
Abstract
Abstract
Background/Purpose:
Single-incision laparoscopic surgery aims to minimize surgical trauma. Yet there has been no report on its application to the treatment of correctable biliary atresia (BA). We present here our initial mini-series of successful single-incision laparoscopic hepaticojejunostomy (SILH) for correctable BA.
Patients and Methods:
We reviewed 4 correctable BA patients (Type I/II, 3/1) who underwent SILH between May and July 2011. Ultrasonography, upper gastrointestinal contrast studies, and blood tests were performed during the follow-up period. The age at operation, operative time, postoperative hospital stay, resumption of full diet, postoperative complications, and perioperative laboratory tests were evaluated.
Results:
The median age at operation was 21 days. The median operative time was 2 hours. Blood loss was minimal. The median follow-up duration was 4.5 months. Jaundice gradually declined after 3–5 days in Type I and 6 days in Type II BA patient. There was no mortality or surgical complication so far.
Conclusions
Introduction
Patients and Methods
Three neonates with Type I BA and one with Type II BA who underwent SILH between May and July 2011 were reviewed. The procedures were carried out by a single surgical team. Ethics approval from the Ethics Committee of the Capital Institute of Pediatrics (Beijing, China) was obtained. Written informed consents were obtained from the parents of the BA neonates before operation.
