
Abstract
Abstract
The introduction of robotics in head and neck surgery has facilitated access to the contents of the neck region using less cosmetically obtrusive incisions. Robotic systems offer a three-dimensional viewing, tremor filtration, and articulating distal arms that mimic natural hand and wrist movements. We hypothesized that these characteristics would allow for the performance of a robotic-assisted selective and comprehensive neck dissection via combined pre- and post-auricular incisions. We were able to demonstrate adequate access in a cadaver, using a combination of conventional, endoscopic, and robotic surgical manipulation. Thus preclinical cadaver studies support the ability to perform robotic-assisted neck dissection via combined pre- and post-auricular incisions.
Introduction
The introduction of robotic surgery in head and neck surgery brings the advantages of three-dimensional magnification, increased degrees of freedom with the effector arms, tremor filtration, fine dissection, and an articulating distal end that mimics hand movements. The da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) robot is now one of the options in the transoral resection of tumors in the upper aerodigestive tract. This new technology has been applied clinically in procedures such as modified radical neck dissection (levels 2–5b) with thyroid surgery. 3 Although this approach requires an axillary approach to perform the thyroid surgery and neck dissection while achieving optimal cosmesis, there is a considerable anatomical distance if this approach is applied to selective or comprehensive neck dissection. This problem was addressed by Kim et al. 4 using robotic-assisted neck dissections (RANDs) via transaxillary and retroauricular approaches.
We present here our preclinical cadaver study using the da Vinci Surgical System, to determine if it is feasible to do robotic-assisted selective and comprehensive neck dissection through pre- and post-auricular incisions.
Materials and Methods
Two cadavers with an intact arterial and venous system were injected with colored latex (red, artery; blue, vein) to visualize the arterial and venous components of the neck during neck dissection. Injected latex assisted in determining if any vessels were missed or injured during neck dissection. Both the right and left neck of the cadaver was dissected. The cadavers were obtained from the Maryland State Medical Examiner according to institutional approval.
Lymph node levels were divided into 1a (submental nodes), 1b (submandibular lymph nodes), 2a (upper jugular lymph nodes), 2b (submuscular recess), 3 (middle jugular nodes), 4 (lower jugular nodes), 5a (spinal accessory lymph nodes), and 5b (transverse cervical and supraclavicular lymph nodes) according to the American Joint Committee on Cancer 2 (Fig. 1). Selective neck dissection (levels 1–4) was performed in both sides of the neck of one cadaver, while comprehensive neck dissection (levels 1–5) was performed on both sides of the neck of the other cadaver.

Lymph node levels. © The Johns Hopkins University, 2012.
Dissections were done in the following order: open or traditional neck dissections were done for levels 2a, 2b, and 3 for selective neck dissection and in levels 2a, 2b, 3, and 5 for comprehensive neck dissection. Levels 1a, 1b, and 4 neck dissections were done using the da Vinci Surgical System robot on both types of neck dissection. The operative and setup times were noted. After the RAND, the areas of dissection were then inspected by another head and neck surgeon to determine completeness of resection and for any missed or injured vessels.
The average numbers of lymph nodes per lymph node level in RAND were then compared with those by historical open cadaver lymph node dissection in the study of Friedman et al. 5
Results
One cadaver was draped for a bilateral selective neck dissection (levels 1–4). The other cadaver was draped for bilateral comprehensive neck dissection (levels 1–5). The da Vinci Surgical System robotic platform was positioned opposite the operative site. The pre- and post-auricular hairline incisions were marked (Fig. 2). We only used a 4.5-cm post-auricular incision. The post-auricular hairline incision was beveled to avoid the hairline follicles followed by identification of the lateral border of the sternocleidomastoid (SCM) muscle and Erb's point. The greater auricular nerve was identified and preserved. A subplatysmal flap was raised, avoiding injury to the cervical branch of the facial nerve, using a lighted breast retractor and an extended guarded Bovie tip. The Thompson retractor was then inserted and positioned. It was later adjusted for level 1 and 4 dissections. The Thompson retractor was able to suspend the flap with no undue motion of retractor during the surgery (Fig. 3). It provided a very stable working environment and was not displaced during or after the procedure.

Post-auricular hairline incision with pre-auricular extension for additional exposure.

Thompson retractors and robotic positioning.
Laparoscopic 5-mm and 10-mm clip applicators were used for vessel hemostasis in addition to the Harmonic scalpel. The 5-mm and 10-mm laparoscopic instruments were used in assisting during RAND by the bedside assistant.
