
Abstract

Oral Abstracts
Basic Science
The Protective Effects of Ischemic Preconditioning and Postconditioning on Liver Ischemia/Reperfusion Injury in a Rat Model of CO2 Pneumoperitoneum
Objective: To investigate the protective effects of ischemic preconditioning and postconditioning on liver ischemia/reperfusion injury in a rat model of CO2 pneumoperitoneum (P).
Methods: 24 male SD rats were randomly divided into 4 groups, pneumoperitoneum (P group), ischemic preconditioning (IP group), ischemic postconditioning (IPo group), and control (C group). C group was subjected to sham operation. Other groups were subjected to the CO2 pneumoperitoneum, 15 mmHg intra-abdominal pressure (IAP). P group was subjected to 60 min of P, followed by 30 min of deflation (D). IP group was subjected to preconditioning prior to P/D, which consisted of 10 min of P, followed by 10 min of D. IPo group was subjected to 60 min of P, followed by three cycles of 1 min of D and 1 min of P and 30 min of D. Plasma alanine aminotransferase (ALT) and aspartate aminotransferase (AST), as well as homogenized tissue malondialdehyde (MDA) and nitric oxide (NO) levels, glutathione (GSH), and superoxide dismutase (SOD) activities were measured, respectively. The hepatic pathological changes were also observed by light microscopy. The expression of iNOS in liver tissue was examined by immunohistochemical technique in each group.
Results: Plasma ALT and AST as well as liver MDA levels were significantly increased, whereas liver SOD values were decreased in groups P, IP, and IPo, as compared to group C (P < 0.05). Plasma ALT, AST, as well as liver MDA and NO levels were significantly decreased, whereas liver SOD and GSH values were increased in groups IP and IPo, as compared to group P (P < 0.05). The biochemical markers except GSH were no significant difference between group IP and IPo. The iNOS concentration markedly decreased in group IP and IPo in comparison with group P.
Conclusions: ischemic preconditioning and ischemic postconditioning both can increase SOD and GSH levels and inhibit the expression of iNOS that can induce the production of NO, which may decrease hepatic I/R injury induced by CO2 pneumoperitoneum. Compared with IP, IPo increased GSH more prominently. It is suggested that IPo may play a greater role as protective effect on oxidative stress.
The Impact of Integrated Serum Proteomic and Metabolomic Profiling following Sleeve Gastrectomy in Children and Adolescents
Aim: Morbid obesity in children and adolescents is increasing dramatically world wide. Bariatric surgery is presently the most effective treatment to provide with long-term weight loss and increased survival in severely obese. However, the consequences of such surgical interventions on central metabolic pathways, adipokines, and myokines are poorly understood yet. The aim of our study is to unravel the complex network of metabolic changes in obese children undergoing bariatric surgery after 6 month treatment. Our proposal is based on a prospective study of 6 children's with morbid obesity.
Methods: Applying innovative technology of clinical chemistry for metabolome endocrinological analysis, we aim to identify key biomarkers of the underlying pathways and compare the impact of each treatment modality. Here we used a combined proteomic and metabolomic approach to identify previously unrecognized circulating molecules that discriminate the changes of pathways, following sleeve gastrectomy. In our study, 6 males at the age of 9 to15 were involved. We compared serum at basline level with 6 months postsurgery.
Results: We applied a global serum proteomics approach (DIGE) that yielded 135 differentially abundant spots representing 39 different unique proteins. Differential abundance of regulated proteins was confirmed positively by Elisa for antithrombin-III, clusterin, complement C3, pigment epithelium derived factor, retinol binding protein, and vitamin-D binding protein. Targeted serum metabolomics of 163 different metabolites resulted in 4 metabolites that were significantly different in respect to 6 months after sleeve gastrectomy. Among those, glycine, glutamine, and glycero-phospatidylcholine 42:0 (PCaa 42:0) serum concentrations were lower, whereas PCaa 32:1 and PCaa 40:5 were increased after 6 months compared to baseline.
Conclusion: In this study, an integrated serum proteomic and metabolomic profiling enabled detection of parameters that are related to weight loss after bariatric surgery. In the future, this transomics approach enabled detection of parameters and pathways to understood the physiology regulation of weight loss.
Changes in CR3 and FC?R III/II Expression on Peritoneal Macrophage after Laparoscopic and Open Abdominal Surgery in a Mouse Model
Background: The stress response after abdominal operations has been associated with impaired phagocytosis by peritoneal macrophages. Compared with the traditional open abdominal surgery, laparoscopic surgery can result in better preservation of the patient's immunological defenses. This study examined the influence of minimally invasive techniques and open abdominal surgery on postoperative expression of CR3 and FcγR III/II on peritoneal macrophage.
Methods: 8- to 10-week-old BALB/c mice were randomly divided into 3 groups: control animals (C), open surgery (OS), and laparoscopic surgery (LS). Peritoneal macrophages were harvested via intraperitoneal lavage. The following fluorescence-conjugated antibodies were used: PE CR3 (BioLegend), FITC F4/80, PE FcγR III/II, and the relevant isotype controls. The cells were incubated with the antibodies for 30 min at 4°C and washed with PBS. The cells were then analyzed on a FACSort flow cytometer (Beckam-Coulter). Statistical analysis was performed using SAS 8.0 and t test between groups. A P-value of 0.05 was considered significant.
Results: Significant differences were observed between groups. Studying on the MFI of CR3 on peritoneal macrophages, the LS group had a value of 437.40 ± 85.52, which was the same as the C group's 503.17 ± 33.38 (P > 0.05), but was obviously different from the OS group's 292.25 ± 43.88(P < 0.05). However, to the MFI of FcγR III/II on peritoneal macrophages, there is no difference among the C group (43.07 ± 12.01), the LS group (40.72 ± 6.79), and the OS group (51.85 ± 3.75)(P > 0.05).
Conclusion: Open abdominal surgery resulted in greater impaired expression of receptors on peritoneal macrophages than laparoscopic surgery.
Stitch Versus Scar: Evaluation of Laparoscopic Pediatric Inguinal Hernia Repair in a Rabbit Model
Introduction: Laparoscopic repair of pediatric inguinal hernias has been described in great detail in the literature, and numerous techniques have been described. The majority of minimally invasive options rely on the placement of a simple ligating suture. However, when compared with the gold standard open repair, some studies have shown an increased hernia recurrence rate. The purpose of the current study was to evaluate the effectiveness of the ligating stitch in successful hernia repair.
Methods: The male New Zealand white rabbit has a congenital inguinal hernia similar to a patent processus vaginalis seen in infants. Twenty two rabbits weighing 2.7–3.0 kg underwent laparoscopic repair of their inguinal hernia defect. Prior to hernia repair the gubernaculum was ligated with electrocautery to internalize the testicles. The defect was closed utilizing the Subcutaneous Endoscopically Assisted Ligation (SEAL) technique, which involves placing a single ligating suture (2-0 polypropylene suture) around the hernia defect under laparoscopic guidance. Group 1 (6 rabbits) was used to determine the time to healing with simple suture placement. These animals underwent suture repair on both sides and had survival periods of 1, 2, 4, 6, 8, and 12 weeks. Group 2 (16 rabbits) was done to evaluate the role of peritoneal trauma on repair. These animals underwent suture repair on the left, whereas on the right underwent trauma to the peritoneum with laparoscopic scissors prior to suture closure. Group 2 was allowed to survive for 2 or 4 weeks. At the time of necropsy the defects would initially be explored laparoscopically at 4 mmHg pressure. The pneumoperitoneum was released and the suture used for repair was cut and removed. The abdomen was then reinsufflated to 4 mmHg, and under direct visualization, the pressure was increased to 36 mmhg looking for opening of the defect.
Results: Group 1—At all evaluated time points, defects were closed upon initial examination; however, after stitch removal all defects opened at an average pressure of 5 mmHg. As the pneumoperitoneum was increased the defects enlarged nearly returning to original size. Group 2—At 2 week evaluation, only 25% (2/8) of defects repaired with suture alone remained closed after stitch removal, whereas 87.5% (7/8) of defects which had peritoneal trauma remained closed when insufflated to maximum pressure. At 4 weeks the numbers remained similar with 17% (1/6) of defects repaired with suture alone remaining closed and 100% (8/8) of defects repaired with peritoneal trauma remaining closed.
Discussion: Using a rabbit model we have shown that a simple ligating suture alone may not be sufficient for closure of a patent processus vaginalis out to 12 weeks after repair. The addition of sharp trauma to the peritoneum in combination with suture placement may allow for a more permanent repair of the defect.
University Department of Paediatric Surgery, Regensburg, Germany
Aims: Off-patient laparoscopic training is essential in the expanding variety of instruments, procedures, and techniques available to an increasing number of minimally invasive pediatric surgeons and theater staff alike. We presented our Endo-Paed-Trainer at the IPEG-meeting in Phoenix Arizona 2009. In the last few years we designed a programmed systematic training for students and residents to assess their basic skills and monitor their further development in tasks like camera handling or bimanual interaction with a variety of instruments. In addition, sequential short sessions were compared with one long session in our aim to analyze the most effective way of training.
Methods: 34 students and residents with no prior experience in MIS were instructed to perform clearly defined exercises. Every trainee repeated the same exercise 3 to 5 times per session. The first exercise was to use the 30° scope and visualize several defined points of orientation in the abdomen from two sides. In the second exercise the trainees practized the bimanual use of instruments, in this case the dissector and the scissors, to excise and remove objects from the abdomen.
Results: The sequential training group consisted of 11 students and residents, who underwent the 5 day workshop in groups of 3 or 4 trainees doing each exercise three times a day. The long session group included 23 trainees, who took part in a 5 hour workshop in groups of 4–5 and performed both exercises 5 times. The sequential training group completed the first exercise in an average time of 155 seconds the first round and 36 seconds on day five. The long session group had an initial average time of 153 seconds, which was reduced to 55 seconds in the last round. The second exercise was completed by the sequential training group in 350 seconds in the first attempt and could be finally reduced to 124 seconds. The long session group needed 342 seconds the first and 181 seconds in the 5th attempt. The intragroup improvements were 73 and accordingly 65 per cent in the sequential, 64 and accordingly 47 percent in the long session groups. In summary, the sequential training group achieved better improvements in both exercises.
Discussion: The programmed systematic score card training had a very high acceptance by all trainees. It is possible to measure the individual progress in a realistic setting and to compare the own results with the rest of the group, which seemed to be a very strong motivator. We could prove that the sequential training is superior to a single long-term session, altough it may be more difficult to implement it as the regular training. All trainees improved significantly throughout the training. The score card training is also suitable for the testing and implementation of new instruments and methods by advanced MI surgeons.
Endoscopic Surgery in Children's Oncology
Aims: To define performance possibility endoscopic surgery in children's oncology.
Materials and Methods: In Scientific Research Institute of in children's oncology and hematology of N.N. Blohin RAMS endoscopic operations in patients with tumors are regularly performed since 2007. At the present moment the score of performed operations is 249 of which 112 were laparosopic and 106 were thoracoscopic. Operation specter includes biopsies of large formations (92), lung resections (59), nephrectomies (23), adrenectomies (18), kidney resections (1), gastric resections (1), hepatic resections (5), hemihepatectomies (8), retroperitoneal tumorectomies (11), mediastinal tumors (24), operations performed on the organs of minor pelvis (5), appendectomies (1), and splenectomies (1). Operated children aged form 2 months to 18 years (average 8.3 years). Diagnostic operation's average time was 28 minutes. Therapeutic operations took from 30 minutes (in cases of standard adrenectomies) to 280 minutes (hemihepatectomies). Maximal blood loss was 400 ml in cases of hemihepatectomies. Performing endoscopic surgical interventions in children has its specific features: small abdominal cavity volume, lesser sizes of all anatomical structures, and specific features of performing prolonged pneumoperitoneum; it is also impossible to separately intubate selected bronchi when performing thoracoscopic operations in children under 6 years old.
Summary: Advantages of using laparoscopy in children with tumors are earlier possibility of starting specific postoperative treatment, less traumatic operation, minimal blood loss, decreased rate of postoperative complications, earlier recovery of physical activity in operated children, decreased time of staying in the hospital, and better cosmetic effect after surgical intervention.
Conclusion: Performing endoscopic operations in children with malignant tumors is possible from the age of several weeks without breaking the principles of oncological surgery; in such operations the age of the child is not a limiting factor for performing surgical interventions.
Colorectal
Laparoscopic-Assisted Endorectal Soave Pull-Through Procedure for Hirschsprung's Disease: A 10-Year Experience from a Single Institution in China
Purpose: Laparoscopic-assisted endorectal pull-through (LAEPT) was safe and it had a good clinical outcome. The aims of the present study were to describe some technical refinements and evaluate complications and functional results.
Methods: The clinical courses of 218 patients who underwent LAEPT for HSCR were reviewed. LAEPT was described by Georgeson. The main modifications were minimal dissection of pelvic floor, the hepatic or splenic flexure divided before rectosigmoid dissection in patients with long forms, indirect electrocautery during the submucosal dissection, and a “V” incision in posterior muscular sheath. Patient data were collected according to the period of operation-group I, routine LAEPT was used in 80 patients (1999–2002); group II, selective LAEPT was used in 138 patients (2003–2009). The patients were evaluated for age, problems encountered during surgery, complications, and functional outcomes after the operation. Mean follow-up was 68 months.
Results: Patients aged 15 days to 12 years, mean operating times were 127 ± 20 minutes in short forms and 226 ± 35 minutes in long forms. Intraoperative complications were 7.3%. The overall surgical technique related complication rate fell from 12.5% in the group I to 4.3% in the group II (P = 0.026). Early postoperative complications included intestine herniated from trocar site (1.4%), perianal excoriation (9.6%), enterocolitis (2.8%), stricture (4.1%), and anastomotic leak (1.8%). Late postoperative complications included perianal excoriation (5.5%), postoperative adhesive bowel obstruction (1.8%), anal stenosis (2.8%), recurrent constipation (1.4%), and enterocolitis (3.7%). 86% had excellent and good bowel function. Continence showed an increasing trend during growth (P = 0.044) and soiling showed a decreasing trend in patients with HSCR (P = 0.035).
Conclusions: LAEPT is progressively demonstrating its durability in application, with minimal morbidity and satisfactory functional results. A laparoscopic assist before the transanal dissection adds versatility to the pull-through procedure makes the operation simple, and complications such as recurrent constipation less.
Perioperative Outcomes of Laparoscopically Assisted Anorectal Pull through: Rectal Mucosa Prolapse—Is it a Rare Complication?
Background: Laparoscopically assisted anorectal pull through (LAARP) is a recently developed technique for treating high and intermediate anorectal malformations (ARM). This procedure is becoming an established operation for high type anorectal malformations. Since 2000, several articles on LAARP have been published, yet there has not been not much discussion about the complications and perioperative outcomes. The aim of this study is to report on the perioperative outcomes and to discuss the most common complication (rectal mucosa prolapse) after performing LAARP at our center.
Methods: Between 2003 and 2010, we performed 25 LAARPs in patients with intermediate-high type anorectal malformations. We retrospectively analyzed the perioperative outcomes; the patients' ages, the types of anorectal malformation, the associated anomalies, the follow-up duration, the hospital days, the operation times, the postoperative complications, the readmissions, and the reoperations of the patients.
Results: All 25 patients were male. The median age was 2.78 months (range: 0.5–6.2 months). The most common type of anorectal malformation was rectoprostatic urethral fistula (n = 17), followed by rectovesical fistula (n = 3), rectobulbar fistula (n = 3), and recto-bladder neck fistula (n = 2). There were various associated anomalies like gastoschisis (n = 1), duodenal atresia (n = 1), and tracheoesophageal fistula (n = 1); however, spine anomaly (n = 10) were majority. The median length of hospitalization was 8 days (range: 6–42 days), the median operation time was 4 hrs (range: 2.29∼8.20 hrs), and immediate postoperative complications occurred in only 3 patients: urinary tract infection, atelectasis, and ileus, respectively. They recovered after conservative treatment. The median follow-up duration was 27.47 months (range: 2.53–75.70 months). The most common cause of re-admission was prolapsed rectal mucosa (n = 15, 60%); among them, 13 patients received excision of the prolapsed rectal mucosa after 13 months later from LAARP on average, and the next common readmission cause was constipation (n = 7, 28%). All re-admission patients were discharged uneventfully. A urethral diverticulum occurred in one rectobulbar urethral fistula patient.
Conclusion: LAARP was a technically safe procedure for the high-intermediate type ARM. However, rectal mucosa prolapse occurred in more than 50% of the patients after LAARP. Most of them received excision of the prolapsed rectal mucosa. Therefore, further evaluation and effort to find the method that decrease the incidence of rectal mucosa prolapse is needed.
Long-Term Outcomes after Primary Laparoscopic-Assisted Endorectal Pull-Through for Hirschsprung Disease in Infants
Purpose: The laparoscopic-assisted one-stage endorectal pull-through procedure has become the standard treatment for Hirschsprung disease. We evaluated complications, the occurrence of enterocolitis after the operation, and long-term outcomes of fecal continence after a one-staged laparoscopic-assisted endorectal pull-through procedure for Hirschsprung disease in infants.
Materials and Methods: Sixteen infants (10 males, 6 females) found to have Hirschsprung disease, with 3 of them associated with Down syndrome, underwent one-staged laparoscopic-assisted pull-through using transanal endorectal coloanal anastomosis. The procedure was carried out using three 5-mm ports in 15 cases, and four 5-mm ports in a neonate with total colonic aganglionosis. The transition zone was identified by seromuscular biopsies laparoscopically or full-thickness biopsies transanally. The affected colon was laparoscopically mobilized distally beyond the peritoneal reflection, facilitating subsequent perineal dissection, pull-through, and coloanal anastomosis. Transanal endorectal mucosal dissection and a coloanal anastomosis were conducted. The diagnosis of enterocolitis after the operation was based on the clinical presentation of diarrhea, abdominal distension, and fever. All patients were followed up for 3 to 9 years (median: 7 years) after the operation. Evaluations of early and late complications, occurrence of enterocolitis, and long-term outcomes of fecal continence were examining by patients' records.