One male and three female neonates with persistent jaundice after birth were referred to our department. Hilar cysts were detected by prenatal ultrasound studies in 2 patients and by postnatal ultrasonographic studies in the remaining 2 patients. The blood test results showed significantly deranged liver function: Type I, alanine aminotransferase (ALT) of 254.2–275.0 U/L, aspartate aminotransferase (AST) of 262.1–274.0 U/L, gamma-glutamyltransferase (GGT) of 1054–1285 U/L, alkaline phosphatase (ALP) of 320.8–922 U/L, total bilirubin of 181.9–217.7 μmol/L, and direct bilirubin of 128.2–157.4 μmol/L; Type II, ALT of 316.0 U/L, AST of 333.0 U/L, GGT of 3280 U/L, ALP of 1200 U/L, total bilirubin of 249.0 μmol/L, and direct bilirubin of 186.6 μmol/L.
The patient was placed in the supine anti-Trendelenburg position. The surgeon stood on the feet end of the patient, the assistant with the camera on the patient's left side, and the instrument nurse on the patient's right side (Fig. 1).
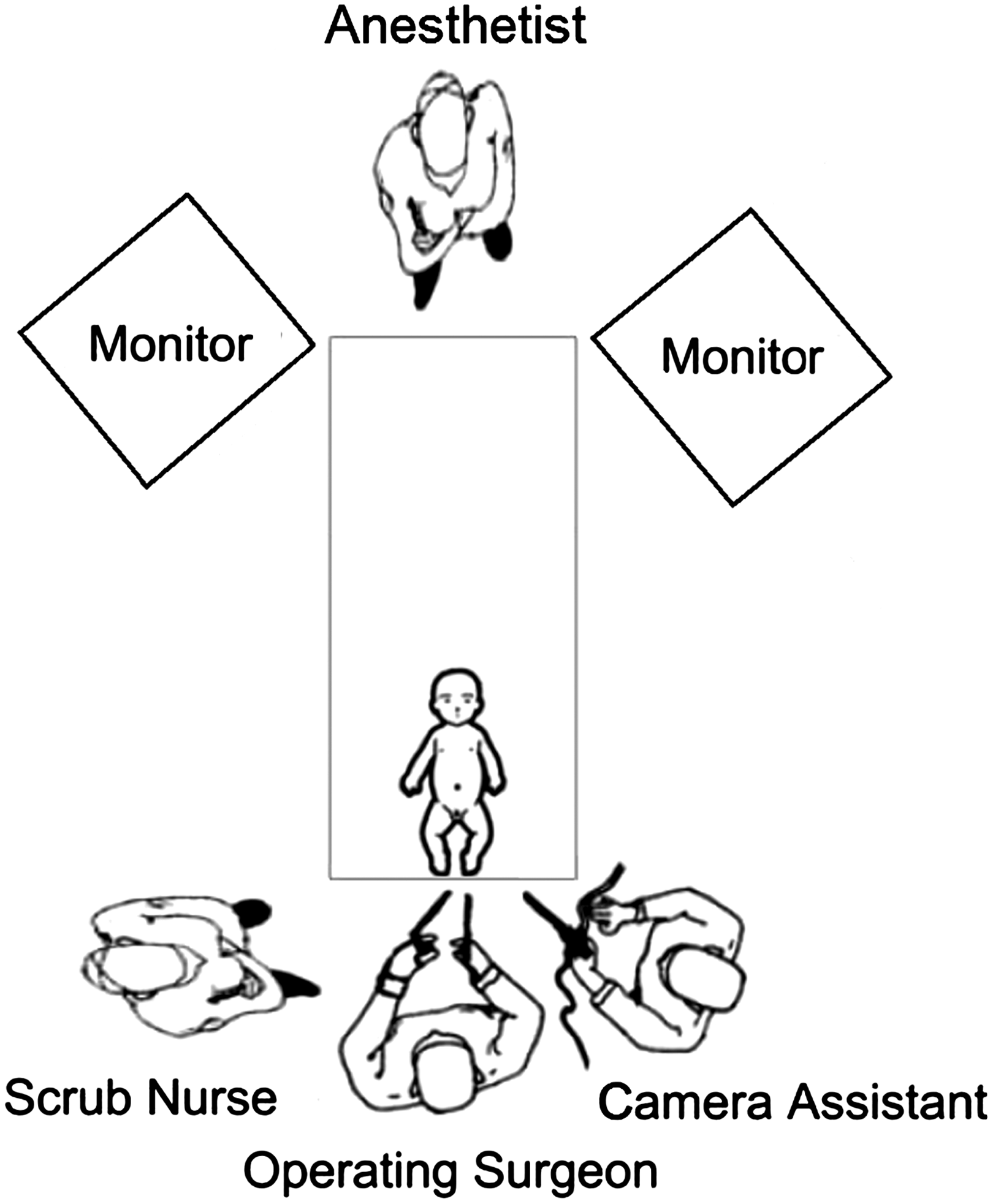
Set-up of the operating room for single-incision laparoscopic hepaticojejunostomy for neonates with correctable biliary atresia.
A vertical umbilical incision was made. An extralong 5-mm 30° laparoscope (model 26046BA, Karl Storz GmbH & Co. KG, Tuttlingen, Germany) was inserted through the camera port, which was placed in the midline fascial incisions. Carbon dioxide pneumoperitoneum was established with the pressure at 6–8 mm Hg. Two 3-mm conventional laparoscopic instruments were inserted through working ports, which were placed lateral to the camera port on either side, at the horizontal ends of the umbilical incision (Fig. 2).

Transumbilical single-incision with three ports and two transcutaneous suture retractions in a female neonate with Type I biliary atresia.