Because levels 2a, 2b, and 3 were directly accessible through the incision, cervical lymph nodes of these levels were dissected in a standard open neck dissection in both types of neck dissection. The anterior border of the SCM was released for selective neck dissection, while the posterior border of the SCM was released for the comprehensive neck dissection. The spinal accessory nerve was identified and preserved. The internal jugular vein, vagus nerve, and carotid artery were identified and exposed via open standard neck dissection of levels 2a, 2b, and 3. Levels 2a, 2b, and 3 were removed en bloc on both types of neck dissection, while levels 5a and 5b were removed in the comprehensive neck dissection. At this stage, only levels 1 and 4 were undissected, and with the removal of levels 2a, 2b, and 3, there was a better visualization of levels 1 and 4.
We then proceeded in the dissection of level 4. The anterior two-thirds border of the SCM was sutured with 2-0 silk suture to the posterior incision site, thus providing retraction and exposure of the level 4 lymph node area. The medial head of the SCM was also retracted by the Thompson retractor, and thus additional exposure to level 4 was gained. An opening was created along the surgical planes of dissection of the digastric muscle and in the carotid sheath. The da Vinci Surgical System robotic platform was then positioned opposite of the incision site and placed in a 30° angle to the operative table. A 0° or 30° three-dimensional camera was used depending upon the exposure and visualization of the operative site. The three-dimensional camera and two robotic arms were inserted in the incision site. A 5-mm Maryland dissector and a Harmonic scalpel were then inserted in their respective robotic arms. A 5-mm spatula cautery tip was also used for dissection and cauterization.
The omohyoid was resected, and level 4 tissue was dissected off the internal jugular vein, vagus, and carotid artery. The phrenic nerve was identified and preserved. The inferior limit of level 4 was transected just above the clavicle. The transverse cervical vessels were identified and ligated. The cervical rootlets were preserved in the selective neck dissection (Fig. 4).
Dissection of the posterior belly of the digastric muscle.
Although traditional neck dissection requires en bloc dissection, we opted to do it for levels 2a, 2b, and 3 en bloc for the selective neck dissection and levels for 2a, 2b, 3, and 5 for comprehensive neck dissection. The ones most distal to our incision (levels 1 and 4) were independently removed using the da Vinci Surgical System robot.
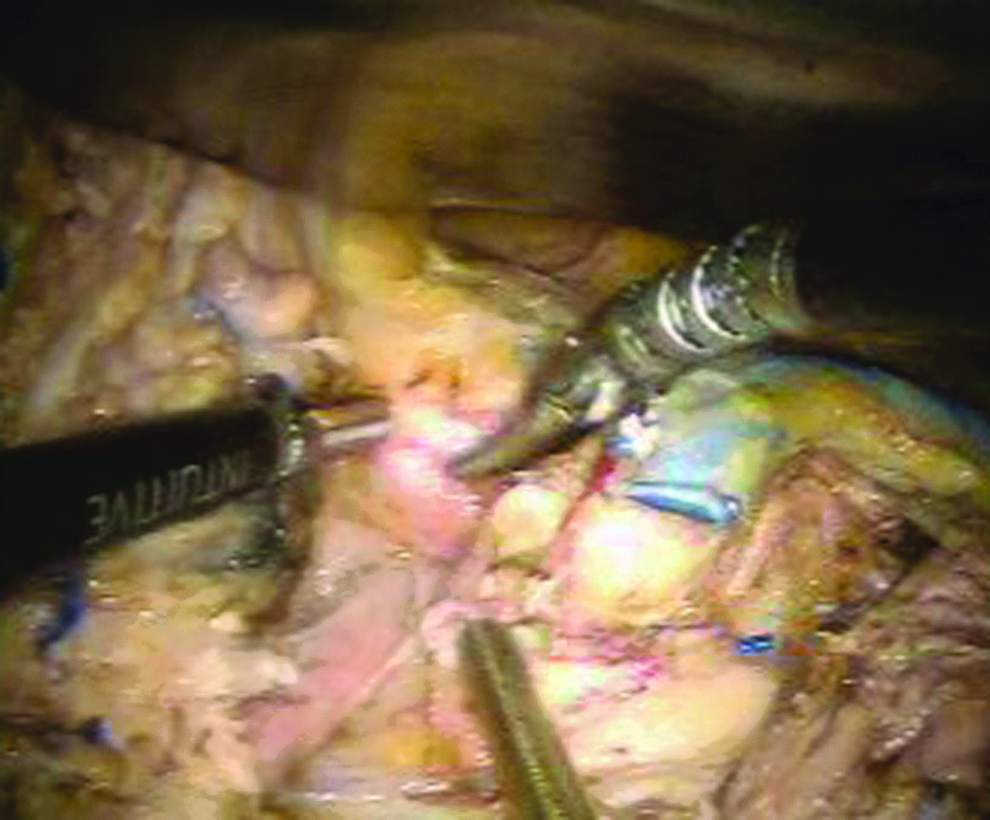
Level 1b was dissected starting with the exposure of the anterior and posterior belly of the digastric muscle (Fig. 5). The submandibular gland was freed posteriorly. The facial artery and vein entering the submandibular gland inferiorly were ligated. The facial artery and vein in the superior border of the submandibular gland were isolated individually and ligated (Fig. 6). The marginal branch of the facial nerve was also isolated and preserved.