Results: Eight neonates aged 16 to 30 days and 8 infants aged 1 to 4 months underwent this procedure laparoscopically. The transition zone was identified by seromuscular biopsies laparoscopically in 13 patients, and by full-thickness biopsies using a prolapsed procedure in 3 patients. Ten cases had rectosigmoid aganglionosis, 5 cases long-segment aganglionosis, and 1 case total colonic aganglionosis. Entire colon was excised through the umbilical site in a neonate with total colonic aganglionosis. Other patients had transanal resection of the aganglionic segment. Endorectal mucosal dissection was performed using a prolapsed procedure in 13 patients, and transanally in 3. Early complications occurred in 10 infants. Seven infants showed perineal excoriations in an early postoperative period. A 3-month-old infant associated with Down syndrome underwent a re-pull-through procedure due to ischemia of the pull-through intestine 2 days after the operation. Seven infants had mild anastomotic stenosis and required dilatation with Hegar dilators. An infant with Down syndrome who underwent redo surgery required long-term anal dilatation. Postoperative enterocolitis occurred once within 3 months after the operation in 2 infants with rectosigmoid aganglionosis and an infant with long-segment aganglionosis. An infant with total colonic aganglionosis had 5 episodes of enterocolitis in a period of 5 years after the operation. Enterocolitis of these infants resolved with conservative management. An infant with total colonic aganglionosis and 2 with Down syndrome suffered from intermittent fecal incontinence. The rest of the infants showed satisfactory continence and normal bowel movement. None of the children showed signs of neurogenic bladder dysfunction.
Conclusions: One-stage laparoscopic-assisted transanal endorectal pull-through permits the early diagnosis of the transition zone as well as an adequate mobilization of the bowel for long- type aganglionosis. Enterocolitis occurs at the high rate of 18%; long-term bowel movement and continence, however, are satisfactory in most children after the one-stage laparoscopic-assisted pull-through procedure for Hirschsprung disease.
Outcome Comparison among Laparoscopic, Laparotomic-Duhamel, and Transanal Endorectal Pull-Through: A Single-Center 18-Year Experience
Purpose: Transanal endorectal pull-through has drastically changed the treatment of Hirschsprung's disease (HD) in the past decade. The aim of the study is to compare outcomes, in a single center, obtained with laparotomic Duhamel (LTD), laparoscopic Duhamel (LSD), and laparoscopic assisted transanal endorectal pull-through (LTEPT).
Materials and Methods: We have retrospectively reviewed the charts of all the patients operated on for HD since 1992. Preoperative, operative, and postoperative data were collected to compare short- and long-term outcomes among the three groups of patients operated with different techniques.
Results: From 1992 to 2010, 70 children were treated for HD. Our patients were divided into three groups based on the surgical technique used for the repair: 14 LTEPT, 32 LSD, and 24 LTD. Mean ages at diagnosis were (in months) 4.67, 14.61, and 13.28, respectively. Patients of the LTEPT group had significant shorter operating times (195 vs. 257 vs. 291 minutes, p = 0.03), earlier start of oral feeding (1.2 vs. 3.1 vs. 4.7 days, p < 0.01), and shorter length of hospital stay (4.4 vs. 6.8 vs. 9.7 days, p < 0.011). Complications rate was lower in the LTEPT group (14%) compared with the LSD and LTD (18.7% and 20%). Postoperative enterocolitis episodes, ranging between 6% and 10%, were not different among groups. The mean follow-up period for the LTEPT group was 26 months with no constipation and good continence results for age.
Conclusions: This study further supports the technical advantages, the lighter impact of the surgical procedure on the infants, the decreased incidence of complications, and the better long-term outcome of the transanal pull-through compared to the Duhamel approach.
Laparoscopic-Assisted Restorative Proctocolectomy in Children with Ulcerative Colitis: Is Diverting Ileostomy Necessary?
Purpose: Laparoscopic-assisted restorative proctocolectomy (LAP) with J-pouch ileoanal anastomosis (IPAA) is routinely performed for children with ulcerative colitis (UC). Controversy exists whether this can be done without diverting ileostomy due to risk of early pouch leak and sepsis. Our goal was to compare complications and functional outcomes of children who underwent LAP with IPAA with and without diversion.
Methods: We performed a single-institution retrospective review of UC patients who had LAP with IPAA without diverting ileostomy (−Os) from 2002–2010 compared with a historically matched group of consecutive patients undergoing LAP and IPAA with diversion (+Os) and subsequent takedown. Decision for or against ileostomy was based on surgeon and patient preference. 38 patients were studied (19 +Os, 19 −Os). Demographics, early complications, and functional outcomes were examined. Comparisons were made using the t-test for equality of means.
Results: Preoperative demographics were similar in mean age (14.31yrs −Os vs. 14.21 yrs +Os), serum albumin (3.64 −Os, 3.62 +Os), BMI (20.57 −Os, 21.17 +Os), and immunosuppression use (74% in both groups). Mean total hospital length of stay was significantly less in −Os (12.36 days vs. 17.68, p < 0.05), and the −Os group has less total OR time on average (6:15 vs. 9:56). Each group had one episode of pouch leak, with 5 patients experiencing complications in −Os and 7 in +Os. The −Os group required less pouch dilations in the OR (0.47 vs. 1.79, p < 0.05). Functional outcomes were not significantly different regarding pouchitis occurrences per patient (0.53 −Os, 0.53 +Os), bowel movements per day (5.39 −Os, 7.17 +Os, p = 0.13), and postoperative loperamide dose (9.07 mg qday −Os, 6.29 mg qday +Os, p = 0.09).
Conclusion: LAP with IPAA without diverting ileostomy is a viable treatment option for children with medically refractory UC. Although questions remain about optimal patient selection, quality of life impact, and cost benefits, short- and long-term outcomes can be equivalent to those patients with diverting ileostomy.
Laparoscopic Bowel Resection in Pediatric Coloproctology
Purpose: To analyze our 7-year experience in pediatric laparoscopic coloproctology.
Materials and Methods: The total number of 129 patients underwent laparoscopic procedures with bowel resection for various coloproctologic problems: 106 patients (2 months–17 years) with confirmed diagnosis of Hirschsprung's disease (HD) underwent laparoscopic endorectal pull-through with resection of 25–70 cm of distal and left colon. 6 patients (6–36 months) with high anorectal malformations (ARM) were corrected with laparoscopic technique. There were 4 male patients with high atresia with recto-vesical (2) or recto-prostatic urethra fistulas (2), and 2 females with ARM with recto-vaginal fistulas. In all cases fistula was ligated laparoscopically, the rectum was dissected, resected (bulbous distal part; from 3 to 10 cm), and proctoplasty was performed. 10 patients (10–17 years) with refractory ulcerative colitis underwent:
total laparoscopic proctocolectomy with endorectal pull-through and straight ileo-anal anastomosis (8 patients); laparoscopically assisted restorative total proctocolectomy with pouch-anal anastomosis was performed in 2 patients (1, lateral pouch; 1, J-pouch).
Three patients (males, 12, 13, and 15 years old) with medically refractive Crohn disease and ileocecal stricture underwent laparoscopic ileocecal resection (from 20 to 45 cm) with intracorporeal stapled ileo-colonic anastomoisis; 2 girls (12 and 14 years old) with clinically and radiologically confirmed Payr's disease, chronic colostasis in the transverse colon, presence of painful syndrome, progressive increase of symptoms, and absence of effect from conservative therapy were also treated laparoscopically. Totally, laparoscopic resection of the transverse colon (about 30 cm) with stapled anastomosis, dissection, and bringing down of a lienal flexure was performed. Right hemicolectomy was made in 2 male patients (9 and 13 years old) with similar history and clinical situation. Both patients underwent multiple open procedures for complicated appendicular peritonitis (6 previous operations in one case, 8–in the other) with ileo-transversal anastomosis at the end of the treatment. The presence of large and inflamed blind bowel suck (right hemicolon) with acute clinical symptoms (pain, intoxication, and painful mass in the abdominal cavity) was the indication for laparoscopic right hemicolectomy with resection of 30–35 cm of inflamed bowel.
Results: There were no cases of conversion in the described group of 129 patients.
Complications:
HD (106 patients):
mild stricture treated with dilatation—5 patients (4.7%); serious stricture treated with repeated laparoscopic pull-through—1 (0.9%); rectovaginal fistula (treated with colostomy for 6 months) —1 (0.9%); episodes of mild enterocolitis—6 (5.7%) mild degree of fecal incontinence—13 (12.3%); mild degree of constipation—5 (4.7%).
Ulcerative colitis (10 patients): acute pouchitis—1 patient with J-ileoanal pouch. Laparoscoipic pouch excision with straight endorectal ileoanal abastomosis was performed 8 months after the primary procedure.
Conclusion: Laparoscopy provides excellent conditions for minimally invasive bowel surgery in pediatric coloproctology. All necessary variants of bowel resection (ileocecal, right hemicolectomy, transverse colon, left colon, total proctocolectomy, etc.) with various types of anastomosis or pull-through can be effectively performed laparoscopically; laparoscopic bowel surgery is associated with good functional outcomes, excellent cosmetic results, and acceptably low complications rate.
Laparoscopic-Assisted Rectal Pull-Through for Persistent CLOACA
Aim: To describe the surgical technique and initial outcomes of laparoscopic-assisted anorectal pull through for persistent cloaca.
Materials and Methods: From January 2008 to June 2010, laparoscopic-assisted rectal pull through was performed for 10 patients with cloaca. The patient ages ranged from 4 to 9 months. The operation was carried out using 4 trocars. CO2 pressure was maintained between 8–10 mmHg.
Results: Laparoscopic-assisted rectal pull-through was successfully performed in all patients. Operative time ranged from 90 to 120 minutes (mean, 110 minutes). There were no intra- and postoperative deaths or complications. The mean hospital stay was 4.4 days (range 4–5 days). Follow-up from 1 to 18 months was obtained in 9 patients. Number of stools ranged from 1 to 4 times/day.
Conclusion: Laparoscopic-assisted rectal pull-through is a feasible and safe procedure for persistent cloaca.
Laparoscopic Treatment of CLOACAS
Background: The traditional surgical treatment of cloacas has been modified by the advent of laparoscopy, which allows the intrabdominal and deep pelvic procedures without laparotomy. Laparoscopic surgery has the advantage of being minimally invasive, providing much less perineal trauma to the structures that are essential for continence, but some improvements in technique are only now being developed. The aim is to show examples of video-assisted techniques for correction of cloacas showing tricks and strategies for fast and safe operations using 3 trocars, also demonstrating the mobilization of the urogenital sinus (UGS) more easily than in open surgery and a limited sagittal perineotomy.
Materials and Methods: 6 girls with cloacas had common channels ranging from 2 to 4 cm. All underwent preoperative endourological study to define the anatomy and surgical planning. We used 3 trocars and transparietal stiches allowed bladder and sigmoid traction, facilitating retrovesical exposure. The 30-degree view of the scope allowed adequate visualization and detailed dissection of the deep pelvic spaces. Following the release of the rectum and of the UGS, we identified the striated muscle complex, and performed the incision in the perineum for the anoplasty, guided by electrical stimulation. The rectal fistula was sectioned and ligated with Vicryl®. Different types of vagina required vaginoplasty. One girl with vesico-ureteral reflux had the Gregoire reimplantation done before the rectal pullthrough. A transperineal tunnel was made up by a 5-mm trocar following the vertical fibers of the complex into the dissected cavity. The rectum was pulled down for anoplasty, completing the laparoscopic time. The mobilization of the distal UGS was performed through a midline incision at the anterior perineum. Since the deep segment of the UGS had already been released from the inside, the perineal mobilization was quick and easy. The vaginoplasty and urethroplasty did not require wide opening of the striated sphincteric complex.
Results: All the girls have been operated on without complications. They were discharged after 2–4 days. After follow-up periods from 6 m to 4 years, five have urinary continence and one is incontinent. Three have presented good fecal continence, two are incontinent, and one (2 years old) with satisfactory degree of continence for age.
Conclusions: The laparoscopic is feasible and very effective in treating cloacas, facilitates UGS mobilization, and requires very limited perineal incision; however, a larger sample and longer follow-up time are needed to analyze functional results compared to Peña's procedure.
Cool Tricks
A Retrospective Review of Gastroscopy-Assisted Closure of Pyriform Sinus Fistula in 57 Children
Objective: To evaluate the effect of gastroscopic assistant operation for children with pyriform sinus fistula.
Methods: The clinical data of 57 patients (male 38 and female 19) aged from 2.5 to 9 years with pyriform sinus fistula were retrospectively analyzed. Recurrent infections after fistulectomy or cystectomy were noted in 37 patients. The other 20 patients presented with twice or more episodes of infection. The diagnosis was identified by esphagogram, CT, ultrasonography, and scintigraphy. All 57 patients underwent gastroscopic assistant fistulectomy. Eight patients heretofore underwent fistulectomy regarded as control group.
Results: In gastroscopic assistant operation group, the mean operation time was 1 h 35 min. All patients did well postoperatively and shown no recurrences during follow-up term. In control group, the mean operation time was longer; recurrent infection had been noted in three patients.
Conclusions: Gastroscopic assistant operation is a simple, quick, and effective operation for children with pyriform sinus fistula.
Gastrointestinal & Hepatobiliary
The Experimental Studies and Clinical Applications of Laparoscopic Duodenal Single-Layer Sutured Anastomosis in Infants
Objective: To explore the reliable methods of a laparoscopic single-layer duodenal sutured anastomosis through animal experiments and utilize the clinical works.
Methods
Animal experiment: Ten rabbits were pretended to simulate the abdominal environment of newborn and infant. They were randomly divided into the continuous suture group and the interrupted suture group to carry out the single-layer diamond-shaped anastomosis in the duodenum.
Clinical application: A single-layer full-thickness sutured anastomosis was applied in 12 infants with congenital duodenal obstruction. Under the laparoscopic visualization, the cause of duodenal obstruction was explored and a single-layer diamond-shaped sutured anastomosis was performed.
Results
Animal experiment: All laparoscopic single-layer diamond-shaped anastomoses of the duodenum were successfully performed in 10 rabbits. The anastomotic time was 38.8 ± 5.07 min in the interrupted suture group and 27.0 ± 7.25 min in the continuous suture group, the continuous suture time took shorter than the interrupted suture time (t = 2.984, p = 0.017, p < 0.05). The laparotomy after laparoscopic procedure in two groups of rabbits showed good patency of the anastomosis and no intestinal leakage. The tolerant pressure of the anastomosis was 72.4 ± 19.50 cm H2O in the interrupted suture group and 90.8 ± 6.38 cm H2O in the continuous suture group. The significant difference was not found between the two groups (t = 2.00, p = 0.08, p > 0.05). However, there was a rabbit that the pressure could only meintain 48 cm H2O due to interrupted anastomotic mucosal eversion.
Clinical application: The etiology of 12 infants was laparoscopically identified and all procedures were successfully performed. Six cases with duodenal diaphragmatic stenosis were encountered a partial excision of the diaphragm after vertical incision of the anterior part in the duodenum followed by a transverse suture. A diamond-shaped full-thickness duodenoduodenal anastomosis was completed in 4 cases with duodenal atresia and 2 annular pancreas. The operative time was 60–150 min. There was no intraoperative complications and blood transfusion. Except 1 neonate with transient anastomotic leak was cured by draining for 3 days (from day 2 to 4 postoperatively) without another intervention. All children were cured and the postoperative period of hospital stay was 7 to 12 days.
Conclusion: The hand-sewn single-layer anastomosis is carried out that it avoids mucosal eversion. If the mucosal eversion occured, the anastomotic tolerant pressure would decrease significantly and prone to anastomotic leakage. The single-layer interrupted and continuous suture anastomosis could achieve satisfactory effect, but the continuous suture is more convenient and time-saving compared with the interrupted suture under the laparoscope.
Early and Intermediate Outcomes of Laparoscopic Cystectomy and Hepaticoduodenostomy Versus Roux-EN-Y Hepaticojejunostomy for Choledochal Cyst in Children: A Randomized Clinical Trial
Objective: To compare the early and intermediate outcomes of laparoscopic cystectomy and hepaticoduodenostomy versus Roux-en-Y hepaticojejunostomy for choledochal cyst in children.
Methods: An open randomized clinical trial was developed and a research protocol approved by the hospital ethics committee. Written consent was obtained from patient's parents. Patients with choledochal cysts admitted to National Hospital of Pediatrics of Hanoi, Vietnam, from December 2007 to August 2010 were enrolled in the study. The patients were randomized to undergo laparoscopic cystectomy and hepaticoduodenostomy or Roux-en-Y hepaticojejunostomy. The main outcome measures included operative time, rate of postoperative biliary leakage, bleeding, hospital stay, cholangitis, duodenal ulcer, and anastomotic stenosis.