Under laparoscope guidance, intraoperative cholangiograms were performed with a 20-gauge transcutaneous angiocatheter puncturing through the gallbladder fundus. Intraoperative cholangiograms of the 3 female neonates showed atresia of the common bile duct with cystic dilatation proximal to the atresia, indicating Type I BA according to the Japanese BA classification system 5 (Fig. 3a–c). The intraoperative cholangiogram in the one male neonate showed atresia of the common hepatic duct with cystic bile ducts found at the porta hepatis, suggesting Type II BA (Fig. 3d). 5
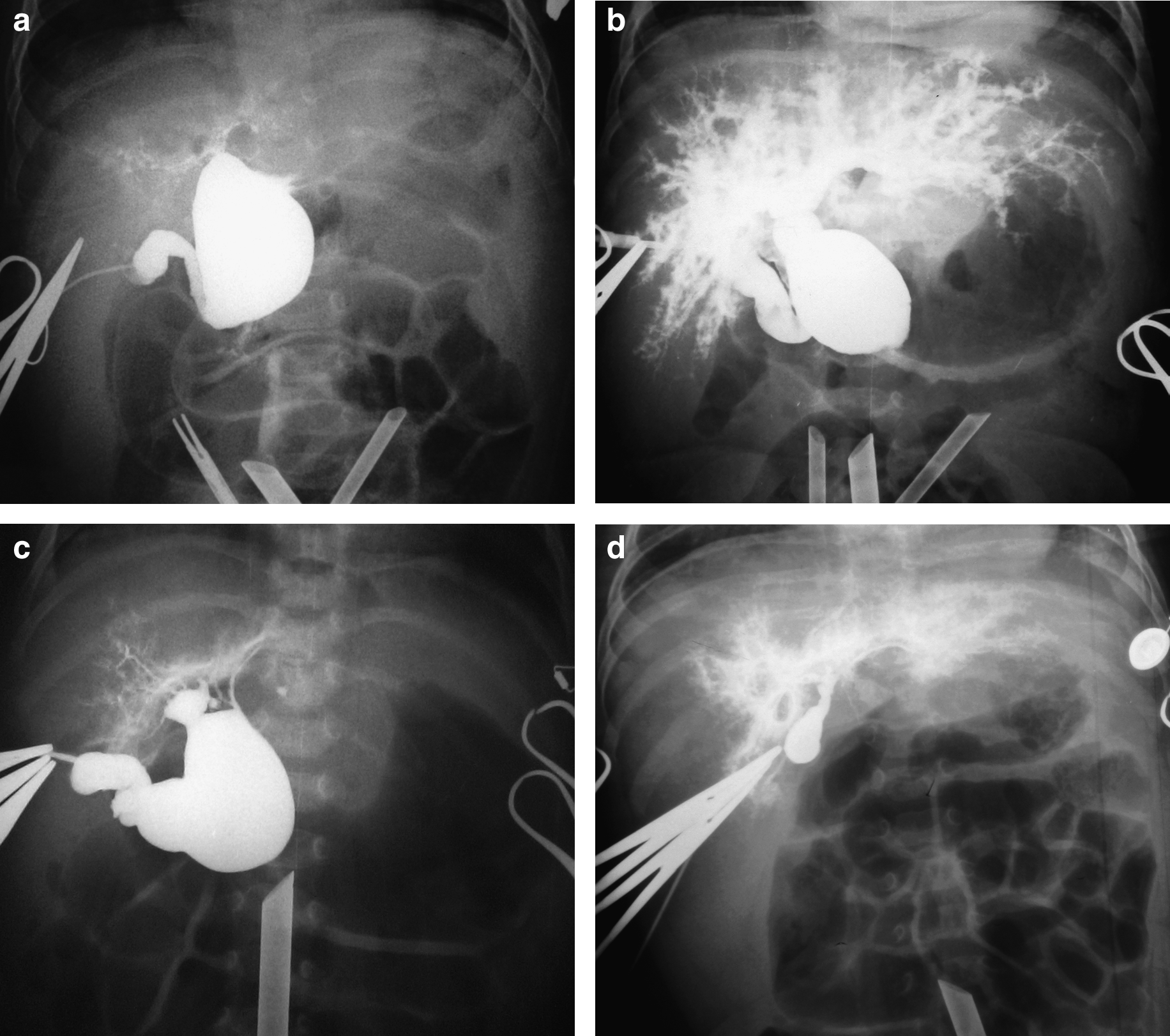
Intraoperative cholangiograms confirmed correctable biliary atresia:
To achieve adequate exposure of hepatic hilum and facilitate dissection and anastomosis, two or three traction hitch stitches were routinely passed through the anterior abdominal wall and (1) the gallbladder fundus, (2) fibrous tissue of the hepatic hilum, and (3) the midportion of the anterior wall of cystic dilatation (for patients with larger cysts) (Fig. 2).
The blind-ends of the bile duct cysts were dissected out and incised at the distal ends (Fig. 4a and b). Significant and continuous bile drainages were found in all patients (Fig. 4c). After bile aspiration, the cyst was resected. The resection was performed as high as possible to improve long-term bile flow (Fig. 4c). The gallbladder was then dissected off the liver bed using a 3-mm hook cautery. The suture through the serosa of gallbladder was left behind for liver retraction during the hepaticojejunal anastomosis.
