
Abstract
Abstract
Background:
The purpose of this study was to evaluate the learning curve of the laparoscopic approach for colorectal cancer and generate a focused training program for more junior surgeons.
Subjects and Methods:
This study analyzed data from 100 consecutive laparoscopic surgeries for colorectal cancer between January 2009 and July 2010. The learning curve was compared between the first 50 surgeries (study group 1) and the subsequent 50 surgeries (study group 2).
Results:
Age, gender, mean body mass index, history of abdominal surgery, and tumor stage were not significantly different between the two study groups. Operative time decreased with increasing experience and reached a plateau after 23 patients. The operative time in study group 2 tended to be shorter than in study group 1 (P=.06). Other parameters including blood loss, average number of retrieved lymph nodes, conversion rate, and intraoperative complication rates were not different between the two study groups.
Conclusions:
More junior surgeons can be safely trained if they are exposed to a focused training program. Supervision by an experienced surgeon and considerable experiences in open colorectal surgery are assets for an accelerated learning curve.
Introduction
In general, laparoscopic colorectal surgery is safe and feasible5–8 ; however, there are still some surgical challenges. Inadequate laparoscopic procedures may lead to complications and poor survival. Several studies indicated that complication rates decrease as surgeons gain experience.9–11 One of the most common methods to gauge the learning process is evaluation of the “learning curve.” 12 An accelerated learning curve is the key to improving short-term outcomes. 13 Both operative risks and oncological results should be taken into consideration during the initial learning curve. To date, the learning process for the laparoscopic approach to colorectal cancer has not yet been clearly described.
In general, trainees start in a conventional training program with basic procedures such as appendectomy, cholecystectomy, and hernia repair.14–16 It was not clear whether the training program for the more junior surgeons should be different from a conventional training program. Indeed, a conventional training program may not be necessary for them. The objective of this study was to evaluate the feasibility and short-term outcomes of laparoscopic surgery for colorectal cancer performed by the more junior surgeons and to assess the learning curve. We further discuss the need to generate a focused training program for more junior surgeons at a cancer-specializing center.
Subjects and Methods
Patient selection for laparoscopic surgery
From January 2009 to July 2010, 100 patients underwent laparoscopic colorectal cancer surgery at The Tumor Hospital of Harbin Medical University, Harbin, China. Patients received preoperative intravenous antibiotics and a mechanical bowel preparation. All patients were encouraged to eat and drink as soon as possible after the surgery. Informed consents were obtained for all procedures.
Because the present study was designed to evaluate the learning curve for laparoscopic colorectal surgery, difficult cases were excluded from the present study. Exclusion criteria were as follows: body mass index of >35 kg/m2, extensive previous abdominal surgery, palpable fixed tumors, tumor of splenic flexure, and intestinal obstruction. The more junior surgeons had more than 10 years of experience in open colorectal surgery and had performed more than 300 open colorectal surgeries per year for the past 3 years. Furthermore, they had completed the laparoscopic training program in our hospital and had been an assistant in more than 100 laparoscopic colorectal operations during the laparoscopic training program. All surgeries were supervised by experienced staff surgeons who previously had performed more than 300 laparoscopic surgeries.
Patient characteristics included age, gender, body mass index, American Society of Anesthesiologists score, history of abdominal surgery, tumor stage, and tumor location. Operative procedures, operative time, intraoperative complications, blood loss, number of lymph nodes harvested, positive resection margin, conversion to open surgery, and surgical outcomes were prospectively recorded. Conversion to open surgery was defined as any case that could not be completed laparoscopically as planned.
To evaluate the learning curve, surgeries were grouped into the first 50 cases (study group 1) and subsequent 50 cases (study group 2). The aforementioned outcome parameters were compared between the twoh study groups.
Technical considerations and operative strategy
Standardized procedures were performed in all cases. Laparoscopic left-sided colon resection began with ligation of proximal vascular pedicles followed by mobilization and resection of bowel with anastomosis. For right-side surgery, the bowel was laparascopically mobilized, and division of blood vessels, bowel resection, and anastomosis were performed extracorporeally through a small extension of the midline trocar incision.
For rectal cancer, the total mesorectal excision was completed intracorporeally. The rectum was mobilized as far distally as required by tumor location with attempts to keep the mesorectal fascia intact. The rectum was divided using articulating endoscopic linear staplers to achieve a distal margin of ≥2 cm. After placement of the anvil of the endoluminal circular stapling device in the proximal bowel segment, an anastomosis was performed intracorporeally using a standard double-stapling technique. 17 A perineal dissection for abdominoperineal excision of rectum was then performed, and the resected specimen was retrieved through the perineal wound. The D3 dissection was performed when indicated.