Results: There were 242 patients. 121 patients underwent hepaticoduodenostomy and 121 patients underwent Roux-en-Y hepaticojejunostomy. There was no significant difference between the two groups in regard to the patient's age, gender, and the diameter of the choledochal cyst. The mean operative time in hepaticoduodenostomy group was 151 ± 3 minutes, whereas it was 213 ± 5 minutes in Roux-en-Y hepaticojejunostomy group. The difference was significant (p < 0.01). Four patients in the hepaticoduodenostomy group and two patients in the Roux-en-Y hepaticojejunostomy group had biliary leakage. The difference was not significant. Postoperative hospital stay was 6.2 ± 0.3 days in the hepaticoduodenostomy group and was 7.0 ± 0.4 in the Roux-en-Y hepaticojejunostomy group. The difference was not significant. Follow-up from 1 month to 38 months was obtained in 81 patients of the hepaticoduodenostomy group and 82 patients in the Roux-en-Y hepaticojejunostomy group. Cholangitis was reported for one patient in the hepaticoduodenostomy group and one patient in the Roux-en-Y hepaticojejunostomy group. One patient in the hepaticoduodenostomy group suffered from anastomotic stenosis and one patient in the Roux-en-Y hepaticojejunostomy group suffered from duodenal bleeding due to duodenal ulcer. The difference of cholangitis, anastomotic stenosis, and duodenal bleeding was not significant between the two groups.
Conclusion: There were no significant difference in early and intermediate outcomes of laparoscopic cystectomy and hepaticoduodenostomy versus Roux-en-Y hepaticojejunostomy in the management of choledochal cyst in children. However, the operative time was significantly shorter in the hepaticoduodenostomy group.
Middle-Term follow-up Results on Laparoscopic Versus Open Roux-Y Hepatojejunostomy for Children with Choledochal Cysts
Aim: Laparoscopic hepatojejunostomy (LH) for children with choledochal cysts (CDC) has recently been gaining popularity. However, its safety and efficacy remain unknown. The current study is to evaluate the middle-term results of laparoscopic hepatojejunostomy (LH) for children with choledochal cysts (CDC).
Methods: We reviewed 218 patients who underwent LH between October 2001 and October 2009 and 200 patients who underwent open hepatojejunostomy (OH) between September 1993 and September 2001. Ultrasonography, upper gastrointestinal contrast studies, and laboratory tests were performed during the follow-up period. Age, operative blood loss, operative time, postoperative hospital stay, time to full feed, duration of drainage, postoperative complications, and perioperative laboratory tests were evaluated in both groups.
Results: Median follow-up periods of LH and OH groups were 38 and 146 months, respectively. There was no significant difference in age between 2 groups. Interestingly, the operative time of LH group decreased significantly with increasing number of cases (p < 0.01). The most recent result did not differ from that of OH group (3.04 hrs vs. 2.95 hrs, p = 0.557). The operative blood loss of LH group was significantly less (p < 0.001). The postoperative hospital stay, resumption of alimentation, and duration of drainage in LH group were significantly shorter (p < 0.001, respectively). Two out of 218 (0.9%) LH patients developed bile leak. This was significantly less than 11/200 (5.5%) in OH group (p < 0.01). The morbidities of LH group were significantly lower than those of OH group. Postoperative liver function tests and serum amylase levels normalized in both groups (p < 0.001).
Conclusion: Laparoscopic hepatojejunostomy is safe and effective. Its middle-term results are comparable to or better than open surgery.
Is the Laparoscopic Operation as Safe as Open Operation for Choledochal Cyst in Children?
Aim: To compare the safety of laparoscopic operation with open surgery for choledochal cyst in children.
Methods: Early outcomes of open surgery from January 2001 to December 2006 were compared with early outcomes of laparoscopic operations from January 2007 to July 2010. The main outcome variables included intra- and early postoperative complications, operative time, rate of reintervention, and duration of postoperative stay.
Results: There were 307 patients in the open operation group and 307 patients in the laparoscopic operation group. There was no significant difference in cyst diameter between the two groups. The operative time was longer in the laparoscopic operation group. Number of patients requiring blood transfusion was lower in the laparoscopic operation group. Intraoperative complications were low in both groups and not significantly different. The rate of postoperative complications was lower in the laparoscopic operation group but not significantly. The rate of reintervention was significantly lower in the laparoscopic operation group. The postoperative stay was significantly shorter in the laparoscopic operation group.
Conclusion: Laparoscopic operation is as safe as open operation for choledochal cyst. The postoperative stay was significantly shorter in the laparoscopic operation group.
Laparoscopic Versus Conventional Kasai Portoenterostomy in Infants with Biliary Atresia: A Prospective Trial
Background Data: Studies on laparoscopic versus conventional Kasai portoenterostomy focus on short-term results, include small numbers of patients, and have design limitations. Therefore, the long-term outcome after laparoscopic Kasai procedure remains to be established.
Methods: Laparoscopic Kasai procedure was performed in a consecutive series of children from 2006 to 2007. Conventionally operated control patients consisted of a consecutive series of infants with biliary atresia operated from August 2003 to 2006. All data were ascertained prospectively using the European Biliary Atresia Registry/EBAR registration forms. Primary outcome measure was survival with own liver 6 months after Kasai without being listed for liver transplantation. An interim analysis was planned after data became available for the first 12 patients, who underwent the laparoscopic Kasai procedure. In case of a significantly different interim outcome, the follow-up period should be extended to 24 months until a final decision can be made.
Results: Laparoscopic Kasai procedure was performed in 12 children without conversion or revision and there was no revision in the control group of 28 conventionally operated patients. Six months after operation, 5 out of 12 laparoscopically operated patients (42%) survived with own liver, compared to 23 out of 28 (82%) controls (p < 0.001). The study was stopped due to the significantly higher rate of liver transplantation after laparoscopic operation. Ten patients (83%) after laparoscopic Kasai versus 18 (64%) conventionally operated patients were transplanted after 24 months (p < 0.05) and survival rates with own liver and serum bilirubin <20 μmol/l were 1 (8%) versus 8 (29%), respectively (p < 0.05).
Conclusions: Laparoscopic Kasai procedure for biliary atresia is technically feasible. The study was stopped after inclusion of 12 laparoscopically operated infants due to a lower survival with the native liver after laparoscopic versus conventional Kasai operation. Superior results after conventional operation were confirmed at follow-up after 24 months.
Choledocholithiasis: Management and Treatment—Experience in a Pediatric Hospital
Introduction: Laparoscopic cholecystectomy (LC) is the treatment of choice for cholelithiasis. However there is still controversy about the sequence of treatment in pediatric patients with choledocholithiasis: for example, intraoperative cholangiography (IOC) versus preoperative endoscopic retrograde cholangiopancreatography (ERCP).
Materials and Methods: When doing an LC, selective IOC is our choice in patients with clinical history and or laboratory values compatible with biliary tree obstruction, pancreatitis, or ultrasound findings of a dilated common bile duct (CBD) or stones in it. During the last year preoperative ERCP was introduced on a selective basis when suspecting impacted stones in the distal CBD. We make a restrospective review of 95 patients out of 531who underwent an LC that required IOC between November 1995 and June 2010. Clinical, ultrasound, and laboratory preoperative data and intraoperative findings were analyzed.
Results: 27 (28.4%) were boys and 68 (71.5%) girls. Their mean age was 14.6 years (range 5 to 17 years). In 74 (77.9%) the IOC was negative for stones in the CBD. 17 (17.9%) patients required instrumentation of the CBD to remove the stones. They were successfully removed laparoscopically in 7, one of which required an ERCP 2 months later for residual microlithiasis. Aditional procedures were necessary in the other 10:7 were converted to open surgery and a laparoscopic transcystic catheter was left in 3 who underwent a postoperative ERCP to remove all stones. The 7 patients who inderwent open surgery were adolescents with an impacted stone in the distal CBD. The following 4 patients with suspected impacted stones underwent a preoperative ERCP and papilotomy followed by a laparoscopic cholecystectomy
Conclusions
17.9% (95/531) of patients with cholelithiasis had preoperative suspected choledocholithiasis. Only 3.9% (21/531) probed to have it at the time of CL or in preoperative ERCP. An initial laparoscopic IOC showed that 81.3%% of the patients with clinical, laboratory, or ultrasound findings suggesting choledocholithiasis did not require instrumentation of CBD or an ERCP. A preoperative ERCP and papilotomy in these group of patients would have been unnecessary. On the hand, it would be the best option for adolescents with evidence of impacted stones in the distal CBD, preventing convertion to open surgery.
Laparoscopic Liver Resection for Treatment of Liver Tumors in Children
Malignant tumors have recently become the second cause of children death all over the world. However, the application of laparoscopic methods in children with liver tumors is usually limited to biopsies and cysts deletion. We used minimally invasive techniques to perform separate stages of hemihepatectomy in adults passing to full scale liver surgeries. In 2008 we started applying that experience in children oncology. From July 2007 to September 2009 we performed 8 laparoscopic bisegmentectomies II and III; 2 laparoscopic bisegmentectomy IV and V; and 5 laparoscopic right-side hemihepatectomies in children. We used balanced multicomponent endotracheal anesthesia combined with epidural analgesia. When performimg the right-side hemihepatectomy, we used the endoscopic tool LigaSure. It allows to control hemostasis when cutting short hepatic veins, performing the phased dissection of liver parenchyma, and cutting the branches of portal vein in the liver parenchyma. Using the stapler ENDO GIA 30 the right liver vein was sealed and cut. The resected liver fragment was placed into a container and evacuated through the section in right iliac zone. The liver surface was covered by the absorbable hemostat Surgicel. Right-side hemihepatectomies lasted from 150 to 240 minutes, the blood loss was 150–400 ml. Liver resection and bisegmentectomy lasted 90–120 minutes with the blood loss of 60–80 ml. Postoperational anesthesia was secured by constant epidural infusion of 1% ledocain. The quantity of the fluid removed by the drainage did not exceed 80 ml. The drainage tubes were removed on the 2nd or 3rd day. The patients were activated on the 1st or 3rd day. The results of the surgeries provide the conclusion that large-scale video-assisted surgical procedures in children with liver tumors have far-reaching prospects in the institutions practicing open surgeries on the liver.
Laparoscopic Versus Open Repair of Congenital Duodenal Obstruction in Infants
Background/Purpose: Congenital duodenal obstruction (CDO) is traditionally managed via laparotomy. Laparoscopy has been suggested as an alternative; however, only a few series have described this in neonatal CDO. We report our series of CDO repaired laparoscopically compared to laparotomy.
Methods: From October 2001 to July 2010, 58 patients presented to our medical center with CDO. During the period, duodenal obstruction was explored either laparoscopically (LAP) or via a traditional open approach (OPEN) based on the surgeon's choice. Patients requiring conversion from laparoscopy to laparotomy were included in the laparoscopic group. Data were analyzed based on intention to treat and are expressed as median ± range. The Children's Healthcare of Atlanta Institutional Review Board approved this retrospective chart review.
Results: Twenty-two neonates underwent laparoscopy and 36 had a traditional laparotomy for management of duodenal obstruction. Associated diseases for all comers included Down's Syndrome (n = 26), congenital heart disease (n = 29), malrotation (n = 16), other (n = 8). Median age was 4 days with a range of 1–310 days for LAP and 3 days with a range of 0–166 days for OPEN (p = 0.04). The 2 children who presented at 310 and 166 days were found to have a partially obstructing duodenal web on a work up for failure to thrive. There was no statistically significant difference in gestational age or weight (p = 0.335 and 0.378). The CDO was due to atresia (n = 32), web (n = 16), and annular pancreas (n = 10). Median operative time for LAP was 116 minutes with a range of 73–164, whereas median time for OPEN was 103 minutes with a range of 71–220 (p = 0.013). There was no difference in time to full feedings (p = 0.69) or postoperative length of stay (p = 0.682). Number of days of IV narcotic usage approached statistical significance (p = 0.079). Ventilation time was 2 days with a range of 0–149 for LAP and ventilation time was 4 days with a range of 0–9 for OPEN (p = 0.02). Complication rates between the groups were similar.
Conclusion: In the hands of a skilled surgeon, laparoscopy appears to be a safe and effective technique in managing CDO in neonates. In this retrospective study, laparoscopic management of CDO appeared to allow a lower narcotic pain medication requirement and shorter postoperative ventilator requirement with similar length of stay and time to full feedings. Operative time was slightly longer in the LAP group. Formal prospective trials are recommended to validate these findings.
Utility of Laparoscopic Nissen Fundoplication in the Control of Pulmonary Hypertension Secondary to Gastroesophageal Reflux
Introduction: Although gastroesophageal reflux is a physiological event in almost all infants and babies, some cases have symptoms that are severe and life threatening. The reflux may cause airway obstruction and other problems such as hypoxia and hypercapnia. These events produce vasoconstriction of the pulmonary vessels, with elevated pulmonary artery pressure. Information about the relationship between gastroesophageal reflux and pulmonary hypertension is very scarce and only one report of a case has been found. In this study we measured pulmonary systolic pressure in patients with severe gastroesophageal reflux who underwent laparoscopic Nissen Fundoplication in the pre-and postoperative period to assess the usefulness of the procedure.
Methods: In a prospective study of 2006–2010, we selected patients with severe gastroesophageal reflux associated with cyanosis, almost sudden death, and severe pneumonia, in which gastroesophageal reflux was demonstrated by clinical, radiological, and pH diagnostics. All of the patients had their systolic pulmonary pressure measured by echocardiography before the surgery, as well as a week, month, and 6 months on a postoperative basis. The preoperative oxygen saturation and its response to oxygen administration were also measured. Fundoplication under laparoscopic Nissen technique was performed. We evaluated any remission of symptoms and complications. Patients with severe heart disease that conditioned pulmonary hypertension were excluded.
Results: 48 patients were treated; mean age was of 86.66 days, average weight of 4.99 kg. 22 presented cyanosis and apnea, and 26 with severe pneumonia. The barium study showed reflux without any other anatomical abnormality. Lipid-laden alveolar macrophage was positive in 26 patients. The pHmeter measurement was positive in 16 patients. Mean preoperative pulmonary pressure was 64.29 mmHg (normal 25 mmHg). The mean average pressure a week after surgery decreased to 30.3 mmHg (P < 0.01), 1 month after to 25.95 mmHg (P < 0.01), and 6 months into the postoperative period to 23.08 mmHg. (P < 0.01). The average oxygen saturation before surgery was 75.33%; all recovered with the administration of oxygen. 12 patients were oxygen dependent preoperatively and 1 month after operation none of them required oxygen. 4 patients were operated when they underwent mechanical ventilation and administration of nitric oxide at 72 hours of postoperative ventilatory support was removed. In all the symptoms disappeared, there were no complications or conversions.
Conclusions: This study showed that gastroesophageal reflux disease with cyanosis or pneumonia in patients 6 months and younger produces severe pulmonary hypertension. The normalization of pulmonary pressure in this group of patients after laparoscopic Nissen Fundoplication demonstrates the utility of the procedure in pulmonary hypertension due to gastroesophageal reflux. The pulmonary pressure measurement is an useful and objective method for evaluating the effectiveness of antireflux surgical treatment.
Long-Term Outcome of Laparoscopic Nissen Procedure in Pediatric Patients with Gerd Mesured using the Modified QPSG Roma III Espghan's Questionnaire
Background/Purpose: Laparoscopic fundoplication (LF) represents the gold standard for surgical treatment for pediatric patients with gastroesophageal reflux disease (GERD).
Methods: We report the results of long-term outcome of 36 patients who had undergone LF from January to December 1998, with a follow-up of at least 10 years. The patients were telephonically invited to undergo a clinical follow-up. All patients underwent the modified ESPGHAN's Roma III questionnaire; however, only 22/36 patients accepted to be controlled in a day hospital setting, 10/36 accepted to underwent telephonic questionaire. Our study is focused on the data of these 32 patients.
Results: 28/32 (87.5%) patients had completely recovered; 4/32 patients (12.5%) had a mild persistent GER; 9/32 patients (28%) referred a mild dysphagia; 21/32 (66%) patients can burp and only 9/32 (28%) can vomit. The cosmetic result was good in 30/32 (94%) patients. The weight/height ratio was satisfactory in 28/32 (87.5%) patients. The quality of life is good in 28/32 (87.5%).
Conclusions: Our experience shows that the long-term follow-up after LF produces a good clinical result and a good quality of life. The modified ESPGHAN's Roma III questionnaire seems an effective way to check the long-term results, because it avoids submitting patients to long and not well-tolerated instrumental exams.
Role of Mininvasive Intraoperative Enteroscopy in Neonates
Introduction: Mini Intra-Operative Enteroscopy (MIOE) is accepted as the ultimate diagnostic procedure for complete evaluation of small bowel disease in infants. MIOE has been used for small intestine polyposis and occult intestinal bleeding. The availability of capsule endoscopy has considerably reduced the indications for MIOE, but this technique is still useful to diagnose rare disease that affect intestinal wall in small babies.
Material and Methods: Two patients were submitted to MIOE because of clinical signs of intestinal obstruction and enteral bleeding. Case 1: male, admitted in emergency at 15 days of life for severe sepsis, developing persisting signs of intestinal bleeding and sub-occlusion. Diagnostic laparoscopy showed augmented thickness of the wall involving most part of the small bowel. Concomitant endoscopic evaluation revealed presence of ulcerative disease in stomach, duodenum, and upper jejuneum. The patient was treated with steroids and cyclosporine without complete remission, so MIOE with biopsies permitted to define the diagnosis of persistent vasculitis of the distal ileum, which was successfully treated with limited bowel resection. Case 2: female, admitted at 4 months of age for intestinal obstruction and enteral bleeding. MIOE carried out through umbilical access performed for a diagnostic laparoscopy, allowed the identification of intestinal ulcers leading to the diagnosis of jejunal eosinophilic enteritis. The patient was successfully treated with steroid and cyclosporine and segmental resection.
Discussions and Conclusions: In both cases MIOE permitted to obtain an unusual diagnosis that was not exhaustive with conventional imaging and upper tract endoscopic biopsies. The small size of the patients limited the use of endoscopic capsule and ileoscopy. The combination of diagnostic laparoscopy and MIOE was essential for a complete view of the whole intestine and allowed limited transombelical exposure of the affected bowel. MOIE defined localization, extension, and characteristics of the lesions that were essential for a correct diagnosis and treatment.