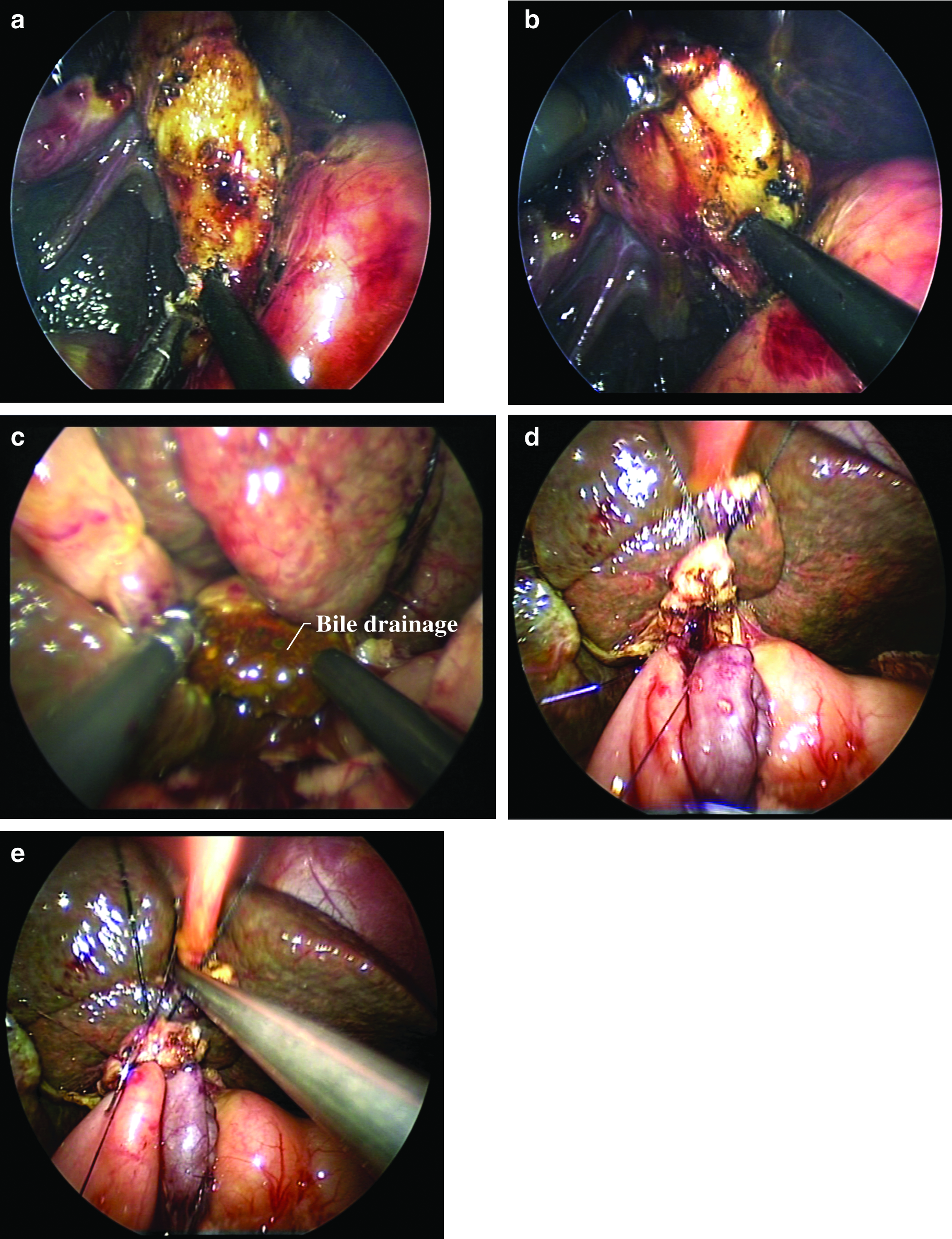
Single-incision laparoscopic hepaticojejunostomy for correctable biliary atresia:
An individualized length (based on the distance between umbilicus and the liver hilum) of the jejunal Roux loop was fashioned extracorporeally through the enlarged umbilical wound, as previously described. 6 The mesenteric defects were closed extracorporeally. The Roux loop was then brought to the hepatic hilum through the retrocolic route laparoscopically. In this series, the proximal common hepatic ducts in all patients were adequately large enough for end-to-side anastomosis (diameters in Type I BA of 1.0 cm and in Type II of 0.5 cm [i.e., correctable BA]). The hepaticojejunostomies were carried out. Anastomosis started at the 6 o'clock position of the bile duct and headed to the 9 and 3 o'clock positions separately using a continuous suture. The sutures were tied at the 9 and 3 o'clock positions simultaneously when the posterior wall anastomosis finished (Fig. 4d). The anterior wall anastomosis was completed by continuous suture along the 3–12–9 o'clock direction using the same polydioxanone suture (Fig. 4e). The diameter of the anastomosis was 0.5–1.0 cm. No abdominal drainage tube was placed.