Statistical analysis
We used the moving average method (specifically, a moving average of four) to analyze the data. For example, an average of the first four values was calculated (=first moving average); with the addition of another variable, an average of the last four values was calculated (=second moving average), and so on. For construction of a smoothed learning curve and analysis of the operating time, these moving averages were used. All numerical values are expressed as median (range). The differences between study groups 1 and 2 were analyzed using Fisher's exact test, chi-squared test, or Mann-Whitney U test where appropriate. Analysis was performed with statistical software (SPSS version 13.0; SPSS Inc., Chicago, IL), and differences were considered significant at P<.05.
Results
In total, 100 patients were included in this study. Demographic characteristics of study patients are shown in Table 1. The age, gender, body mass index, history of abdominal surgery, and tumor stage were not significantly different between study group 1 (first 50 laparoscopic surgeries) and 2 (last 50 laparoscopic surgeries). Sixty-two (62%) patients suffered from colon cancer, whereas another 38 (38%) patients had rectal cancer. According to the clinical TNM classification, there were 5 cases with stage I, 39 with stage II, 52 with stage III, and 4 cases with stage IV tumors (Table 1). Tumor locations were significantly different between study groups 1 and 2. Specifically, the percentage of tumors in the ascending or transverse colon and rectum was lower, whereas the percentage of tumors in the cecum or descending and sigmoid colon was higher, in study group 1 compared with study group 2 (P=.02) (Table 1).
Data are number of patients (%) unless indicated otherwise.
ASA, American Society of Anesthesiologists; BMI, body mass index; NS, not significant.
Operative procedures were significantly different between the two study groups (Table 2). Specifically, the percentages of right hemicolectomies, transverse colectomies, anterior resection, and abdominoperineal excision of rectum were lower, whereas the percentages of left hemicolectomies and sigmoidectomies were higher, in study group 1 compared with study group 2 (P=.04) (Table 2). Average operating time, blood loss, and number of retrieved lymph nodes were comparable between the two study groups (Table 2). No intraoperative complications or patients with positive resection margins were found in either study group. Conversion to open surgery was required in 1 patient in study group 2 (2%) because of locally advanced disease.
Data are number of patients (%) unless indicated otherwise.
APER, abdominoperineal excision of rectum; NS, not significant.
The moving average of the learning curve for study group 1 is shown in Figure 1. The operative time was longer than 240 minutes in the first 8 cases. The operative time gradually decreased with increasing experience (Fig. 1).
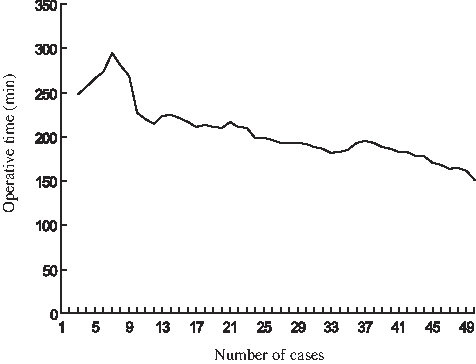
Learning curve in study group 1 calculated using the moving average method (see Statistical analysis for more details).
Surgical outcomes are presented in Table 3. The time to flatus, time to bowel opening, and postoperative hospital stay were similar between the two study groups. Anastomotic leakage occurred in 1 patient who underwent a sphincter-saving surgery in study group 2. Postoperative complications were not significantly different between the two study groups, although they tended to be slightly higher in study group 1 compared with study group 2 (20% versus 14%, P=.06) (Table 3). There was no mortality in either study group.
Data are number of patients (%) unless indicated otherwise.
NS, not significant.
Discussion
Laparoscopic procedures used for colorectal cancer have recently become a standard in many hospitals. Several randomized controlled trials demonstrated the benefits and safety of laparoscopic colorectal surgery, making it now the preferred approach in the surgical management of colorectal cancer.18,19 Although laparoscopic colorectal surgery is performed more frequently, implementation of laparoscopic colorectal procedures is still challenging because they require a longer training period. 20
Various laparoscopic training programs are available, but their efficiency is not clear. 21 The traditional training paradigm is being challenged in many centers. As a result, clinicians are trying to define the most cost-effective and efficient training program in order to shorten the learning curve. 22 In addition, a traditional training program does not fit all trainees. Surgeons in traditional training will need to learn laparoscopic techniques without ever having performed the procedure in the open way. The shape of the learning curve may vary depending on individual experiences and innate skills. We hypothesized that this laparoscopic training program would help to shorten the learning curve for trainees. The purpose of this study was to assess the learning curve of the training program. In the present study, intensive training of surgeons may be an important key to shorten the learning curve and limit its impact on the outcome of the patient.