Cardiaplication: A Novel Surgical Technique for Refractory Gastroesophageal Reflux in the Pediatric Population
Introduction: Thousands of infants with medically refractory reflux are referred to pediatric surgeons annually. Traditional surgical intervention, the fundoplication, aims at tightening the lower esophageal sphincter (LES) while altering the Angle of His. Over the past year, we have encountered several infants with refractory gastric reflux and anatomic limitations that precluded classic fundoplication. Here, we report the use of an innovative technique, cardiaplication, as an approach for antireflux surgery. This new technique was designed to tighten the LES and elongate the intrabdominal esophagus without disrupting the esophageal hiatus.
Methods: Three infants with medically refractory gastroesophageal reflux disease (GERD) were referred for fundoplication. In each case, the patient's anatomy prevented a traditional fundoplication from being performed. A cardiaplication was performed by invaginating the cardia of the stomach at the Angle of His and securing the invaginated tissue with interrupted silk suture. This was performed over a 14-French suction catheter to prevent excessive tightening of the LES. The plication elongated the intrabdominal portion of the esophagus thereby altering the Angle of His. This created a flapper valve over the distal esophagus further limiting potential reflux. The charts for the infants who received cardiaplication were reviewed. Radiographic studies and clinical notes for the presence of persistent reflux were evaluated.
Results: Three infants with abdominal situs inversus were referred for fundoplication and G-tube placement for management of medically refractory GERD. Each patient had a diagnosis of congenital heart disease and heterotaxy. Two of the babies had undergone prior laparoscopic Ladd's procedure, whereas one underwent a Ladd's procedure concomitantly. Pre-operative imaging (upper-GI) was performed in all 3 patients and confirmed malrotation and significant esophageal reflux. All 3 patients received a cardiaplication and 2 of the 3 had closure of a hiatal hernia. All cases were initiated laparoscopically and one was converted to an open procedure secondary to dense adhesive disease. Each child was initiated on feeds between post-op day 2 and 3. Two of the three patients were tolerating goal feeds within 2 days of starting enteric feeds. The third patient reached goal feeds on day 16. Post-op imaging (upper-GI) was obtained in 2 of the 3 patients. One patient had radiographic evidence of reflux and one showed no reflux. At follow-up (5 weeks, 8 weeks, and 7 months), all 3 patients are clinically symptom free.
Conclusion: To our knowledge, cardiaplication is not described elsewhere in the literature. Based on preliminary findings, this appears to be a valid surgical technique for the management of severe GERD in infants. We performed cardiaplication out of necessity. However, we are hopeful that this will be an alternative surgical approach for GERD in infants, as this can be performed without disruption of the hiatus. Although long-term follow-up is not currently available, the children who had a cardiaplication all were found to have satisfactory resolution of their clinical reflux postoperatively. We are currently working to develop animal models to test this method under a controlled setting, and anticipate a prospective, randomized trial in humans in the near future.
Laparoscopic Repair of Congenital Duodenal Stenosis in a Pediatric Reference Center in Peru
Background: Laparoscopic repair of Congenital Duodenal Obstruction (CDO) has been recently described with good results. However, there still exist few series describing this procedure.
Methods: A retrospective analysis of all patients undergoing repair of CDO from January 2009 to August 2010 was achieved. Open and laparoscopic approach was performed. Three-port technique for laparoscopy was used, with intrabdominal pressure 8–10 mmHg and a duodenoduodenostomy with PDS 5/0 was made, with intracorporeal knots.
Results: Sixteen patients underwent repair of CDO. Seven patients had duodenal atresia type I and 9 patients had duodenal stenosis (7 with diaphragm and 2 anullar pancreas). Five cases of duodenal stenosis were treated by laparoscopy. Age varied from 23, 62, and 68 days old, 2 years 2 months, and 2 years 7 months old at operation. A female predominance (3:2) was found. All the patients had Down Syndrome, 4 of them had congenital heart disease, and 1 with anorectal anomaly. Location of the stenosis was at the 2nd portion in 4 cases and at the third portion of duodenum in one of them. There was one duodenal anastomotic leak in the older patient who needed a second open repair. Operative times were similar (average 175 minutes). The length of postoperative hospitalization (average 9 in the first 4 cases and 23 days in the complicated case), time to initial feeding after succesfull laparoscopy was 6 days. Minimal scar with excellent cosmetic results were obtained at 1 and 3 months after surgery.
Conclusion: Good functional and cosmetic results has been achieved by laparoscopic repair of CDO. However, longer series or multi- institutional reviews are needed to know the real benefits of this approach.
Primary Laparoscopic-Assisted Endorectal Pull-Through for Hirschsprung's Disease: 5-Year Outcome Data for a National Cohort of 28 Cases
Introduction: There is a lack of reported medium to long-term outcome data for primary laparoscopic-assisted endorectal pull-through (LAERPT). We report outcomes in a national cohort of patients with 5-year follow-up from two pediatric surgical centers in Scotland that perform primary LAERPT, utilizing similar operative techniques and follow-up.
Methods: Cases were identified from prospectively recorded theatre and neonatal databases. Data including complications, unplanned readmissions, enterocolitis rates, and bowel function were extracted from case-notes using a structured proforma. Retrospective assessment of bowel function was performed based on frequency of stooling, requirement for laxatives or washouts, and need for manual evacuations or ACE procedure. Patients with less than 5-year follow-up were excluded from analysis.
Results: 61 patients underwent primary LAERPT in Scotland between 1998 and 2009. 28 patients have been followed-up for at least 5 years after definitive surgery and they form the basis of this study. Median age at diagnosis was 11.5 days (range 2–826 days) and median weight at surgery was 5.53 kg (range 3.12 kg-13 kg). Intra-operative frozen section analysis of laparoscopic biopsies demonstrated rectosigmoid transition zone in 27 patients and descending colon in 1 patient. Colonic mobilization was performed laparoscopically in 20 cases; by transanal mobiliaation following laparoscopic biopsies in 7 cases; and by combined laparoscopic and transanal mobilization in 1 case. Intraoperative complications were uncommon. In two patients, the posterior urethra was injured during endorectal dissection, with both closed primarily with no long-term sequelae. 3 patients underwent conversion to open procedures due to difficult laparoscopic mobilisation. There were no anastomotic leaks or wound infections. Median time to discharge was 6 days (range 6–33 days). Postoperatively, 16 patients underwent a course of anal dilatations and 1 patient required stricturoplasty for an anastomotic stricture. Overall, 19 (68%) patients had unplanned readmissions, with a median number of unplanned readmissions of 4 (range 1–19). 13 (46%) patients required admission for suspected enterocolitis and 2 of these required temporary defunctioning colostomy. 1 patient required redo pull-through for an aganglionic proximal resection margin. There was no late mortality. Stool frequency 5 years after surgery ranged between one stool every 3 days to 2 stools per day. An objective assessment of bowel function based on requirement for laxatives, washouts, or enemas was available for 25 patients. 16 patients had normal bowel habit without medication. 4 patients required laxatives or stool softeners alone; 2 patients required laxatives and washouts or enemas; and 2 patients required washouts or enemas alone to maintain a normal stool frequency. 1 patient was on anti-diarrhoeal medication.
Conclusion: These results demonstrate acceptable medium-term outcome in terms of bowel function and complications although they highlight a significant rate of suspected postoperative enterocolitis and unplanned readmissions in the first 5 years after surgery. Previous reports suggest that retrospective studies underestimate the frequency of complications such as soiling and constipation. Although we limited our analysis of bowel function to objective assessment of need for medications or washouts, we plan to perform a questionnaire-based assessment of bowel function, including soiling, incontinence, and overall quality of life 10 years after surgery.
Miscellaneous
Laser Ablation of Placental Vessels in Twin-to-Twin Transfusion Syndrome: A Paradigm for Endoscopic Fetal Surgery
Background: Endoscopic fetal surgery is most commonly used for the treatment of twin-to-twin transfusion syndrome (TTTS), but the surgical techniques can be applied to other forms of fetal surgery. We present our experience with endoscopic fetal surgery over the past 10 years.
Technique: All procedures are performed under general anesthesia. After preoperative ultrasonographic mapping of the placental position and locations of recipient and donor, a minilaparotomy incision (2.0 cm) is created. The subcutaneous tissues, fascia, and muscle layers are divided to enter the peritoneal cavity. Once the uterine surface is exposed, the recipient sac is accessed via Seldinger technique. A 14-French peel-away introducer is used as a cannula to accommodate a custom-curved 9-Fr sheath containing a 1.9-mm semirigid fiber endoscope. Concomitant endoscopy and ultrasonography is used to map the umbilical cord insertions and the avascular plane between the vascular beds. Laser ablation is performed on unpaired vessels crossing the intertwin membrane using a diode laser (wavelength 940 nm) at powers between 5 to 15 W. The cannula is removed while a gelatin sponge plug is placed. Postoperative nifedipine tocolysis is routinely utilized.
Results: From 2000 to 2010, 62 endoscopic laser ablations of placental vessels for TTTS were performed. Median number of placental vessels ablated was four. The incidence of preterm rupture of membranes (PROM) was 5%. Overall survival was 70%, with at least one twin surviving in 82%. Tocolysis was used in 73% of patients for a median of 12 hours.
Conclusions: We demonstrate successful utilization of endoscopic laser ablation of placental vessels for TTTS over 10 years. The combination of an open surgical approach, Seldinger technique, and uterine plugging led to outcomes similar to other reports, with a 2–3 times lower PROM rate. Although TTTS is the most common application of endoscopic fetal surgery, this approach is applicable for other indications. Insertion and removal of tracheal occlusion balloons for severe congenital diaphragmatic hernia are currently being performed at our institution.
Children's Mercy Hospital and Clinics, Kansas city, MO
Introduction: Laparoscopic adrenalectomy is presently recognized as the standard approach for adrenalectomy for benign lesions in adults. The published experience in children and adolescents has been limited to sporadic small case series. To better describe the feasibility of the laparoscopic approach to adrenalectomy in the pediatric population, we conducted a large multicenter review of children who have undergone laparoscopic adrenalectomy.
Methods: After IRB approval, a retrospective review was conducted on all patients who have undergone laparoscopic adrenalectomy at 9 institutions over the past 10 years. Operative times included unilateral adrenalectomy without concomitant procedures. Continuous variables are expressed as mean ± standard deviation (range) and are compared using 2-tailed Student's T-test.
Results: 98 patients were identified of whom there were 51 males (52%). Laterality included 56 left-sided lesions (57%), 38 right (39%), and 4 bilateral (4%). Mean age was 9.3 ± 6.1 years (0.0–25.5) with a mean weight of 40.2 ± 26.1 kg (3.4–125). Mean maximal tumor dimension was 4.4 ± 2.1 cm (1.8–14.0), and mean operating time was 128 ± 64 minutes (44–404). Most common pathologies were neuroblastoma (29), pheochromocytoma (22), ganglioneuroma (13), and adenoma (11). Pre-operative chemotherapy was used for neuroblastoma in 20/30 cases (66.7%). There were 8 conversions to an open operation (8.2%). Most conversions were due to tumor adherence to surrounding organs as tumor size was not different in converted cases (P = 0.51). A blood transfusion was required in 4 cases (4.1%). The only postoperative complication was renal infarction after resection of a large neuroblastoma that required skeletonization of the renal vessels. At a median follow-up of 18 months (range 1–91), there was only one local recurrence which was in a patient with a pheochromocytoma.
Conclusions: The laparoscopic approach for adrenalectomy in children is feasible and can be applied for a wide variety of conditions regardless of age or the size of the lesion, with greater then 90% chance of completing the operation without conversion. The risk for significant blood loss or complications is low and it should be considered the preferred approach for the majority of adrenal lesions in children.
Laparoscopic Versus Open Inguinal Herniotomy in Infants and Children: A Meta-Analysis
Background: Inguinal hernia repair is one of the most frequently performed pediatric surgical operations. Open repair has been accepted as the gold standard. Several laparoscopic techniques have been introduced over the last few years. Unresolved debate still exists regarding the benefit of using laparoscopy over conventional open repair even among laparoscopic surgeons.
Objectives: To undertake a meta-analysis of published comparative data of laparoscopic versus open inguinal herniotomy in infants and children.
Methods
Search strategy: We searched MEDLINE, EMBASE, and The Cochrane Central Controlled Trials Registry for relevant randomized controlled trials and observational studies. The reference list of identified studies, journal supplements, relevant book chapters, and conference proceedings were searched for further relevant studies. Content experts were contacted for information on any other recent and ongoing trials known to them.
Selection criteria: All published randomized controlled trials and observational studies comparing laparoscopic with open inguinal hernia repair in children aged less than 19 years were eligible for inclusion.
Data collection and analysis: Two of the authors independently assessed study quality using the Newcastle-Ottawa Quality Assessment Scale for quality of observational studies. A fixed effects model was used to estimate a summary odds ratio (OR) with 95% confidence intervals (CI) for dichotomous data, and to calculate weighted mean difference (WMD) with 95% confidence intervals (CI) between continuous variables.
Results: Data on 2699 infants and children were identified from 10 comparative studies (two randomized controlled trials, one nonrandomized trial, and seven cohort studies). Laparoscopic techniques were associated with trend toward higher recurrence rate (OR = 1.81; 95% CI, 0.89 to 3.67; p = 0.10), longer operative time for unilateral repairs (WMD = 10.23; 95% CI, 8.82 to 11.64; p < 0.00001), and may be shorter operative time for bilateral repairs (WMD = −4.54; 95% CI, −11.63 to 2.55; p = 0.21). There was a significant reduction in developing contralateral metachronous inguinal hernia in the laparoscopic group (OR = 0.37; 95% CI 0.20 to 0.67; p = 0.001).
Authors' conclusions: The review showed that laparoscopic inguinal herniotomy is significantly associated with longer operative time for unilateral cases and a reduction in metachronous hernia development. There was a trend toward higher recurrence rate for laparoscopic repairs and shorter operative time for bilateral cases. A well-conducted randomized controlled trial is warranted to compare both approaches.
Differentiated Approach to Laparoscopic Vaginal Construction in Adolescents − 7 Years Experience with 48 Patients
Introduction: The purpose of this study was to evaluate the results of our differentiated approach to videolaparoscopic vaginal reconstruction in adolescent patients with absent vagina.
Materials and Methods: 48 patients (aged from 13 to 17 years) underwent laparoscopic neovaginoplasties during the period from 2004 to 2010 for Mayer-Rokitansky-Kuster-Hauser syndrome (MRKHS)–in 35 girls (XX genotype) and for testicular feminization syndrome (TFS)—in 13 XY patients. Two variants of laparoscopic treatment were used: In 12 patients with existing 1–3 cm of distal vagina (10–with MRKHS and 2 with TFS)—laparoscopic vaginal dissection and forceful dilatation and elongation was elaborated. This simple method made it possible to elongate vagina up to 9–11 cm depth and to avoid more complex surgical operations; In 36 patients (25 with MRKHS and 11 with TFS) laparoscopic total intracorporeal sigmoid vaginoplasty was performed. Three trocars (12 mm umbilical+ two 5 mm) were used in all cases. A 15 cm segment of sigmoid colon with two preserved feeding vessels was isolated with “Ligasure” dissection and linear staplers. One end of the segment was pulled down to the perineum and sutured in the hymenal region to form the neovaginal orifice (single layer anastomosis with demuscularisation of the distal 1–1.5 cm of bowel). The bowel integrity was reestablished using Ethicon circular stapler (from 21 to 29 mm in diameter). Our method of circular stapler usage in these cases was totally intracorporeal and made it possible to avoid any minilaparotomy or trocar incision broadening providing excellent cosmetic results.
Results: In the group with laparoscopic vaginal elongation there were no complications, except one case of vaginal prolapse (treated with laparoscopic vaginal sacropexy). The average operating time was about 25 minutes. During the period of postoperative observation (from 6 months to 5 years) regular dilatation and sexual activity later on made it possible to achieve and maintain satisfactory vaginal volume. The mean operating time in sigmoid vaginoplasty group was about 110 minutes (from 80 to 240 min.), and the postoperative hospital stay varied from 4 to 7 days. No cases of conversion occurred. Mild introital stenosis on skin level was observed and easily treated conservatively in 3 patients. There were no other postoperative complications and no additional surgical manipulations were needed during the period from 3 months to 7 years. Cosmetic results were excellent.
Conclusion: Both types of laparoscopic procedures for absent vagina in adolescent patients showed excellent results with low complications rate and good quality of general and sexual life. Laparoscopic vaginal elongation provides simple and effective alternative to complex surgical technologies in the cases with the present vaginal introitus. Laparoscopic sigmoid vaginal replacement is a feasible and safe operation and may be employed as an “gold standard” procedure. The modified method of intracorporeal sigmoid vaginoplasty provides excellent functional and cosmetic results in the patients with MRKHS and TFS without any significant difference between these two groups.
Bronchoscopic Removal of Aspirated Foreign Bodies: An Essential Skill for a Paediatric Surgeon Working in the Developing World
Introduction: Foreign body aspiration is a common respiratory emergency and an important cause of pulmonary complications and accidental death in children. A high index of suspicion and an early bronchoscopy are essential for the removal of a foreign body to prevent morbidity and mortality. As thoracic surgeons are not available in many hospitals in the developing world, the ability to remove aspirated foreign bodies by bronchoscopy is an essential and life-saving skill for Paediatric Surgeons practicing in such areas.
Aim: We aim to analyze our experience in the management of aspirated foreign bodies and share the lessons we have learnt during the management of these patients.
Background: The East London Hospital Complex (Frere and Cecilia Makiwane) hospitals are the only public sector hospitals with bronchoscopic facilities and expertise in the retrieval of aspirated foreign bodies in the eastern two thirds of the Eastern Cape Province in South Africa. These hospitals serve the population of approximately 6 million people, 40% of which are children under the age of 18 years.