According to the intervention protocol in our department, patients were routinely given antibiotics, ursodeoxycholic acid, and Compound Glycyrrhizin (glycyrrhizin, glycine, and cysteine hydrochloride monohydrate, to improve liver function) postoperatively until the laboratory results returned to normal level after medicine cessation.
Patients were followed up in our clinic postoperatively at 1, 2, 3, and 6 months and will be seen every 6 months thereafter. The laboratory results and ultrasonographic findings were reviewed. Upper gastrointestinal studies were conducted to detect whether the patients had Roux loop reflux.
Results
All SILH procedures were completed laparoscopically without conversions. The median diameter and length of the cysts were 3.35 cm (range, 1.00–4.30 cm) and 2.50 cm (range, 1.50–2.90 cm), respectively. The median age at the time of operation was 21 days. The median operative time was 2.00 hours (range, 2.00–2.17 hours). Blood loss was minimal. No blood transfusion was required. Patients were given 7 (Type I BA) or 10 (Type II BA) days of intravenous antibiotics, ursodeoxycholic acid, and Compound Glycyrrhizin before discharge. The median postoperative hospital stays was 7.00 days (range, 7–11 days). The median duration to establish full diet feeding was 2.50 days (range, 2–3 days).
Up to now, the patients have completed 3–5 months of follow-up visit. The median follow-up duration was 4.5 months. All patients recovered uneventfully. Cholic stool passage started on postoperative Days 2–3. Jaundice gradually subsided on postoperative Days 3–5 in Type I BA patients and on Day 6 in the Type II BA patient. All patients with correctable BA were put on regular medications postoperatively. The total and direct bilirubin levels in Type I BA patients normalized 1 month postoperatively, whereas those of the Type II BA patient normalized 3 months postoperatively (Fig. 5). Liver function significantly improved in all patients. ALT, AST, and ALP returned to normal or near normal levels 3 months postoperatively. To date, no mortality or morbidity of cholangitis, bile leak, anastomotic stenosis, Roux loop obstruction, wound infection, and wound dehiscence/hernia were encountered. No intrahepatic reflux was observed in postoperative upper gastrointestinal contrast studies. The cosmetic outcome of SILH was superior to that of our conventional laparoscopic hepaticojejunostomy in patients with correctable BA (Fig. 6).
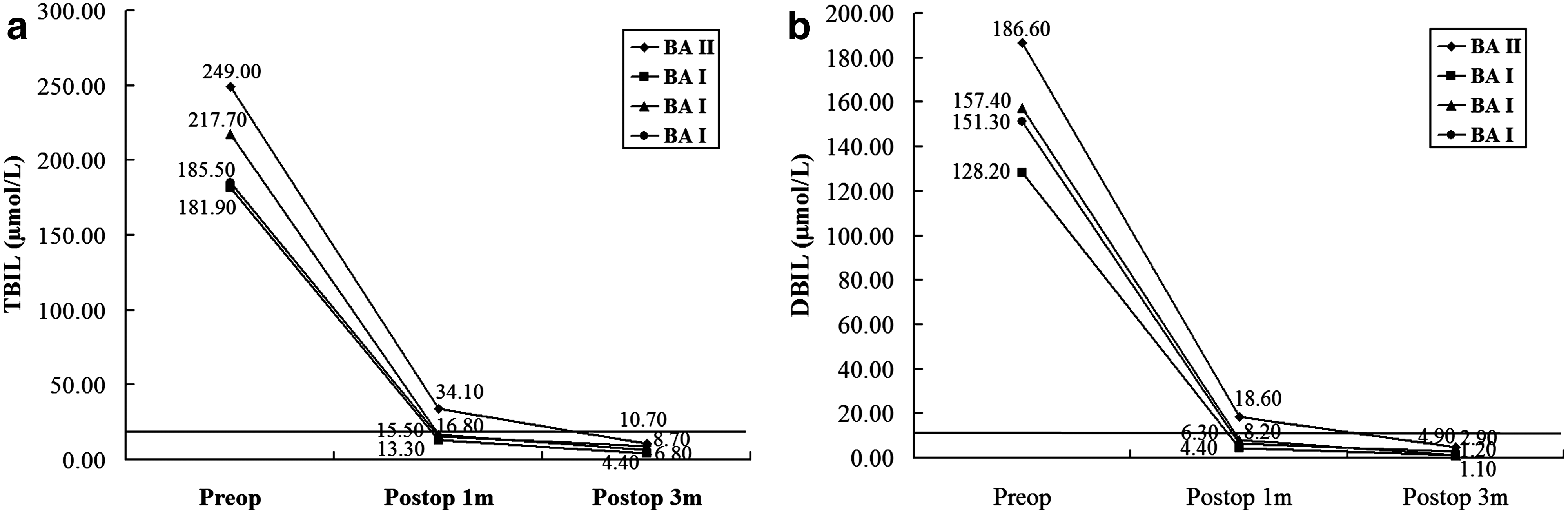
Perioperative serum bilirubin levels of neonates with correctable biliary atresia (BA) who underwent single-incision laparoscopic hepaticojejunostomy. DBIL, direct bilirubin; TBIL, total bilirubin; Type I BA, jaundice disappeared by 1 month postoperatively; Type II BA, jaundice disappeared by 3 months postoperatively.