Ligation of the facial artery during level 1b dissection.
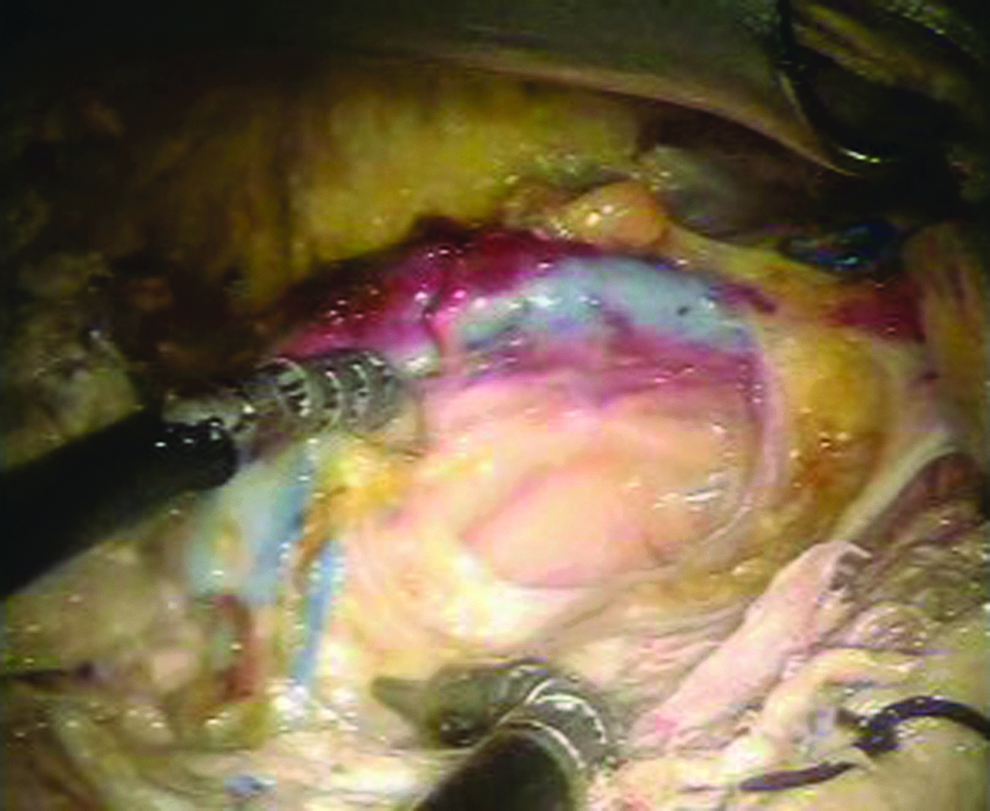
Floor of the neck after dissection with identification of the internal jugular vein, vagus nerve, and carotid. The fascia of the floor was intact.
The submandibular gland, level 1b nodes, and facial nodes were retracted superiorly and medially to visualize the floor of the submandibular triangle, exposing the submandibular duct and visualizing the lingual nerve. The lingual nerve was freed from the submandibular gland. The mylohyoid muscle was retracted by the robotic arm, followed by clipping and transaction of the submandibular duct. Level 1b was removed, and level 1a was dissected. The hypoglossal nerve was identified and preserved.
Lymph node levels 1–4 (selective neck dissection) and levels 1–5 (comprehensive neck dissection) were visually inspected by another head and neck surgeon. There were no iatrogenic injuries noted.