Patients and Methods: This is a retrospective analysis of the cases of aspirated foreign bodies in children up to 15 years of age managed in our unit in a 15 year period from February 1995 to June 2010. The operation records, inpatient database, copies of the discharge summaries, patient records, and their radiographs were analyzed. We studied the distance of child's home from our hospitals, the clinical presentation, the radiographic findings, the surgeon who did the procedure, the nature of foreign bodies, and the immediate postoperative complications and compare our data with the available English language literature.
Results: There were 32 children with the diagnosis of foreign body aspiration during this period. The majority of these children resided between 50 and 200 km from our hospitals and were older than 4 years at the time of presentation. More than half of these patients presented with acute onset of respiratory distress without a history of choking. A radio-opaque foreign body was visible only in 40% of children. In 40% of the patients the chest radiograph was normal. The foreign bodies were removed with the rigid bronchoscopes by consultant surgeons or by registrars under direct supervision. We had higher incidence of inorganic foreign bodies. One patient had tension pneumothorax and surgical emphysema that settled with a chest drain. There was no mortality.
Lessons Learnt: The typical history of choking and/or foreign body aspiration may not always be present. A normal chest radiograph does not rule out an aspirated foreign body. An early bronchoscopy done by a competent surgeon with a rigid bronchoscope deals effectively with the problem with minimum morbidity.
Conclusion: The ability to safely remove an aspirated foreign body is an essential skill to be acquired as part of the training of Paediatric Surgeons in the developing world.
Improved Insulin Sensitivity and Decreased Insulin Secretion in Adolescents Undergoing Gastric Bypass
Introduction: Insulin resistance (IR) is a key feature of most obesity-related comorbidities. Roux en Y gastric bypass (RYGB) causes substantial weight loss, but effects on IR and carbohydrate metabolism in adolescents are not fully understood.
Methods: Intravenous glucose tolerance tests (IVGTT) were used to prospectively characterize metabolic responses to RYGB in adolescents before and 1 year after surgery. Twenty-three subjects studied included 2 with T2DM; age range 14–20 (mean 17 years); gender distribution 15F/8M; 18 Caucasian, 5 AA. The study protocol was IRB approved; informed consent provided by caregivers while participants assented to the study procedures.
Results: Concomitant with mean (±SD) decrease in BMI from 60 ± 12 to 38 ± 8 kg/m2, mean (±SD) insulin sensitivity (SI) increased 5-fold (0.79 ± 1 to 4.2 ± 3 min-1 pM-1 [p < 0.01]). While the the acute insulin response to glucose, AIRg, decreased 2-fold (864 ± 482 to 380 ± 177 pmol/L [p < 0.01]), when corrected for the changes in insulin sensitivity (disposition index) there was an increase of beta-cell function, although this did not reach statistical significance (772 ± 823 [baseline] and 1398 ± 1020 [1 yr; p = 0.26]).
Conclusions: These data suggest that RYGB in adolescents significantly improves insulin sensitivity, associated with a compensatory decrease in insulin secretion after IV glucose stimulus. Although these findings document a clear metabolic benefit of RYGB for morbidly obese adolescents, further research is needed to determine the degree to which weight loss and improvement in carbohydrate metabolism will impact long-term risks of diabetes and cardiovascular sequelae of persistent obesity in adolescents undergoing weight loss surgery.
This work was supported by NIH grant R03DK068228-01A1 (Dr. Inge)
NOTES (Natural Orifice Transluminal Endoscopic Surgery)
Experience with Endoscopic and Endoscopic-Assisted Management of Pediatric Surgical Problems: Results and Lessons
Purpose: Minimally invasive operative techniques are becoming increasingly popular within the pediatric population. Endoscopy may enhance or replace existing techniques in the future. Many of the reported benefits of laparoscopy and thoracoscopy may apply to endoscopy and endoscopic-assisted procedures; however, no reports exist as to the application, results, and outcomes for these procedures in children. We hypothesized that endoscopy is a useful and safe adjunct for pediatric surgical patients.
Methods: We retrospectively reviewed the medical records of patients who have undergone endoscopic or endoscopic-assisted operations within the division of pediatric surgery at two children's hospitals over 3 years (August 31, 2007–August 31, 2010). During this time period, 30 procedures were performed on 28 patients. Indications for procedure, age, operative technique, operative times, surgical outcomes, complications, and length of stay for each patient were reviewed.
Results: Patient age ranged from 3 days to 20 years and weight ranged from 1.7 kg to 75 kg. Indications for operation included esophageal pathology in 12 cases including pharyngeal stricture; cricopharyngeal achalasia; esophageal strictures; and esophageal duplications. Gastric and duodenal pathology was managed in 12 cases including gastroparesis; perforated gastric ulcer; gastric tumor; gastric volvulus; displaced gastrostomy tubes; and duodenal atresias, webs, and strictures. The final 3 cases were pancreatic pseudocyst (2) and displaced sigmoid cecostomy tube. Of those foregut endoscopies, 26 were completed transorally while 3 were completed with a combined transoral/transgastrostomy approach. One colonoscopic procedure was performed. Although endoscopy was intended only as an adjunct in all cases, the planned procedure was satisfactorily completed with a purely endoscopic approach in 5 cases; traditional laparoscopy (14) or thoracoscopy (10) was required to complete the other procedures. There were no intra-operative complications. Postoperative complications included stridor (2) and anastomotic leak (1), all managed conservatively. One open cervical myotomy was performed for cricopharyngeal achalasia. One patient required a repeat endoscopic procedure followed by an endoscopic-assisted laparoscopic duodenoduodenostomy for a duodenal web.
Conclusions: We conclude that endoscopy offers a promising adjunct to more traditional minimally invasive techniques in children. In some cases, endoscopy may offer an alternative to more invasive procedures or eliminate the need for tube thoracoscopy or postprocedural contrast studies in some esophageal cases.
Embryonic Natural Orifice Transumbilical-Anal Endoscopic Surgery (E-Notes) for Hirschsprung's Disease
Objective: The quest to make more minimally invasive techniques has generated a drive within the surgical community to explore novel ways of achieving this. This has led to surgeons attempting to either decrease the number of trocars placed through the abdominal wall or eliminate them completely. This led to the evolution of several approaches, including natural orifice translumenal endoscopic surgery (NOTES), single-incision laparoscopic surgery (SILS), transumbilical endoscopic surgery (TUES), or embryonic natural orifice transumbilical endoscopic surgery (E-NOTES). We report on the feasibility and safety of NOTES subtotal colectomy using transanal endorectal pull-through (TAEPT) surgery with transumbilical laparoscopic visualization for Hirschsprung's disease with the long aganglionic segment.
Methods: Through a single 0.5-cm intraumbilical incision and a single-access trocar, a 5-mm 30° laparoscope was introduced into the peritoneal cavity. Under the laparoscopic vision, two 5-mm working trocar were inserted transanal through the rectal muscular cuff into pelvic cavity. The total colonic mesentery was dissected and the ileocecum was mobilized using an ultrasonic scalpel. A transanal endorectal pull-through subtotal colectomy and a coloanal anastomosis were done.
Results: From Feburary to August 2010, 6 infants with Hirschsprung's disease with a transition zone to the splenic flexure or transverse colon underwent a TAEPT with E-NOTES. E-NOTES in all 3 cases was completed successfully without conversion to standard laparoscopic approach. Median operative time for creating an E-NOTES access and the ensuing TAEPT procedures was 4 min (range 3–6 min) and 95 min (range 75–110 min), respectively. Median blood loss was <20 ml. No complications requiring treatment occurred.
Conclusions: TAEPT with E-NOTES is a feasible alternative method for subtotal colectomy with better cosmetic outcome. Natural orifices present an unprecedented opportunity for scar-free surgery. Ongoing refinement in technique and instrument is likely to expand its future role.
Transesophageal Right Upper Pulmonary Lobectomy: In Vivo Porcine Experimental Study
Background and Study Aims: Video-assisted thoracoscopic surgery (VATS) is being widespread as the better approach to carry out pulmonary lobectomy. Natural Orifice Transluminal Endoscopic Surgery (NOTES) is being assessed as an alternative to the transthoracic endoscopic surgery. We designed this study to test the feasibility of peroral transesophageal right upper pulmonary lobectomy with the assistance of a single transthoracic trocar.
Material and Methods: In 10 anesthetized pigs (35–45 Kg), we performed right upper pulmonary lobectomy using a forward viewing double-channel gastroscope (introduced perorally) and an operative thoracoscope with a 5 mm working channel (introduced through a single-transthoracic 10 mm port) (Karl Storz). After introducing the gastroscope throughout an oroesophageal overtube into the esophagus, a 1 cm transverse esophagotomy was carried out in the upper third using an ESD-knife under thoracoscope control. Anatomic dissection of the right upper hilum was performed using flexible (gastroscope) and rigid (thoracoscope) instruments. After individual dissection, right upper pulmonary arteries, veins, and correspondent bronchus were independently stapled using a 45 mm long, linear endostapler (EndoPath®, Ethicon Endo-Surgery) introduced through the oroesophageal overtube. After completing the lobe resection using an endoscopic snare with cautery, the specimen was extracted retrogradely through the mouth. The esophagotomy was stitched and tied using Endo Stitch™ (Covidien) and a long knot-pusher; both were handled through the oroesophageal overtube.
Results: Esophagotomy was performed safely in all animals. Dissection of the right upper lobe hilum elements (arteries, veins, and bronchus) was also carried out in all animals without significant problems. Oroesophageal handling of the endostapplers for independent ligation of the hilum elements under transthoracic imaging was surprisingly feasible, reasonably easy to perform and reliable in 7 cases. In two cases ligation of the vessels was en bloc. In one case, severe hemorrhage occurred from incomplete vein ligation, although we could control it using electrocoagulation (this pig died before pulmonary lobectomy was completed). Esophagotomy closure was feasible but its reliability was not tested in survival studies. All but one animal were kept alive until the end of the acute experiment when they were sacrificed.
Conclusions: Transesophageal right upper pulmonary lobectomy using single transthoracic trocar assistance is feasible and it may represent a step toward scarless pulmonary lobectomy. Additional survival studies are necessary to test the reliability of this procedure.
Robotics
Autonomous Interventions: Progress on Image-Guided Robotics
Introduction: The development of sophisticated imaging systems that provide 3 dimensional data with a high degree of resolution allows real time identification of the exact coordinates of a potential target in space. Transfer of the coordinates to a robotic guidance system allows autonomous access to the lesion.
Methods: Initial feasibility studies were done with a simple 3 axis robot (Gantry III Cartesian Robot Linear Motion System (Techno-Isel, Techno, Inc., New Hyde Park, NY) and real-time ultrasound imaging (Duke/Volumetrics 3D scanner system (Volumetrics Medical Imaging, Durham, NC). A water phantom containing 14 wire tips was used to measure the accuracy of the ultrasound-guided system. Subsequently, a 4-D imaging system (GE Logiq L9 scanner) was combined with a turkey breast phantom and image analysis to simulate autonomous biopsy of breast lesions. A biopsy needle was incorporated into the system such that the system identified the lesion, guided the biopsy probe to the lesion, and fired the biopsy probe. In an effort to improve the sophistication of the robot system, an iARM Assistive Robotic Manipulator with 6 + 1 degrees of freedom manufactured by Exact Dynamics BV (Didam, The Netherlands) has been used to direct a needle to a sciatic nerve phantom to simulate sciatic nerve block.
Results: For the initial studies using the Cartesian robot and wire phantom the robot accurately guided the needle to the target (Fig. 1). 16 data points were collected and the mean root mean square (RMS) error for these 3D scan measurements was found to be 1.34 mm ± 0.68 mm.
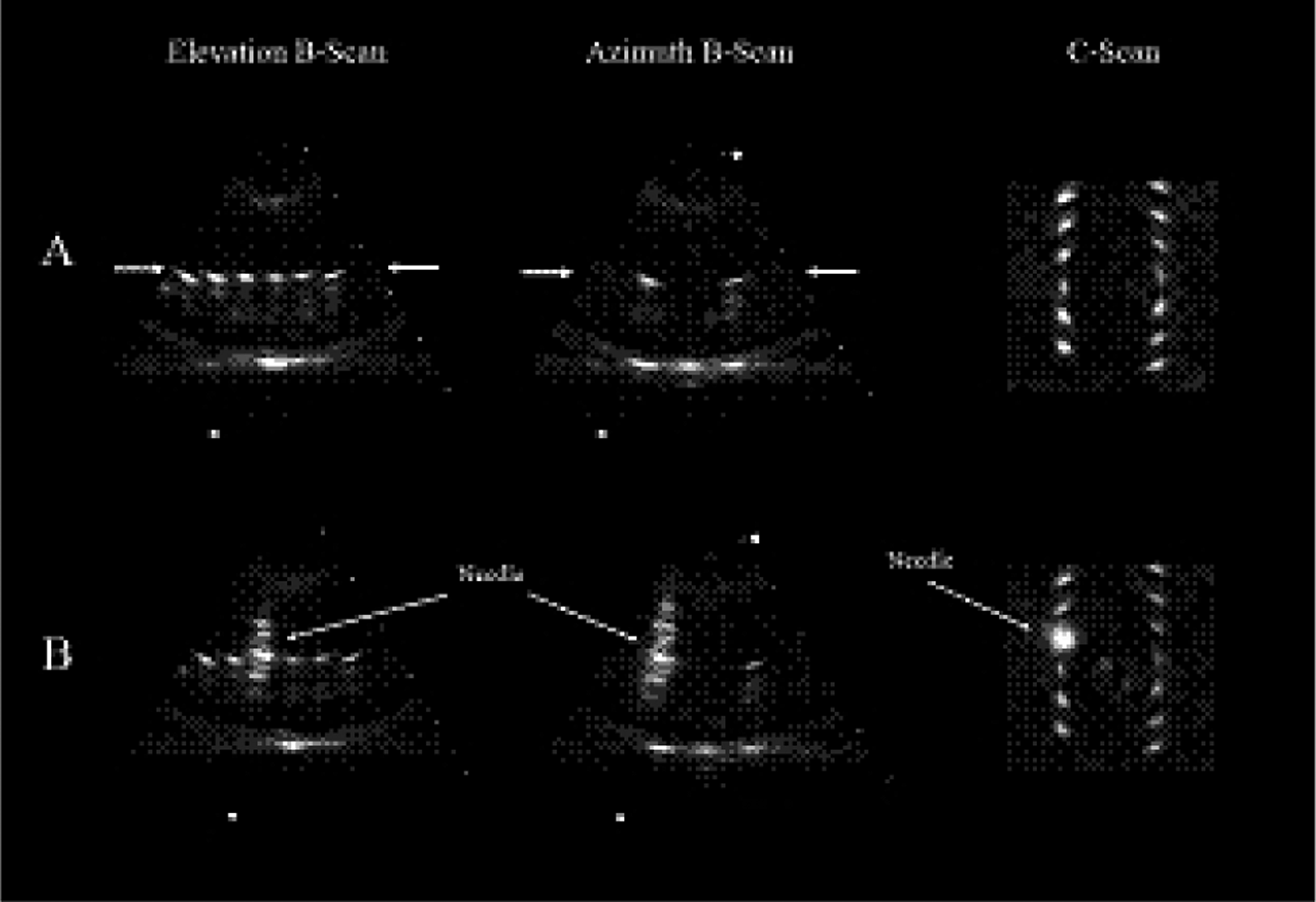
For the breast simulation with the 4D scanner and image analysis software, the procedure time was 65 seconds and the RMS error was 2.82 mm. The sciatic nerve model demonstrates the feasibility of incorporating the increased capability of the iARM robot into the guidance system.
Conclusions: Substantial progress has been made in developing a truly autonomous image guided system to access lesions visualized on ultrasound. Progressive sophistication of the communication between the imaging system and the increasingly sophisticated robotic guidance systems will reduce procedure time and increase accuracy. The techniques being developed would revolutionize multiple clinical applications in the diagnosis and treatment of radiographically identified pathologic lesions in many solid organs. Potential interventions could include diagnosis using biopsy needles or therapy using radiofrequency ablation or cryotherapy probes.
Single-Incision Laparoscopic Surgery
Background: Minimally invasive procedures for inflammatory bowel disease have been shown to be safe and improve recovery in children. We report our initial experience with single-incision laparoscopic operations for pediatric chronic ulcerative colitis (UC) and Crohn disease (CD).
Methods: We retrospectively reviewed perioperative outcomes for 11 consecutive patients (4 females) that were referred to our multidisciplinary pediatric inflammatory bowel disease clinic from March 2010 to August 2010. All procedures were conducted using standard 5-mm laparoscopic instruments and either a 50-cm laparoscope or a deflectable video laparoscope in one patient. Single site access was obtained using the Gelpoint device (Applied Medical) in 6 patients or with the Quadport or Triport (Olympus) in 4. A wound protector with surgical glove was used in 1. Mesentery was divided using LigaSure (Covidien). Ileal pouches were created extracorporeally. The rectum was divided by everting the bowel transanally. Double stapled anal anastomosis was used in 6 of the 7 IPAA patients.