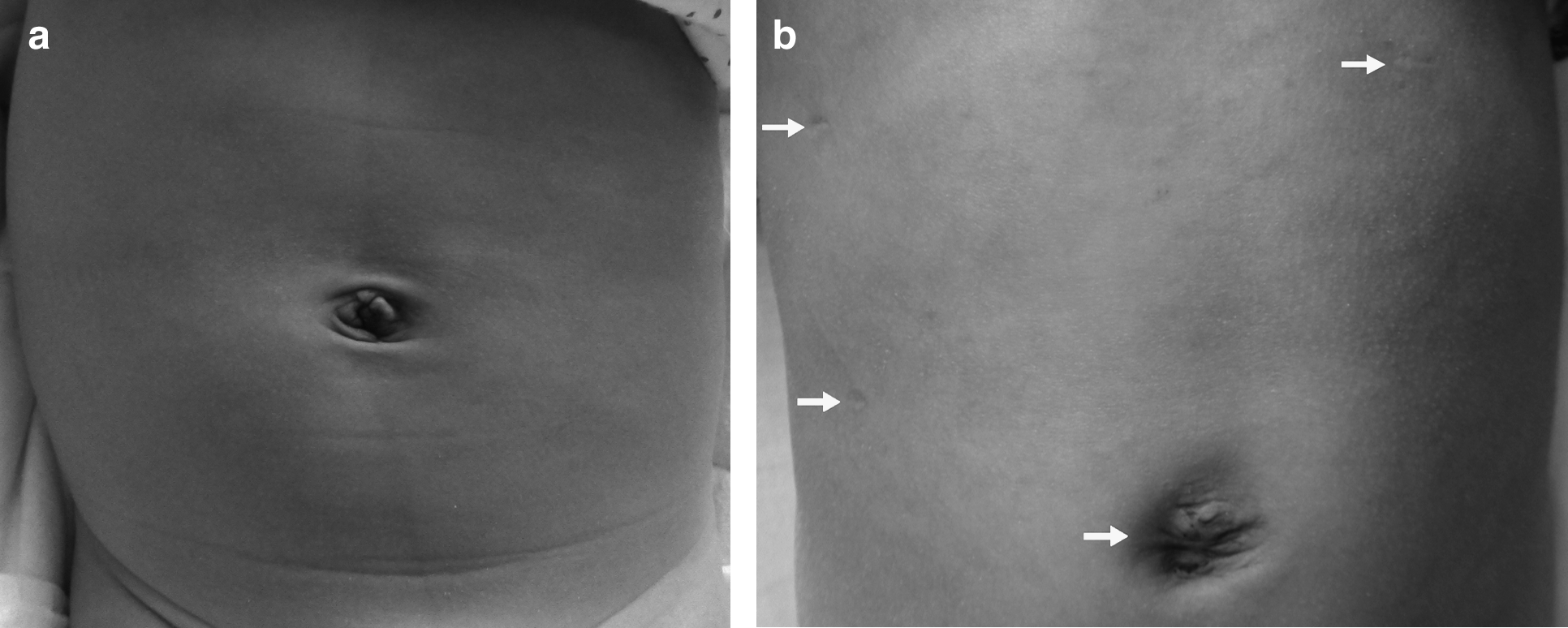
Cosmetic outcome of
Discussion
Over the last 3 years, single-incision laparoscopy has gained wider acceptance in the pediatric surgery practice. The operations include appendectomies, cholecystectomies, pyloromyotomies, enterolysis, ovarian cystectomy, inguinal hernia repairs, Nissen fundoplications, and endorectal pullthrough procedures.1–4 The aim of single-incision procedures is to minimize scar size and wound pain. In this report, we reviewed our initial experience of SILH using conventional straight laparoscopic instruments treating correctable BA and assessed its safety and feasibility. To the best of our knowledge, this is the first series of SILH application in surgery for correctable BA.
