelvic lymph node dissection.
Table 2 shows univariate and multivariate analysis of association of clinicopathologic variables with BCR. All parameters were statistically significant predictors of BCR on univariate analysis. However, on multivariate analysis, pathologic Gleason score, pathologic T stage, and lymph node metastasis were identified as significant predictors of BCR.
P<.05 was defined as a significant difference.
CI, confidence interval; GS, Gleason score; HR, hazard ratio; PSA, prostate-specific antigen.
Table 3 shows the distribution of positive lymph nodes in Group 2. Twenty-five percent (7/27) of positive lymph nodes were in the internal iliac packet and common iliac packet. In particular, of the positive internal iliac nodes, 75% (3/4) nodes were found in that location, exclusively. In addition, 60% (6/10) patients who were found to have positive lymph nodes had lymph node metastasis outside of the templates of sPLND. There was no positive lymph node in the specimen of the node of Cloquet and preprostatic fat pad.
One exclusively in this location.
Three exclusively in this location.
Six ePLND-related complications were recorded for the patient population, with 4 (66%) Clavien Grade 1. Two lymphocele (Grade 3a) cases and three lower extremity edema (Grade 1) cases occurred in Group 1, and one lymphocele (Grade 1) occurred in Group 2. Two patients with symptomatic lymphocele in Group 2 underwent percutaneous drainage with the assistance of an interventional radiologist. Intraoperative vascular, neural, and ureteral injuries during PLND did not occur.
Discussion
The usage of PLND has declined because of the advent of PSA screening and the development of nomograms to predict lymph node status. 13 From 1992 to 2004, analysis of a community-based cohort showed that PLND had decreased from 94% to 80%. 23 However, there is no doubt that PLND during radical prostatectomy improves the accuracy of cancer staging, as conventional imaging techniques have proven to be insufficient. Accurate cancer staging helps to identify patients who need further adjuvant treatment and provide accurate prognosis after surgery.1,2,20,21 Therefore, our unit routinely has performed PLND during RALP, both standard and extended, in all patient. In particular, in high-risk prostate cancer, we postulate that PLND has significant diagnostic and therapeutic roles.
The varying extent of PLND for prostate cancer has been described. This includes minimal template with obturator fossa only, limited/standard template consisting of obturator and external iliac fossae, and extended template with dissection of the obturator fossa and external and internal iliac vessels, as well as the common iliac vessels up to the ureteric crossing.3,21 However, the prostate lymphatics were made up of three groups of the periprostatic subcapsular networks (ascending duct from the cranial prostate draining into the external iliac lymph nodes, lateral duct to the internal iliac lymph nodes, and the posterior duct from the caudal prostate to the subaortic sacral lymph nodes of the promontory).6,7 Hence, sPLND may miss positive lymph nodes. In addition, crossover of lymphatics is common, and no single sentinel node has been identified.7,13 Recently, Heidenreich et al. 6 found that 26% of patients had positive lymph nodes even on clinically localized prostate cancer. Moreover, Schumacher et al. 24 reported that positive lymph nodes were found in 11% of ePLND even in patients with a serum PSA of <10 ng/mL. In the present study, we performed ePLND depending on preoperative stratification according to preoperative PSA, Gleason score, and clinical stage. Retrieved lymph nodes and incidence of metastasis were significantly higher in patients who underwent ePLND. In 60% of patients who underwent ePLND and who had lymph node metastasis, positive lymph nodes were found in the extended regions. Fifteen percent of the positive nodes were found in the internal iliac packet. In particular, of internal iliac nodal involvement, 75% (3/4) nodes were found in that location, exclusively. This suggests that the current sPLND template of dissecting the obturator and external iliac nodes only is insufficient for high-risk prostate cancer. As a result, internal iliac lymph nodes as primary lymphatics of the prostate should be removed in patients with high-risk prostate cancer. Additionally, autopsy data from Weingärtner et al. 25 showed that 20 lymph nodes need to be removed for an adequate lymph node dissection. In our study, a mean of 24 lymph nodes was removed in the ePLND group compared with 15 lymph nodes in the sPLND group.
The survival benefits of PLND also have been debated. Bhatta-Dhar et al. 26 demonstrated that PLND did not affect BCR rates at 6 years after surgery. However, Bader et al., 9 who reported lymph node metastases in 25% of patients with organ-confined prostate cancer, showed that BCR was significantly associated with the number of diseased nodes. They concluded that PLND was not only a staging procedure, but might also have a positive impact on BCR and disease-free survival. On our multivariate analysis, lymph node metastasis was found as a significant predictor of BCR. Furthermore, all patients with positive lymph nodes in the sPLND group had BCR, and 60% (6/10) patients with positive lymph nodes in the ePLND group had BCR. In addition, Briganti et al. 27 demonstrated that the extent of PLND was related to the probability of lymph node metastasis. They designed a nomogram based on clinical stage, PSA, biopsy Gleason score, and the number of total lymph nodes removed. In the review of the Surveillance Epidermiology and End Results database, more extensive PLND improved disease-specific survival even in patients with negative nodes. 10 These results suggest ePLND, which identifies patients with lymph node metastasis more frequently, might have survival benefits.
Performing PLND at RALP, we bear in mind to balance the effectiveness of the procedure with the complications of PLND. PLND has potential complications and morbidities, with an overall reported rate of complication from 4% to 50%.1–3,22 In randomized prospective evaluation of the extent of PLND, Clark et al. 28 reported an overall complication rate of 10.7%, with 75% of unilateral complication occurring on the side where ePLND was performed. However, in the present study, PLND-related complications, including lymphocele, were also not significantly different between sPLND (3.1%) and ePLND (2.2%). In addition, intraoperative vascular, neural, and ureteral injuries during PLND were not seen. Musch et al. 22 showed that intraoperative injuries to the ureter and obturator nerve were significantly associated with PSA levels, not extent of PLND; they also noted one injury of an obturator artery in the series of 1380 patients. Although they concluded that lymphocele formation was associated with extent of PLND, recent studies for robotic ePLND noted a low incidence of lymphocele (0%–3%).13,29 The authors believe that the results may be partially attributable to ePLND sequentially following sPLND and the transperitoneal approach.
This study was limited by the nonrandomized, retrospective design, in addition to short-term follow-up data because of the brief history of RALP. Therefore, this study did not have an association of extent of PLND and cancer-specific survival and overall survival rate. Nevertheless, we believe that this report is worthwhile to describe operative outcomes of robot-assisted PLND in high-risk prostate cancer.
In conclusion, ePLND, which provides a high lymph node yield, identifies a greater proportion of lymph node metastasis in patients with high-risk prostate cancer undergoing RALP. PLND-related complications were not significantly different between sPLND and ePLND. Collectively, ePLND, which identifies patients with lymph node metastasis including the internal iliac packet during RALP, provides an accurate pathologic staging and may have survival benefits in high-risk prostate cancer. To properly evaluate the impact of ePLND on the outcomes of high-risk prostate cancer, a prospective randomized trial and long term follow-up are needed.
Footnotes
Acknowledgments
We are grateful to Hyun Jin Jung for her assistance in the preparation of this article.
Disclosure Statement
No competing financial interests exist.