Results: Mean age was 14 years (range 9–17 years). Preoperative diagnoses included: 6 with UC, 2 with CD (1 colonic, 1 ileocolonic), 2 with familial adenomatous polyposis, 1 with UC and juvenile polyposis, and 1 with indeterminate colitis. Procedures included: 3 total abdominal colectomies (TAC) with end ileostomy, 3 two-stage IPAA, 2 single-stage IPAA, 2 three-stage IPAA, and 1 completion ileocectomy with primary ileocolostomy in a patient with a prior ileostomy for perforated CD. Mean operating time for all procedures was 283 minutes (168 mins. ileocectomy, 254 mins. TAC, 267 mins. three-stage IPAA, 300 mins. single-stage IPAA, and 349 mins. two-stage IPAA). In all but 2 patients, the access device was placed in a predetermined ileostomy site. A 5-mm accessory umbilical port was used in 5 operations (4 IPAA, 1 TAC). Mean skin incision length was 2.5 cms with the largest incisions occurring at the site of previously placed ileostomies. Mean fascial incision length was 4.1 cms. The skin and fascial incisions have been reduced to 1.5 cms and 3 cms respectively for our last 2 IPAA patients. Postoperative complications have occurred in 5 patients (45%). Anastomotic leak occurred in 2 IPAA patients without protective ileostomy, 1 small bowel obstruction necessitating early stoma takedown, 1 pelvic abscess and portal vein thrombosis in a patient undergoing TAC, and 1 readmission for dehydration in a patient following IPAA with diverting loop ileostomy. Both patients with anastomotic leak underwent diverting loop ileostomies with one requiring percutaneous drain placement. One patient that leaked had her diverting stoma reversed with excellent results. Mean length of stay was 4 days (range 3–9 days).
Conclusions: Single-incision laparoscopic colon and rectal surgery for pediatric inflammatory bowel disease is feasible using standard laparoscopic instruments. An accessory umbilical port is useful for patients with markedly inflamed or edematous colons that are difficult to manipulate. This port site is invisible after completely healing. Currently we do not advocate single-incision IPAA without a protective stoma due to the high rate of anastomotic leak. Continued advancement in instrumentation and experience will decrease incision size and shorten operative times.
Comparison of Single Port Laparoscopic Surgery in Small Vs. Large Children
Introduction: Single port laparoscopic surgery (SPLS) is gaining wider acceptance in the adult patient population. Application of this new technique in children requires using existing adult technology since smaller, specialized ports and instruments designed for the pediatric age group are lacking. This raises potential concerns that oversized instruments may compromise the procedural outcomes. We set out to evaluate our SPLS experience in smaller patients as compared to “adult” sized children.
Methods: An IRB-approved, retrospective chart review of all patients who underwent SPLS at a dedicated children's hospital during a one year period from Sept 2009 to Sept 2010 was conducted. Every patient weighing 25 kg or less (n = 45) was placed in a small patient group (SPG) and compared to all patients weighing 70 kg or more (n = 46) who were placed in the large patient group (LPG). Data on type of procedure, technique and instrumentation, length of operation, length of hospitalization, pain medication usage, and complications were collected.
Results: The SPG had a mean weight of 19 kg (range 10–25) and a mean age of 6 years (range 1 to 10 years). These patients successfully underwent 36 appendectomies, 3 diagnostic laparoscopies, 2 cholecystectomies, 2 diaphragmatic hernia repairs, 2 ventriculoperitoneal shunt revisions, 1 splenectomy and 1 oophorectomy. The LPG had a mean weight of 81 kg (range 70–117 kg) and a mean age of 15 years (range 10–18). The LPG underwent 25 appendectomies, 18 cholecystectomies and 3 gynecologic procedures. There were no conversions in the SPG, but one LPG appendectomy required extension of the incision to complete the case. Both groups used the same port, telescope and instrument sets (standard or articulating 5 mm instruments and 10 mm endostaplers or suturing devices, when needed). Direct comparison of some parameters was not possible due to different case type distribution between groups, but a subgroups analysis of appendectomy patients revealed a significantly longer operative time in the LPG (mean 35.5 min. vs 27.2 min, p < .05). There was no difference in length of stay (median 1 day), postoperative pain medicine usage (median 1 dose) or wound infectious complication rate for acute appendectomies (4% LPG vs 0% SPG) and for complicated/perforated appendectomies (36% LPG vs 33% SPG). There was one readmission in each group, both after acute appendectomies, for abdominal pain (SPG) and for gastroenteritis (LPG).
Conclusions: Our results indicate that current SPLS technology, although designed for adult-sized patients, is safe and effective in lower weight pediatric patients. The comparable outcomes in both the LPG and SPG suggests that refinement of instrument and port technology for pediatric applications may yield improved results in smaller children.
Is Single-Incision Laparoscopic Cholecystectomy as Good as Advertised? A Comparative Analysis to the Standard Laparoscopic Cholecystectomy in Children
Purpose: Single-incision laparoscopic (SIL) cholecystectomy is gaining popularity. Early reports have shown the procedure is safe and feasible. However, the question remains whether or not the technique is as effective as the standard 4-trochar laparoscopic (SL) cholecystectomy. The aim of this study is to evaluate the outcomes and to determine if SIL cholecystectomy is comparable to the (SL) cholecystectomy, especially after the initial learning curve.
Methods: After the approval of the institutional review board (606-09CR), we performed a retrospective chart review of consecutive patients who underwent cholecystectomy using SIL from 01/2008 to 9/2010 compared with 50 consecutive patients who underwent the SL cholecystectomy prior to the introduction of the SIL approach. Cases with concurrent procedures were excluded from the study. Pertinent information include demographics, operative (OR) times, intraoperative details, length of stay, blood loss, IV narcotic usage, excluding doses given in the postoperative care unit (PACU), and postoperative results were analyzed. A Student t-test was used to compare data between the two groups with the p-value <0.05 being statistically significant.
Results: During the study period, we identified 38 patients (33 females and 5 males) in the SIL group. Both groups have similar demographics with the average age 15 yrs (8–20 yrs) and weight 69.2 kg (20–120 kg) in the SIL group vs 14.8 yrs (3–22 yrs) and 68.8 kg (32–141 kg) in SL group, respectively. The majority (92%) of the patients in two groups present with cholesterol stones (35/38 vs 46/50). Of the 38 subjects in the SIL group, 4 (10.5%) had acute cholecystitis and 5 (13%) developed pancreatitis compared with 3 (6%) and 7 (14%) in the SL group. Five patients in the SIL group required intraoperative cholangiogram (IOC) as opposed 13 patients in the SL group. The mean OR time for SIL cholecystectomies was 82.3 minutes compared to 70.8 minutes in the SL group (p = 0.0608). Eliminating the first ten cases as the initial learning curve, the average operating time for the remaining cases was 71.6 minutes (p = 0.9058). There were no intra-operative complications or conversions in either group with the blood loss reported as “minimal” (<20 cc) in all cases. The average length of stay was 1.9 days in the study group vs. 2.3 in the standard group, (p < 0.24). During postoperative stays, the patients in the SIL group received, on average, 1 dose of IV narcotics compared with 2.9 doses in the SL group, (p < 0.007). At one month postoperative follow-up, all patients underwent SIL cholecystectomy had satisfactory recovery without postoperative complication, and excellent cosmetic results
Conclusion: Single-incision laparoscopic cholecystectomy is safe and feasible when compared with the standard laparoscopic cholecystectomy. Operative time tended to be longer during the initial learning period but reduced to a comparable operative time to that of SL cholecystectomy thereafter. However the data are retrospective and therefore confounded. A prospective randomized control trial is necessary to determine if one technique is superior to the other.
Single-Incision Pediatric Endosurgical (SIPES) Nissen Fundoplication: A Technique in Evolution
Background: Single-incision Pediatric Endosurgery (SIPES) is gaining popularity for routine ablative cases such as appendectomies and cholecystectomies in a number of centers. We have employed this technique for Nissen fundoplication as a reconstructive procedure.
Objective: To describe the technical evolution of SIPES fundoplication at our center, and to discuss the challenges faced in our series.
Materials and Methods: After IRB approval was obtained, data were prospectively collected on all SIPES fundoplications performed in our hospital from September 2009 through August 2010. Different surgical techniques, operative times, blood loss, complications, additional trocar placement, and outcomes were recorded and described.
Results: SIPES fundoplication was attempted in 10 children (ages 3 months to 11 years, median 21 months; weight 5.5 to 51 kg, median 9 kg). Fundoplication was performed either as the sole procedure in 4 patients, or combined with a gastrostomy in 6 patients. On average, total operative time decreased throughout the observation period (Fig. 1). The mean estimated blood loss was 6 ± 5 ml, and postoperative length of stay was 2.6 ± 1.4 days. Different trocars, liver retraction methods, and suturing techniques were employed. Intracorporeal knot tying was used in 7 operations. There were no intraoperative complications, but additional trocars were added in 2 cases. Reflux symptoms subsided in all patients, with a median follow-up of 7 months (range 1 to 12 months). One patient underwent planned dilation of a persistent preoperatively apparent lower esophageal stricture 3 months after the procedure. In another patient, the gastrostomy tube inadvertently dislodged twice, 2 days and again 2 weeks after the initial surgery.
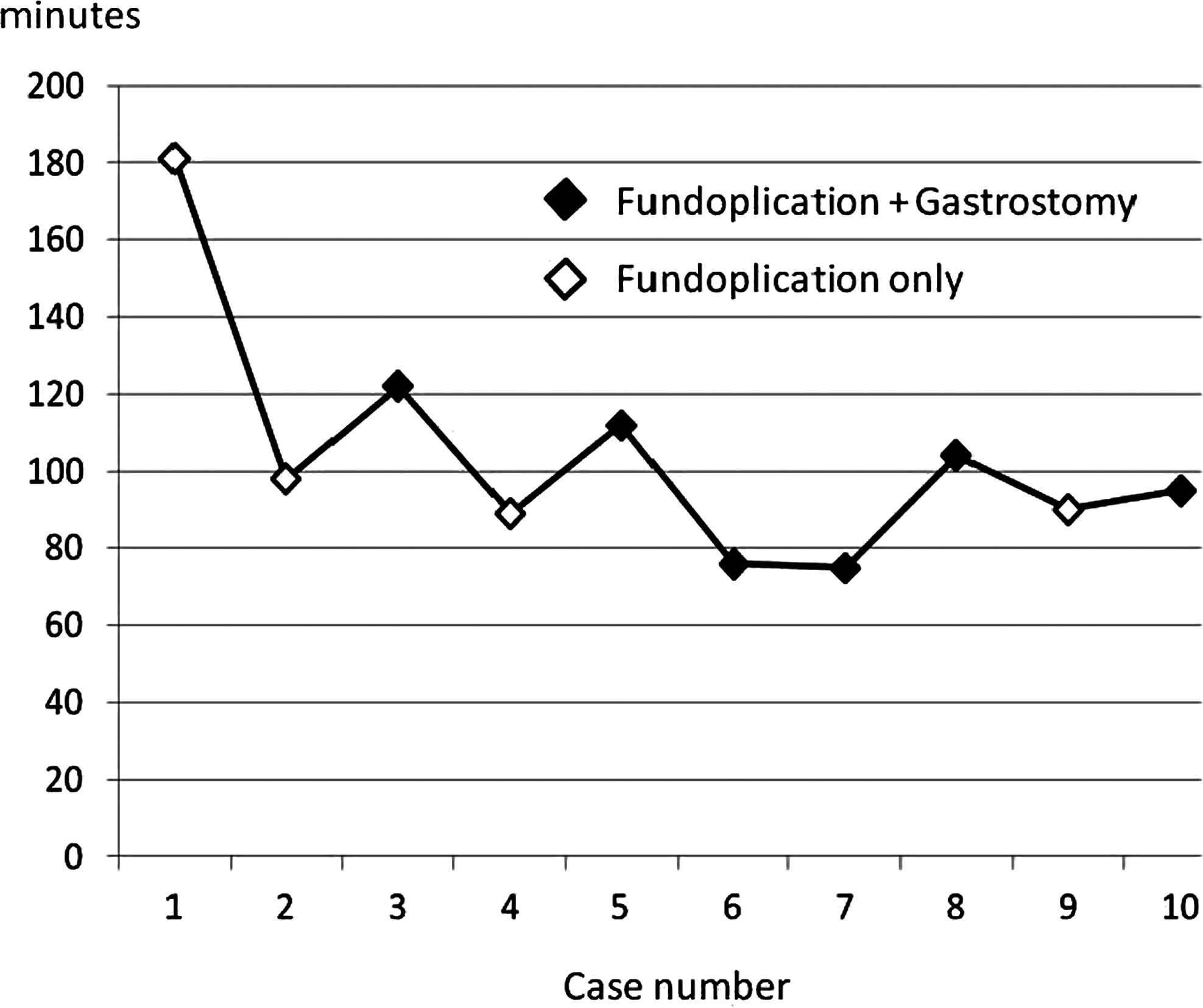
Operative time for SIPES Nissen fundoplication.
Conclusion: Laparoscopic Nissen fundoplication can be accomplished successfully and safely using single-incision endosurgery in children, without leaving any appreciable scar. Although the technique is still evolving, operative times have reached a plateau. So far, no recurrent reflux symptoms, breakdown of the wrap, or hiatal hernias have been observed in the patients.
Background: Laparoscopy is the gold standard of treatment of a pyloric stenosis. The benefits of the endoscopic pyloromyotomy includes a shorter hospital stay and faster return to feeds. The standard laparoscopic approach for correction of congenital pyloric stenosis based on the 3-port technique using two incisions to pass operating instruments. In contrast to the standard laparoscopic technique, the single-incision laparoscopic surgery (SILS) requires only one incision. We report on our experience with this surgical approach.
Materials and Methods: Between September 2009 and August 2010 a total of 24 children underwent a laparoscopic pyloromyotomy, 12 in SILS technique. The single-incision was carried through the center of the umbilicus. A Veress needle was passed through the umbilical fascia. The trocar for optic telescope was inserted through an umbilical incision. The working instruments were introduced in a two-dimensional direction into the peritoneal cavity via the same umbilical incision. Afterward, hypertrophied pylorus was grasped with a forceps, cut, and dissected as in standard laparoscopic surgery. The fascial defect was closed using absorbable suture. The two groups were compared for patients demographics, operative report, and early postoperative outcomes.
Results: All SILS procedures were performed successfully with no conversion rate. There were no differences in the preoperative parameters between the two groups regarding age before surgery and body weight at operation. Operative time and time of full enteral intake were similar to comparable procedures if using a standard laparoscopic approach. The postoperative course was uneventful in the all patients. There were no operative or postoperative complications.
Conclusions: SILS trocarless pyloromyotomy is a safe alternative to standard laparoscopic technique with three trocar approach. The minimal scarring guarantees an attractive cosmetic result. The early experience described in this study confirms that SILS can be applied for treatment of pyloric stenosis with outcomes similar to standard laparoscopic surgery.
Single-Incision Thoracoscopic Surgery (SITS) in Children: Equivalent Results with Fewer Scars as Compared to Traditional Multiple Incision Thoracoscopy
Background: Single-incision pediatric endosurgery is rapidly gaining popularity, particularly for abdominal operations. In an effort to minimize scarring, multiple trocars are passed through a single small incision to complete the operation. There are now several studies supporting the feasibility of the single-incision approach in pediatric laparoscopy. Previously, we have reported our early experience with single-incision thoracoscopic surgery (SITS) in the pediatric population. This study compares our current experience with SITS to traditional multiple incision video-assisted thoracoscopic surgery (VATS) in children.
Methods: With IRB approval, a retrospective chart review of all patients who have undergone a SITS procedure at our institution was performed. An equal number of VATS case controls were randomly chosen from a patient pool operated on during the same time period. Operative time, length of time until chest tube removal, length of hospital stay, complications, and any need for further operations were recorded. Statistical analysis was done by Student's t-test using Instat 3 (GraphPad, San Diego, CA) with p < 0.05 being considered significant.
Results: Fourteen patients underwent SITS during the study period. These patients were compared to 14 patients who had undergone similar procedures using traditional multiple incision VATS. Both groups were equivalent with regards to age, weight, and follow-up time. The procedures performed in the SITS group included 10 wedge resections, one mediastinal biopsy, one chest wall biopsy, one resection of an apical extrapulmonary neuroblastoma, and one drainage of an empyema. Mean operative time in the SITS group was 84 ± 43 minutes as compared to 64 ± 30 in the VATS group (p = 0.18). Days until chest tube removal was 4 ± 2.2 in the SITS group as compared to 2.8 ± 1.4 in the VATS group (p = 0.09). Length of hospital stay was shorter by 1.7 days in the SITS group, but this was not statistically significant (SITS 5.5 ± 4.4 days, VATS 7.2 ± 8.6 days; p = 0.51). There were no intraoperative complications in either group, and no patient in the study required conversion to open. One SITS patient who underwent an apical wedge resection and mechanical pleurodesis for a spontaneous pneumothorax was readmitted one week after discharge for a recurrent pneumothorax and persistent air leak. The patient required a reoperation and ultimately recovered fully. Notably, the patient was found to have an occult pulmonary aspergillus infection.
Conclusions: We have applied the single-incision approach not only to abdominal operations but also to a variety of thoracic conditions in children. Our experience demonstrates that there are no statistically significant differences in operative time, time until chest tube removal and length of hospital stay when comparing SITS to traditional multiple incision VATS. We believe that SITS is an equivalent procedure that allows for fewer scars as compared to VATS in children. A more critical prospective analysis with a larger number of patients is warranted to further validate this technique.
Initial Experience with Magnetically Assisted Single-Trocar Appendectomy (MASTA)
Background: Single trocar appendectomy offers excellent cosmetic results and may be associated with decreased postoperative pain, but it requires significant operator dexterity. In order to ease the procedure and maintain minimal invasiveness, we employed magnetic surgical devices to facilitate retraction and triangulation. The aim of our study was to report our initial experience using this novel technique.
Methods: Patients with acute appendicitis admitted to the General Surgery and Emergency Unit who agreed to undergo MASTA appendectomy were included in this retrospective study. Baseline and procedural data as well as surgical outcome were collected in a dedicated database.