The robotic setup time averaged 13 minutes. The operative times averaged 158 minutes for the comprehensive neck dissection and 134 minutes for the selective neck dissection. The specimen (Fig. 7) was inspected, labeled, and sent for histopathologic examination for lymph nodes (Table 1).

Resected right neck lymph node levels 1–4.
Because the Harmonic scalpel instrument is a nonarticulating distal instrument, the pre-auricular incision allowed the full utility of the instrument by increasing the angulation of entry of the robotic arm with the Harmonic scalpel, especially during level 4 dissection. These limitations were not observed if the instruments used were the distal articulating instruments. We prefer to use the Thompson retractor because of its adjustable, different configuration of blades available, and its versatility and because it is readily available in our institution.
The range of the number of lymph nodes per lymph node level on the open cadaver neck dissection by Friedman et al. 5 were compared with our results. Our results were all within range of the lymph nodes resected on open cadaver neck dissection (Table 2).
RAND, robot-assisted neck dissection.
Discussion
The presence of cervical lymph node metastasis, whether or not clinically apparent, profoundly affects the morbidity and mortality of a head and neck cancer patient. 2 It is responsible for 50%–95% of recurrent disease. 3 Although Ebling 2 noted that 20%–30% of patients have cervical metastasis without clinical or radiologic evidence of nodal involvement, the incidence of occult lymph node metastasis must be stratified in relation to the stage of the disease, histologic risk factors, depth of invasion, and location of the primary tumor.
The type of treatment of the neck depends upon several parameters, such as site of the tumor, T stage of the primary cancer, treatment modality selected for the primary cancer, the desires of the patient, cosmesis, functional results, and the probability of occult metastases. Determining accurately the pathologic stage not only will dictate the need for further adjuvant therapy, but also determine the prognosis of the patient.
The type of neck dissection depends on the lymph node group that is at greatest risk for metastasis from the primary tumor. In general, levels 1–4 are involved for primary tumors of the oral cavity and oropharynx, levels 2–4 for laryngeal and hypopharyngeal tumors, and levels 2–5 for lesions in the occipital post-auricular and suboccipital region.1,6 For thyroid cancer, the pattern for cervical lymph node metastasis commonly occurs in levels 2a, 3, 4, and 5 with a low incidence in other levels.1,7 Montes et al. 8 noted that squamous cell carcinoma of the maxillary palate, alveolar, and gingival exhibits an aggressive behavior and recommended levels 1–3 neck dissection for T2, T3, and T4 cancers at the time of resection.
In the experience of Kang et al., 3 RAND is technically feasible and safe and produces good cosmetic results in patients with low-risk well-differentiated thyroid cancer with lateral neck and central neck involvement done through an axillary approach; no major injury occurred in the RAND in their study. Although this procedure was designed to address thyroid cancer with central and lateral neck metastasis, its utility or application to head and neck cancers with neck metastasis, in our opinion, has limitations. Although this problem was addressed by Kim et al., 4 it still requires a post-auricular and transaxillary approach.
In a review of different endoscopic approaches to the neck by Muenscher et al., 9 the procedures were not only feasible, but also without major complication; although improved cosmetic outcomes were noted, operative time was prolonged. Terris et al. 10 in their work on robotic resection of the submandibular gland in a cadaver model has proven that robotic endoscopic surgery is feasible in that setting.
Lee et al. 11 commented that robotic surgery may overcome the intrinsic limitations of traditional endoscopic surgery, providing a surgeon with a three-dimensional view of the operating field and digitally suppressing physiologic hand tremors. In addition, it may offer motion scaling and superior dexterity, precisely reproducing and enhancing movements of the human wrist and fingers. Moreover, the stability of the view and the possibility of performing meticulous movements may make the robotic Da Vinci Surgical System especially appropriate when fine manipulation of tissues in a deep and narrow operative field is needed as in the case in head and neck surgery. 11 It also gives the surgeon ambidextrous capability. 11 The above-mentioned advantages were demonstrated when Kim et al. 4 performed a robotic neck dissection through transaxillary and post-auricular incisions. The same concept and advantages were also demonstrated when Terris and co-workers reported their results on robotic facelift thyroidectomy.12,13
A facelift incision or pre- and post-auricular incision puts the greater auricular nerve at risk. However, careful anatomical studies and surgical techniques derived from parotid surgery, robotic facelift thyroidectomy,12,13 and facelift surgery allow for a consistent preservation of this nerve.