First, trainees in this program start with basic laparoscopic training. Previous studies demonstrated that initial mastering of basic skills enhances skill acquisition and reduces resource requirements for training. 22 During this process, using the operating room for basic skill training in laparoscopy may be inefficient and expensive. A simulation on inanimate or animate models allows trainees to acquire new skills and learn new procedures in a safe and non-threatening environment before performing these tasks on patients. Trainees practice the video trainer and animal dissection tasks, during which they are personally guided by an experienced staff surgeon. According to our experience, an intense laparoscopic training improves the video–eye–hand skills, and trainees obtain a deeper understanding of anatomy, gain experience in laparoscope manipulation, and learn to provide countertraction. It has previously been reported that surgeons who regularly play video games are generally more skilled at performing laparoscopic surgery. 23 We downloaded video games from the World Laparoscopy Hospital (http://training.laparoscopyhospital.com) to develop the trainees' laparoscopic skills.
Second, the trainees attend advanced laparoscopic training courses, once they become familiar with basic laparoscopy. After attending these courses, laparoscopic surgeons should be able to confidently perform all procedures taught by themselves on their patients. Through skill laboratories involving surgical trainers, animal models, or other simulated operating conditions, many advanced laparoscopic skills, such as intracorporeal suturing, are acquired. It is generally believed that laparoscopic colorectal surgery requires experience of laparoscopic cholecystectomy. However, the trainees in our program start with assisting in laparoscopic colorectal surgeries performed by an experienced surgeon instead of starting with laparoscopic cholecystectomy or appendectomy. As an assistant, it is important to accumulate a sufficient number of cases within a short time. 24 The trainees are required to assist more than 100 laparoscopic colorectal surgeries before being able to independently start their first case as operators.
Previous publications suggested that the learning curve for laparoscopic colorectal surgery ranges from 30 to 100 cases.20,25 In our study, the moving average stabilized after 23 cases. Our results, therefore, suggest that a surgeon is able to safely perform the operation at a relatively early stage. It needs to be mentioned, though, that initial cases were highly selected. In general, sigmoidectomy is regarded as a simpler procedure to perform; therefore, the percentage of sigmoidectomies was higher in study group 1 (i.e., the beginner's phase) than in study group 2 (44 versus 16%, respectively).
There are several reasons why we were able to accelerate the learning curve in our training program. Our more junior surgeons were already extremely experienced in open colorectal surgery. With this experience, the trainee exhibited an excellent ability to identify and dissect tissue planes with the usual tactile clues and a capability to control multiple blood vessels. Additionally, the supervision by experienced surgeons certainly helped to solve laparoscopic surgery problems in the beginning of the learning curve, especially in the identification of anatomical structures and planes of dissection. Under proper supervision, good results can be obtained even when a surgeon is relatively inexperienced. The new training program and the considerable experience of open surgery made a significant influence to the length of the learning curve.
The patient's safety is the major concern during the training program. 14 Our study provides evidence that skills of laparoscopic colorectal surgery can be taught and acquired safely under the proposed training program. It is important to evaluate operative times, complication rates, conversion rate, and blood loss to evaluate the learning curve. In our study, operative time decreased as the surgeon became more experienced and was slightly shorter during the later stages of the training (i.e., study group 2). Several other studies have also demonstrated the impact of the surgeon's experience on complications, showing a significant decrease in the complication rate as trainees gain experience.26,27 The conversion rate during the learning curve was notably low in our study. Specifically, only 1 case of conversion to open surgery occurred in study group 2 and none in study group 1. There were no serious complications during the entire training program. Complications were seen more often initially (i.e., study group 1), although no significant differences were found between the two study groups.
Our study had several limitations. It was not primarily designed to analyze long-term oncological outcomes of laparoscopic colorectal surgery, which would require a subsequent follow-up. Because our center is a high-volume cancer-specializing center, the results of this study may not be directly applicable to the training of surgeons in a general hospital with a low volume of laparoscopic colorectal surgery.
In conclusion, we demonstrated that laparoscopic colorectal surgery can be safely taught to more junior surgeons. Supervision by an experienced surgeon and extensive experience in open colorectal surgery are required for an accelerated learning curve.
Footnotes
Disclosure Statement
No competing financial interests exist.