Technique: Under general anesthesia, a 12 mm Trocar was introduced into the abdomen through the umbilicus followed by placement of an 11-mm 0° laparoscope with a 6-mm working channel (Storz, Tuttlingen, Germany). A powerful external handheld magnet was placed on the abdominal wall and used to move a 10 mm Deployable Magnetic Grasper (DMG) (Domínguez Magnetic Grasper®, Imanlap, Buenos Aires, Argentina). In order to deploy the DMG, we first withdrew the scope and the DMG was positioned at the trocar's entrance. A forceps was then introduced through the working channel and used to push the DMG inside the abdominal cavity. By means of the external handheld magnet the DMG was guided used to retract and move the appendix. Division and removal of the diseased appendix was performed according to standard laparoscopic techniques. Appendix was always retrieved through the trocar lumen.
Results: A total of eleven patients (six men and five women) underwent MASTA appendectomy. Mean Age was 10.5 ± 1.9 years and weight 37 ± 8 kg. The mean duration of the operation was 66 ± 28 min. Intraoperative inspection of the appendix revealed acute inflammation in seven cases, gangrenous in three and perforated in one case. Patients tolerated oral feeding at 22.9 ± 1.9 hours after surgery. The mean length of hospital stay was 3.9 ± 1.3 days. The operation was completed successfully in all patients. Conversion to multiport was required in one patient. No intraoperative or postoperative complications occurred.
Conclusion: Our preliminary results indicate that MASTA is feasible and safe in patients with acute appendicitis, offering cosmetically appealing results. Greater numbers and a prospective trial will be necessary to assess the true benefit of this approach.
Single-Incision Laparoscopic (SIL) Splenectomy in Pediatric Patients
Purpose: Splenectomy is an uncommon procedure in pediatric patients, the majority of which are performed laparoscopically with multiple incisions. The single-incision laparoscopic (SIL) technique is gaining popularity and many procedures such as cholecystectomy and appendectomy are performed using this novel approach. The aim of this study is to review our institutional experience thus far with splenectomy in the pediatric population using the SIL technique.
Method: The operation was performed by using a three-trochar technique via a single periumbilical or transumbilical incision. A roticulating grasper was used to retract the spleen. After splenic attachments were divided, the splenic vessels were individually ligated with the Ligasure device right along the capsule. The spleen was then placed in an Endo-catch bag, morcelated and removed through the umbilical incision. After the approval of the Institutional Review Board, we retrospectively evaluated the patients who underwent SIL splenectomy from Jan 2009 to present. Pertinent data was obtained from the medical charts.
Results: 5 patients, all female, underwent SIL splenectomy in the study period. One patient had a combined SIL splenectomy/cholecystectomy. 2 patients had hereditary spherocytosis, 2 had idiopathic thrombocytopenic purpura and one had splenic torsion. The average age was 11 yrs (6–15 yrs). Mean operating time was 142 minutes (96–180 min) including the combined procedure case. There were no intra-operative complications or conversions to open, and the average blood loss was minimal (<20 cc). Two patients were discharged home on POD# 1. The remaining 3 patients had longer hospital stays due to the etiology of their disease. None of the patient had postoperative complications, and all 5 of them were satisfied with the cosmetic results.
Conclusion: SIL splenectomy is a technically challenging procedure, which mandates surgical expertise. However, this technique is feasible and can be safely performed. The cosmetic result is excellent as the incision is well hidden within the umbilical fold. Further validation of this approach will require larger comparative studies to standard laparoscopic splenectomy.
Perforated Appendicitis: Is Single-Incision Laparoscopic Appendectomy (SILS) A Good Idea?
Background: Single-incision laparoscopic surgery (SILS) is becoming increasingly common for the management of acute appendicitis. Perforated appendicitis poses a major technical challenge for open as well as laparoscopic surgery. Question is whether single-incision laparoscopic appendectomy (SILS) is a good idea for perforated appendicitis? We looked at our experience so far with SILS in perforated appendicitis.
Methods: This is a retrospective study of children who underwent SILS for acute appendicitis, and were found to have perforated appendicitis by a single surgeon at our institution. Charts were reviewed from March 2009 to August 2010. All patients were followed 3–4 weeks postsurgery in the clinic. The variables analyzed were gender, age, operative time, complications, length of stay, and cosmetic results.
Results: 57 single-incision laparoscopic appendectomies for acute appendicitis were performed between May 2009 and August 2010. 12 children (20%) had intra-operative evidence of ruptured appendicitis. Perforation was more frequent in male than female (3:1 ratio). Operative time for ruptured appendicitis using SILS was 58 min average (range: 49–73 min). One patient with perforated appendicitis developed umbilical wound cellulitis which was managed successfully with antibiotics. None developed any postoperative intra-abdominal abscesses. One case was converted to traditional laparoscopic appendectomy. There were no conversions to an open procedure. Average length of stay was 3.6 days (range: 1–10 days). Patients and parents were extremely satisfied with the excellent cosmetic outcomes.
Conclusion: Our initial data suggest that SILS is a safe approach for perforated appendicitis in children. This innovative procedure can be performed in acceptable operative time with good outcomes and great cosmetic results.
The Learning Curve of Single-Incision Pediatric Endosurgery
Background: Single-incision pediatric endosurgery (SIPES) is gaining popularity in centers around the world. A concern in implementing these technically challenging procedures is the associated learning curve. In our hospital, over 340 SIPES cases have been performed so far. This study describes the learning curve associated with the 3 most common procedures appendectomy, cholecystectomy, and pyloromyotomy.
Methods: All SIPES appendectomies, cholecystectomies, and pyloromyotomies performed from April 2009 through July 2010 were chronologically divided into thirds, groups A (first), B (middle), and C (last). The learning curve for each operation was assessed by comparing operative times, conversion rates (defined as adding additional trocars), and complication rates among these groups.
Results: During the study period, we performed 183 appendectomies, 51 cholecystectomies, and 49 pyloromyotomies using SIPES technique. With increasing experience, operating times decreased significantly for all 3 operations (42 ± 14 to 36 ± 13 minutes for appendectomies, p = 0.015; 78 ± 20 to 59 ± 18 for cholecystectomies, p = 0.004; 26 ± 7.7 to 20 ± 5.5 minutes for pyloromyotomies, p = 0.015), but a plateau was reached earlier for cholecystectomies than for appendectomies or pyloromyotomies. The number of additional trocars placed during appendectomies declined steadily from 21% in group A to 0% in group C (p < 0.001). There were more complications during appendectomy in groups A versus B (8% versus 0%, p = 0.03), no other differences in complication rates were found.
Conclusion: Operating times for all SIPES operations declined throughout the study period. The learning curve may be shorter for cholecystectomies than for appendectomies or pyloromyotomies. With experience, the need for additional trocars and the complication rate during appendectomy approaches zero.
Single-Incision Laparoscopic Approach in Management of Splenic Pathologies in Children
Purpose: Certain splenic conditions in children require surgical interventions, the majority of which are approached via standard laparoscopy with multiple incisions. The single-incision laparoscopic (SIL) technique is gaining popularity. The aim of this study is to review our institutional experience in using the SIL technique to surgically manage different splenic pathologies in the pediatric population.
Method: The operation was performed with use of a three-trochar technique either via a single periumbilical using standard laparoscopic canulae or a transumbilical incision using a specially designed multiport device. The operation was performed with use of a standard 5 mm laparoscopic instrument and one reticulated grasper to facilitate retraction. The Ligasure® was used to seal and divide the plenic vessels and splenic parenchyma. After receiving the approval of the Institutional Review Board, we retrospectively evaluated the patients who underwent SIL splenic surgeries from January 2009 to the present. Pertinent data were obtained from the medical records.
Results: Six patients, all female, were identified in the study period. Three patients had spherocytosis, one of whom had a concurrent cholelithiasis. One patient had idiopathic thrombocytopenia purpura. One patient had a 15 cm epidermoid splenic cyst and another had a 13 cm splenic torsion. Four patients underwent splenectomy, one of whom underwent a combined SIL splenectomy/cholecystectomy. One patient underwent splenic cystectomy and omental patching, and one underwent splenic detorsion and splenopexy. The average age of the patients was 10.5 years (5–14 years) and average weight was 40.3 kg (19–66 kg). Mean operating time was 133 minutes (96–180 minutes), including the patient who received the combined procedures. There were no intraoperative complications or conversions to open and the average blood loss was 30 cc (0–100 cc). Diet was initiated on postoperative day 1 in all patients; average time to full oral intake was <2 days. The average length of stay was 3.3 days (1–8 days); the patient with splenic torsion required a longer hospital stay. At an average 8-month follow-up, none of the patients had postoperative complications and all 5 had satisfactory cosmetic results.
Conclusion: A SIL approach to different splenic pathologies in children is feasible and safe, and achieves excellent cosmetic results because the incision is virtually invisible within the umbilical fold. Larger comparative studies are needed to further validate this approach.
Initial Experience with Trocar-Less Single-Incision Laparoscopic Surgery in Infants and Children
Background and Purpose: We started one trocar laparoscopic surgery for gastrostomy, appendectomy, and Meckel's diveticulectomy in 1998. In this method, a scope and one pair of forceps were inserted into one trocar, and we sometimes felt the difficulty in managing the instrument. We developed a new unique trocar-less single-incision laparoscopic surgery (TLSILS).
Patients and Methods: 15 patients, aged 5 days to 17 years, were enrolled. Diseases were congenital intestinal atresia in 1, Hirschsprung related disease (intestinal biopsy) in 1, parasalpingial cyst in 1, Hirschsprung disease (colostomy) in 1, and acute appendicitis in 11. The access system comprising a wrap protector, a newly made disk, and a surgical glove was used. The disk was 7 cm in diameter, silicon made, and contained three 10 mm holes at the center. The wrap protector was set up through an umbilical incision, and the disk was placed over the external ring of the protector, and then a #5.5 surgical glove was installed. The thumb finger of the glove was partially cut, and a CO2 gas insufflation tube was placed. The instruments are inserted through a pin hole at the other finger tip of the glove. In the last 5 cases, one way valves were attached at the finger of the glove for preventing CO2 leak and an acryl window was used for making the instruments' insertion easily.
Results: TLSILS was completed successfully in all cases without conversion to standard laparoscopic approach. The operative time ranged 55 min to 125 min. Postoperative complications were not seen in any case. The cosmetic results were excellent. In the last 5 cases, the amount of CO2 leak was significantly decreased.
Children Evaluate their Postoperative Pain after Conventional Laparoscopic Versus Sils Appendectomy in a Prospective Study
Objective: Single-incision laparoscopic surgery (SILS) is an ambitious minimally invasive approach to avoid visible scarring, but this might be at the expense of an increased postoperative pain due to the performed mini-laparotomy. However, no significant difference in analgesic requirement after conventional laparoscopic (CL) versus SILS appendectomy in children has recently been observed. Therefore, we wondered how children would subjectively rate their postoperative pain after CL versus SILS appendectomy.
Methods: Patients older than 4 years who underwent laparoscopic appendectomy between April and September 2010 were asked by the mentoring nurse to individually rate their pain score at the time of indication as well 8, 16, 24, and 48 hours postoperatively. Depending on the patients' age and compliance, a visual analog scale (VAS; 0–10) or a faces pain scale (FPS; 1–6) was used for quantification. Values assessed by FPS were transformed into VAS to allow an inter-scale comparison. Analgesics were administered regularly or on inquiry of the patient, depending on the individual postoperative course. Data were collected on: age at surgery, BMI, gender, abdominal pain score, presence of umbilical, or shoulder pain as well as vomiting. Data are presented in mean ± standard deviation or percentage tested at a significance level of p < 0.05.
Results: 25 patients (14 female) were included in the study of which 6 underwent SILS and 19 CL appendectomy. Overall mean age at surgery was 11.6 ± 2.8 years and mean BMI was 19.3 ± 3.5 kg/m2, which did not differ between groups. Mean pain score at indication was 3.5 ± 3.4 and 3.9 ± 2.1 for patients that underwent CL and SILS, respectively. There was no significant difference for the individually evaluated pain scores after 8, 16, 24 and 48 hours for CL and SILS appendectomy. Likewise, the frequency of reported umbilical and should pain was similar in both groups. Postoperative vomiting occurred in 10.5% after CL and 33.3% after SILS, which did not differ significantly.
Conclusion: Single-incision laparoscopic surgery is a feasible technique that does not alter the subjective postoperative pain and recurrence in children after common appendectomy, thus encouraging its implementation as a standard procedure in pediatric surgery.
Thorax
Lung Resection using Radio Frequency Ablation in a Porcine Model by Thoracoscopy and Thoracotomy: A Comparative Study
Introduction: Video-assisted minimally invasive techniques are gradually gaining popularity in thoracic surgery. Thoracoscopic lobectomy is a technically demanding procedure requiring both thoracic surgical experience and the dexterity to handle minimally invasive instruments. Despite the recent advances in methods of aerostasis and haemostasis, perioperative bleeding and air leak remain the most common and difficult-to-control complications. At the same time radiofrequency ablation (RFA) is emerging as a promising minimally invasive tool for the treatment of lung malignancies and was proved to provide haemostasis in applied or experimental liver, spleen or renal surgery or trauma, by endoscopic or open technique.
Aim: The aim of this study was to assess the feasibility, efficacy and safety of lingula resection using radiofrequency ablation (RFA) with internally cooled electrodes in a porcine model by thoracoscopy and thoracotomy, confronting the two methods.
Methods: Twelve domestic pigs underwent RFA-assisted lingulectomy, six by video assisted thoracic surgery (VATS, group A), and six by thoracotomy (group B). RFA was the only aerostatic and hemostatic method applied during parenchymal dissection throughout the operation. After the end of the operation the animals returned to their cages and remained under close observation. After 30 days the animals were sacrificed for the study of the macroscopic and microscopic effects of the technique.
Results: RFA-assisted lingulectomy was successful in all 12 animals. No major bleeding, air leak, or other complication was observed and no conversion to open thoracotomy was required in the group A. There was no mortality either during or after surgery. No signs of pneumothorax, blood loss, or infection were observed up to 1 month postoperatively in the minimal invasive group. In the open group, significantly more adhesions and one infection were observed. There was a significant difference in the operating time (shorter in the minimal invasive group A), and a significant amount of adhesions in the group B. The histopathology of the lung revealed three clearly demarcated zone lesions.
Conclusion: Our study demonstrates that thoracoscopic and open lingulectomy using RFA energy is technically feasible. RFA energy is an effective and safe aerostatic and hemostatic method in the porcine model. Between the benefits of the endoscopic technique were the shorter operative time and absence of adhesions in the operating field.
Quantifying Hemodynamic Effects of Pectus Excavatum and Nuss Repair on Right and Left Ventricular Function by High Speed “Cardiovascular Magnetic Resonance Cine-Ssfp-Imaging,” Early Results of the Prospective Berlin-Buch Nuss-CMR Study
Objective: Exercise intolerance in pectus excavatum is known, but true physiological impairment is difficult to prove. Controversial is, whether Nuss improves cardio-pulmonary performance although cardiac relief was reported 2006 by Coln echo-cardiographically. Cardiac nuclear magnetic resonance (CMR) has far less inter-observer variance but postoperative CMR shows severe interferences by ferro-magnetic Nuss bars and investigations are limited by scarce CMR capacities.
Methods: 7/2009–7/2010 51 PE patients of 12.8–42.9y (21.1 ± 8.6, 40 males) with a Haller of 8.3 ± 3.6 (4.3–18.1) and BMI of 20.8 ± 3.6 entered the study and 31 series free of artifacts allowed complete evaluation. This ongoing prospective study quantifies right + left ventricular function by CMR before, 2 weeks, 3 months and 1 year after Nuss. The use of titanium bars (13′–17′) in all patients avoided bar interferences. Cardiac function was assessed by Cine-SSFP-imaging in axial orientation for left ventricular (LV) and right ventricular (RV) function. Phase contrast velocity encoding CMR above aortic and pulmonary valves measured the flows and compared RV and LV stroke volumes (SV).
Results: The right ventricle lies anteriorly and to the right and is predominantly compromised by pectus excavatum (Fig. 1). Thus, right (and left) ventricular ejection fraction and right ventricular stroke volume (SV) are significantly increased 2 weeks (p < 0.001) and 3 month (p < 0.001) after Nuss (similar trend in the few patients 1y pop). Accordingly, right end-diastolic volumes RVEDV (204/189 ml) and right ventricular index RVEDVi are significantly reduced (both p > 0.001 at 3 mo pop) proving better ventricular emptying after Nuss. Moreover, left ventricular mass increased significantly (p < 0.02 at 2 w/3 months) and Haller index decreased from 8.3 ± 3.6 before to 3.1 ± 0.6 after Nuss.
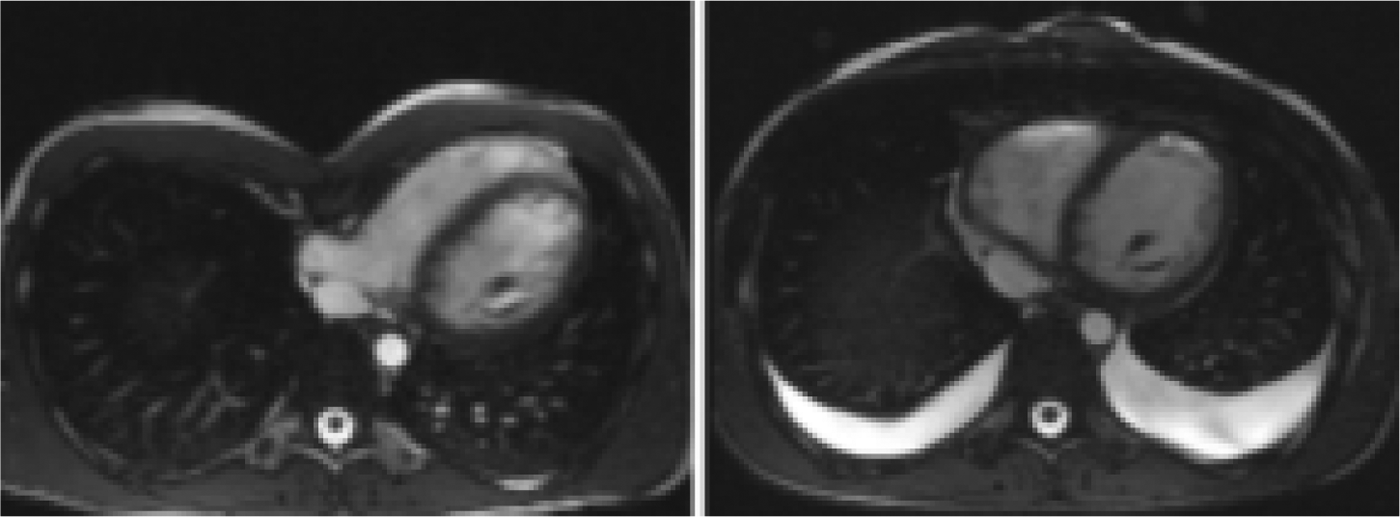
Change of right ventricular shape after Nuss (pleural effusion in 2 wk CMR).