The cervical branch of the facial nerve exits the parotid in the anterior inferior region of the tail of the parotid. 14 Careful release of the retaining ligaments in the region of the submandibular gland will allow full mobilization of the medial platysma without injuring the cervical nerve. 14
A subauricular band along the incision site can occur after a facelift incision. To prevent this band, Rohrich et al. 15 subdivided the periauricular fat into five compartments, namely, superior, middle, inferior, subauricular, and pre-auricular. With adequate release of the lateral neck and post-auricular dissection with accompanying subauricular membrane release, the subauricular band could be avoided. In the present study, the release of the aforementioned areas was done prior to doing the subplatysmal flap.
Mckinney's point is where the greater auricular nerve enters the Loré's fascia or tympanoparotid fascia. 15 The region between Erb's point and Mckinney's point, in which the nerve lies in the SCM, is the vulnerable point of the nerve because it lies closer to the skin and it is only covered by fat. Awareness of this anatomical characteristic and careful dissection will likewise prevent greater auricular nerve injury.
The digastric muscle is superficial to the external carotid artery, internal carotid artery, hypoglossal nerve, and internal jugular vein. The spinal accessory nerve passes over the jugular vein and is posterior to the belly of the digastric muscle.2,16 Using the digastric tunnel as described by Wein and Weinstein 16 allows for the safe and early identification of critical structures in this region. Because the lymph node levels 2a, 2b, and 3 were accessible with the pre- and post-auricular incisions, we prefer to do traditional, open dissection of this region, facilitating structure identification, lessening operative time, and better visualization of level 1 and 4. The pre-auricular incision is especially useful in the exposure for level 4 and also facilitates use of the nonarticulating Harmonic scalpel.
A study by Tesseroli et al. 17 comparing en bloc resection (resection of primary tumor in continuity with neck dissection) versus non–en bloc resection (primary tumor resection with a noncontinuous neck dissection) in oral cancer revealed no statistical significant difference in the two groups with regard to disease-free survival. Although RAND is not an en bloc neck surgery, this remains to be proven in a future clinical study.
The phrenic nerve lies immediately under the enveloping fascia of the anterior scalene muscles. Thus violation of the fascia from the muscle may cause inadvertent injury.2,16 In our robotic neck dissection, the fascia was easily visualized and preserved.
Terris and co-workers have reported clinical experience on thyroid surgery using the da Vinci Surgical System through a facelift incision.12,13,18 Because of the accessibility of levels 5a and 5b, through pre- and post-auricular auricular incisions, it is theoretically possible to do thyroid surgery with a modified neck dissection using the aforementioned approach. Hemostasis using the Harmonic scalpel has been proven to be safe and comparable to standard hemostasis.19,20
Although RAND has an advantage of cosmesis, three-dimensional magnification, increased degrees of freedom with the effector arms, tremor filtration, fine dissection (especially along the major blood vessels at level 4), and an articulating distal end that mimics hand movements, its main shortcoming will be the expense for the use of the da Vinci Surgical System: it is only used in the distal portion of the neck of the neck dissection and has two phases in the procedure (open surgery and robotic surgery).
Depending upon the extent of the neck disease and type of neck dissection, the operative times range from 120 minutes to 240 minutes (2–4 hours).21,22 The RAND operative times in our study are 158 minutes (for comprehensive neck dissection) and 134 minutes (for selective neck dissection), which are comparable to the open neck dissection.
The possible initial clinical application of RAND would be in a nonradiated N0 or N1 neck disease, with the nodes not fixed or adherent to neurovascular structures based on physical examination and imaging studies. RAND can surgically remove the different lymph node levels in the neck and is technically feasible, but the clinical application of this technique should be studied in a prospective randomized clinical trial, comparing open selective neck dissection, open comprehensive neck dissection, endoscopic neck dissection, and RAND with regard to oncologic control, operative time, hemostasis, cosmesis, economics, and postoperative morbidity.
Conclusions
Preclinical cadaver studies on robotic-assisted selective and comprehensive neck dissections are technically feasible through pre- and post-auricular incisions. A pre-auricular incision can further enhance exposure and access. Laparoscopic 5-mm and 10-mm instruments can be used to assist and clip vessels.
Footnotes
Acknowledgments
We thank Richard Hirata, MD, FACS, and James Scuibba, DMD, PhD. This work was supported by the Milton J. Dance Endowment.
Disclosure Statement
No competing financial interests exist.