We started the practice of SILH in correctable BA neonates after accumulating experience of conventional laparoscopic cyst excisions and Roux-en-Y hepaticojejunostomies in 30 correctable BA patients and 7 patients undergoing SILH for choledochal cysts. SILH application in choledochal cysts helped us to establish the logistics of the operation and overcome the technical challenge. The initial success in SILH for choledochal cysts prompted us to extend this technique further to cover correctable BA. Although technically demanding, SILH using conventional straight instruments could be safely accomplished by experienced laparoscopic surgeons without any major intraoperative complication. The operative time was shorter than that of SILH for choledochal cysts (mean, 3.06 hours) 7 and conventional open hepaticojejunostomy for correctable BA (mean, 3.4 hours) carried out by the same surgical team. 8 It may be attributed to the smaller cyst size (usually smaller than choledochal cysts), careful selection of correctable BA patients, and technical improvements. In the open procedure, the mean postoperative hospital stay was 6.8 days, 8 and 2 of the 7 (28.5%) patients had cholangitis during follow-up. The outcomes of the current series demonstrated that the postoperative recovery of SILH was comparable to that of open hepaticojejunostomy, and no postoperative cholangitis was observed in the SILH patients so far. BA patients often suffer from a certain degree of malnutrition and hepatic dysfunction. They have a higher rate of perioperative complications secondary to surgical trauma. In the conventional open procedure with a large muscle-cutting incision, dehiscence and hernias can occur in patients with hypoproteinemia and ascites, which are common features in BA. We believe that SILH potentially minimizes these complications and hence facilitates the healing.
Hepaticojejunostomy is recommended for correctable BA with proximal common hepatic duct diameter not less than 0.5 cm. For Type I and II BA with proximal common hepatic duct diameter less than 0.5 cm or for Type III BA (i.e., uncorrectable BA), Kasai portoenterostomy was recommended. Under the laparoscope, the BA classification can be confirmed by the cholangiogram. Moreover, hepaticojejunostomy can be achieved for correctable BA. This can also be easily converted to open Kasai portoenterostomy for uncorrectable BA.
Recently, a rat experiment showed that elevated intra-abdominal pressure decreased hepatocyte proliferation and induced liver cell apoptosis. 9 Ure and co-workers reported that CO2 pneumoperitoneum temporarily altered the metabolism and function of various abdominal cells, including hepatic macrophages; these were thought to affect the results of the laparoscopic Kasai procedure for BA patients with a compromised liver cell function or hepatic fibrosis.10–12 However, CO2 pneumoperitoneum has not been proven to have such effects on patients with choledochal cysts, even in those combined with liver malfunctions or Grade III and IV hepatic fibrosis. Poor results in previous small series of laparoscopic surgery for BA13,14 may result from difficulties in portal plate dissection, hemorrhage control, or anastomosis. Laparoscopic Kasai portoenterostomy is a challenging and technically demanding procedure. It requires a high case volume and a longer learning curve to acquire the technique as well as proficiency in both hepatobiliary surgery and advanced laparoscopic surgery. It also depends on whether BA is of the correctable type. To date, there is no study to compare the efficiency of laparoscopic versus open surgery in the different subtypes of BA.
Meticulous dissection and anastomosis under magnified vision provided by the laparoscope effectively reduce bleeding or bile leak. Drainage does not prevent or treat these complications. Instead, drainage-related complications (e.g., fever, wound infection, wound hernia, or hemorrhage) may cause unnecessary discomfort to patients, which defeats the purpose of minimal invasive surgery. 15 Therefore, the drain tube is not routinely placed in BA patients in our center.
The initial result of SILH for correctable BA is promising. However, more patients and long-term follow-up are required to assess whether the procedure is equally safe and effective in achieving jaundice clearance as compared with open procedures.
In conclusion, SILH for correctable BA can be performed safely by surgeons experienced in both conventional hepatobiliary surgery and advanced laparoscopic surgery. It provides a viable alternative for correctable BA.
Footnotes
Disclosure Statement
No competing financial interests exist.