Conclusions: Cardiovascular improvement by Nuss repair has longtime been suspected due to decreased palpitations and exercise heart rates but have never been measured in a strictly reproducible way. Although this is an early report and still a small series, Cine-volumetric CMR measurement shows preoperative impairment in PE and significant postoperative improvement of the most important right and left ventricular morphological and functional parameters after several postoperative periods following Nuss repair. The study is planned for 100 evaluable patients with the last measurement 2 years after bar removal.
Purpose: Thoracoscopy is the preferred method of surgical approach for adults with mediastinal neurogenic tumors. In children there is still controversy regarding the use of thoracoscopy for these kinds of tumors. The aim of this study is to evaluate the efficacy and safety of thoracoscopy resection in children with mediastinal neurogenic tumors.
Methods: With ethics approval we reviewed the case notes of 15 children underwent thoracoscopic resection of mediastinal neurogenic tumors in three different tertiary hospitals, from July 1995 to August 2010.
Results: There were 11 (73%) male and 4 (27%) female, with median age of 16 months (range from 7 days to 12 years old), and median weight of 11.9 kg (range from 3.2 to 55.1 kg). Tumors were neuroblastoma in 9 (60%), ganglioneuroma in 4 (27%) and ganglioneuroblastoma in 2 (13%). The mean length of the operation was 118 ± 67.4 minutes, and all of tumors had complete thoracoscopic resection without need of open conversion. A chest tube drain was left for a mean of 1.2 ± 0.9 days in 10 children (67%); in 5 (33%) it was not necessary any drain. Two children (13%), one with ganglioneuroma and other with ganglioneuroblastoma, presented postoperative Horner syndrome. Hospital stay after surgery was 2.9 ± 1.2 days. There was not death and no recurrence has been noted at median follow-up of 3.6 years.
Conclusions: Thoracoscopy resection of mediastinal neurogenic tumors in children is safe and effective. There have been short hospital stays and no recurrence with minimal postoperative complications. Major advantages of this approach are the avoidance of a thoracotomy and the enhanced surgical accuracy due improved visualization.
The use of High Frequency Oscillating Ventilation to Facilitate Stability During Neonatal Thoracoscopic Operations
Background: Thoracoscopy has become a surgical option for the repair of esophageal atresia and congenital diaphragmatic hernia. Insufflation of carbon dioxide combined with one lung ventilation creates an anesthetic challenge to control acidosis and maintain oxygenation while allowing optimal operative exposure. We have overcome these issues by utilizing the high frequency oscillating ventilator (HFOV) and herein report our early experience.
Methods: We conducted a retrospective review from 2007 to 2010 on neonates who underwent thoracoscopic operation utilizing HFOV. Patient demographics and intraoperative course were reviewed.
Results: In the study timeframe, 17 neonates were identified, 12 with esophageal atresia and 5 with posterolateral congenital diaphragmatic hernia. The mean age at operation was 19 days (range 1–166 days), with a mean weight of 3.1 ± 1.0 kg. Mean gestational age was 37 ± 3 weeks. Prior to surgery, 6 patients (35%) were on conventional mechanical ventilation, and no patient was on high frequency oscillating ventilation. The mean American Society of Anesthesiologist's classification score was 3 (range 3–4). There were no intraoperative complications and mean operative time was 197 ± 72 min. The mean intraoperative ventilator manipulation needed was 3 changes per case. The mean intraoperative pulse oximeter saturation was 97% ± 2%. Intra-operative arterial blood gas data were available in 16 patients, the other had venous sampling. In patients with an arterial blood gas, the mean pH was 7.36 (range 7.18–7.47), mean pCO2 was 41 mmHg (range 25–63 mmHg), and the mean pO2 was 156 mmhg (range 41–426 mmHg).
Conclusion: The use of high frequency oscillator ventilation allows for good intraoperative exposure while allowing excellent oxygenation and elimination of carbon dioxide to prevent acidosis.
First Decades Experience with Thoracoscopic Tracheo-Esophageal Fistula Repair
Purpose: The first thoracoscopic tracheo-esophageal fistula (TEF) repair was performed in March of 2009. This report evaluates the results after the first decade of thoracoscopic TEF repair.
Methods: From March 2000 to September 2010 44 consecutive patients with Type 3 TEF and an additional 6 pts with pure esophageal atresia (EA) were repaired by or under the direct supervision of a single surgeon. Patient weights ranged from 1.2 to 3.8 kg (mean 2.6). 18 patients had significant associated congenital anomalies. The repairs were performed using a three ports. The fistula was ligated using a single endoscopic clip and the anastomosis was performed using single interrupted sutures. Transanastomotic tubes and chest drains were left in all cases.
Results: Forty-nine of the 50 procedures were completed successfully thoracoscopically. Operative times ranged from 50 to 120 minutes (mean 85 minutes) stenosis. There were 2 leaks, one in a TEF and one in a EA, both resolved with conservative therapy. Oral feeds were started on day 4 or 5 in all other patients. ten of 50 patients required dilations (1 to 9), and 17 required a Nissen fundoplication for severe reflux. One patient required a thoracoscopic aortopexy for severe tracheomalacia. All patients are currently on full oral feeds. No patient has any evidence of chest wall asymmetry, winged scapula, or clinically significant scoliosis. There have been no recurrent fistulas.
Conclusion: Thoracoscopic TEF repair has proven to be an effective and safe technique. Initial experience resulted in a higher stricture rate but this improved with experience and changes in technique. The results are superior to that of documented open series and avoid the morbidity of an open thoracotomy.
Thoracoscopic approach for Esophageal Atresia: Own Experience
Purpose: To evaluate the safety and efficacy of the thoracoscopic repair of esophageal atresia (EA) with or without tracheoesophageal fistula (TEF).
Material and Methods: From August 2005 to July 2010, 53 patients (32 boys, 21girls) weighing 900–3900 g underwent thoracoscopic repair of EA with or without TEF. Eight cases were operated in other hospitals in Poland. Two 5-mm and one 2.5–3.5-mm trocars were placed. The 5-mm 25- to 30-degree telescope was preferred. A pneumothorax was maintained with 4 to 6 mmHg. The azygos vein was never divided. The TEF was closed with 5-mm titanic clips or by ligation. The esophageal anastomosis was made over 6–8French nasogastric tube by simple stitches of 5–0 Vicryl tied intracorporally. The chest tube was left without suction. The enteral feeding was usually started on postoperative day 3 or 4. Barium swallow was performed on postoperative day 5 or 6, and then the chest tube was removed.
Results: There were fifty cases with EA and distal TEF, and three cases with EA, long gap and proximal TEF (one was missed during the first operation). All procedures were completed without conversion. Primary esophageal anastomosis was performed in 49 cases and delayed in 2 cases. In one case because of unstable condition only TEF was closed. In three cases with long gap Foker technique was used and in two cases esophageal anastomosis was completed in the second stage also by thoracoscopic approach. One case with severe brain damage was withdrawn from further treatment. There were 10 cases weighted under 1500 g. The average operative time for EA and TEF was 113 minutes (range, 55–245 minutes) with significant improvement after gaining experience. There were two cases of accidental tracheal opening. The anastomotic leak rate was 11.7% (six cases), and all were healed on conservative treatment. Six cases required one to three courses of anastomotic stricture dilatations. There were 8 deaths (15%) of causes not related with performed operation, among them were three cases with Edwards syndrome.
Conclusions: The thoracoscopic repair of EA with or without TEF is effective method, with potential benefits of avoiding thoracotomy. Based on our experience, it is the procedure of choice if performed by an experienced endoscopic pediatric surgeon. The intraoperative complications observed if properly managed have a good prognosis.
Long-Term Outcome following Thoracoscopic Repair of Long-Gap Oesophageal Atresia
Introduction: Few, if any reports describing thoracoscopic repair of long-gap oesophageal atresia (OA) exist. The two senior authors (G.A.M. and F.D.M.) have repaired 5 long-gap OAs using this technique and present their experience.
Methods: A retrospective case-note review of all infants undergoing thoracoscopic repair of long-gap OA was performed to describe outcomes and complications associated with this approach.
Technique: All patients were managed with a Replogle tube and Stamm gastrostomy prior to definitve surgery. A “stressed” contrast study was performed to determine the oesophageal gap. Following tracheal intubation infants were placed semi-prone with the right-side elevated. One 5 mm and two 3.5 m ports were used for access. CO2 insufflation was used to collapse the lung. Plasmakinetic forceps were used to dissect and coagulate the azygous vein. After opening the mediastinal pleura, a stay suture was placed on the upper pouch, which was then mobilised. The lower pouch was mobilised down to the level of the diaphragm if necessary, preserving vascular branches to the oesophagus and vagal trunks. The tips of the pouches were excised and interrupted 5/0 vicryl sutures placed under graded traction to bring the ends together and effect a primary intracorporeal anastomosis over an 8Fr transanastomotic tube. A chest tube was left in situ.
Results: 5 patients at three centres underwent thoracosopic repair of long-gap OA between 2–4 months of age. 4 patients had pure OA and 1 patient had an upper pouch fistula. Pre-operative “stressed” contrast studies revealed gaps of 2.5–3.5 vertebral bodies. There were no conversions and no intra-operative complications. There were two anastomotic leaks, both managed conservatively with the chest tube. 4 patients developed an anastomotic stricture, which was managed successfully with a course of dilatations. Detailed follow-up data was available for 3 patients with 3.5–6 years follow-up. All of these patients were tolerating a normal diet with no restrictions. 2 patients had their gastrostomy closed and the third is awaiting closure. 2 patients underwent laparoscopic fundoplication for refractory gastro-oesophageal reflux and the third is currently awaiting fundoplication. One patient required pyloroplasty for gastric outlet obstruction. No patients required aortopexy. One patient with multiple congenital anomalies in whom the procedure was performed for palliation, subsequently died from their co-morbidity.
Conclusions: Successful repair of long-gap OA using an intracorporeal anastomosis under tension can be safely performed thoracoscopically. All surviving patients in this series had normal tolerance of oral feeds and achieved closure of their gastrostomy providing evidence of good long-term oesophageal function. This technique allows the surgeon to provide linear, horizontal traction between the ends when constructing the anastomosis under tension. An unwanted, unavoidable by-product of the open approach is the inadvertent application of oblique traction as the ends are drawn up into the wound, thereby increasing tension on the anastomosis. The thoracoscopic approach combines the benefits of reduced musculoskeletal morbidity with an avoidance of the need for multiple operations. The excellent visualisation of the distal oesophagus allows precise and extensive mobilisation of the lower pouch reducing risk of nerve and vascular injury.
Thoracoscopic Repair of Congenital Diaphragmatic Hernia in Newborns
Congenital diaphragmatic hernia (CDH) occurs in 1 of every 2000 to 3000 live births and accounts for 8% of all major congenital anomalies. CDH has traditionally been repaired via a thoracotomy. The use of minimally invasive surgery in the neonatal population is increasing. In this report, we describe our initial experience with thoracoscopic repair of CDH.
Materials: Since 2008 35 newborns with CDH were treated through thoracoscopic approach. All patients were stabilized preoperatively and underwent repair in the first days after birth. 11 patients were prenatally diagnosed. All were intubated shortly after birth. 3 neonatal had associated cardiac anomalies. The operation was carried out through three 3 mm throacars approach. Pleural insufflation with carbon dioxide was maintained at a pressure of 2 to 4 mm Hg. The hernia defect was repaired using nonabsorbable interrupted sutures with extracorporeal knots. In case of the large diaphragmatic defect we used the synthetic patch. Chest tube was left in all cases.
Results: The mean age at the moment of operation −1.3 ± 0.3 days. Weight of newborns at operation ranged from 2300 g to 3600 g. Average weight −3150 ± 45 g. Left side CDH were found in 80%. 12 neonates with large defects required closure with a synthetic patch, which was placed thoracoscopically. The average operating room time was 60.2 ± 15.5 minutes (in patients with synthetic patch (SP) −81.0 ± 16.4 min). There were no instances of intraoperative respiratory or cardiac instability. No conversions, even in the need for patch closure. There were no intraoperative complications and mortality. Patients spent an average of 6.9 ± 1.0 days on the ventilator following repair (SP −14.1 ± 4.2 days). The average time until full-enteral feeding was 5.3 ± 2.25 days (SP −7.1 ± 3.2). There were 3 early deaths of patients with cardiac anomalies. In postoperative period 3 chylothorax (SP), 2 hydrothorax, and 1 pneumothorax occurred. All complications were successfully treated. Chest tube was removed on 8.0 ± 2.5 day (on 17.3 ± 4.2 day in SP). Average stay in intensive care unit −7.8 ± 2.1 days (SP −16.2 ± 4.1 days).The mean postoperative hospital stay was 8.7 ± 2.7 days (SP −25.2 ± 4.6 days). There was no evidence of recurrence with a mean follow-up of 379 days.
Conclusion: Thoracoscopic repair of CDH is a safe, effective strategy. It is technically possible to perform thoracoscopic repair with a patch. The rehabilitation of CDH newborns with SP is longer, and more complicated.
The Congenital Diaphragmatic Hernia: Evaluation of Selection Criteria for Thoracoscopic Repair in the Neonatal Period
Objective: Minimal invasive surgery (MIS) gains more and more popularity among pediatric surgeons for the treatment of congenital diaphragmatic hernia (CDH) in the neonatal period. Publications multiply aiming to prove the feasibility and safety of the thoracoscopic approach: some teams use selection criteria, but none have proven statistical evidence. The aim of this retrospective study is to investigate selection criteria for thoracoscopic primary closure of CDH.
Patients and Methods: Since 2006, thoracoscopy with intention to treat has been performed in 29 neonates in 5 centers. The complete prenatal, perinatal, postnatal, operative, and postoperative data of 25 patients could be evaluated. Most of the selection criteria mentioned in the literature have been analyzed for each patient. Two subgroups of patients could be identified: 19 patients have benefited from primary closure, 6 patients required conversion for patch closure or presented major complications after thoracoscopic repair. Statistical tests have been used to compare these two subgroups.
Results: In the first group, thoracoscopic primary repair was performed after postnatal stabilization period in 19 neonates (12 boys, 7 girls). The 6 patients (4 boys, 2 girls) of the second group required conversion for patch closure in 5 cases or died in the immediate postoperative period in 1 case. No statistical difference was found for prenatal diagnosis, gestational age at birth, birth weight and age at operation between these populations. Significant statistical difference was found in the second group for immediate postnatal PaCO2 > 65 mmHg, need of NOi in the postnatal stabilization period, intrathoracic position of the stomach on the first radiographic imaging, presence of pulmonary hypertension signs at the cardiac ultrasound done on the first day of life, and preoperative oxygenation index > 3.5.
Conclusion: CDH can be safely closed in the neonatal period by thoracoscopy. The identification of selection criteria may optimize this approach. Even if thoracoscopic patch closure seems feasible and safe, it involves longer operative times that could threaten the stability of these newborns. With the help of selection criteria, some surgical teams trained in pediatric mini-invasive surgery can make their first attempts in the thoracoscopic repair of neonates with a diaphragmatic defect adequate for primary repair. Prospective studies are nonetheless necessary to validate these selection criteria.
The Role of Thoracoscopic Thymectomy in Juvenile Myasthenia Gravis: Adjuvant or Definitive Therapy?
Background: Thymectomy is a well-established treatment for generalized myasthenia gravis in adults, but predictors of long-term efficacy and the optimum timing for intervention in juvenile myasthenia remain controversial.
Purpose: To review the preoperative presentation, surgical experience, and long-term neuromuscular follow-up in patients undergoing thoracoscopic thymectomy in a single institution.
Methods: A retrospective chart review of all patients undergoing thoracoscopic thymectomy for myasthenia gravis at a tertiary referral center between 2000 and 2010. Age at diagnosis, presurgical medications and hospitalizations, pre-operative chest imaging, presence of acetylcholinesterase antibodies, Osserman Stage, time to operative intervention, length of follow-up, and DeFilippi remission classification, as well as peri-operative and postoperative data (length of surgery, blood loss, need for chest tube, length of intubation, length of hospital stay, pathology, and complications) were recorded.
Results: Fifteen patients were identified with a mean age of 11.2 years at time of diagnosis and an average treatment duration of 12.3 months prior to operative intervention. Of these patients, most presented with Osserman Stage IIB (8) or III (5) disease. Two patients presented with Osserman Stage IIa disease. All were on preoperative Mestinon, 11 (73%) were on steroids, 7 (47%) were receiving IVIG at the time of surgery. Average operative time was 145 minutes with an average estimated blood loss of 21 ml. There were no reported complications, no conversions to an open approach and an average length of stay of 2.6 days. Average length of follow-up was 37.5 months, available on 13 of 15 patients. Nine of thirteen (69%) were improved (DeFilippi Class 2 or 3) at one month follow-up, however the pattern of remission waxed and waned, with only 50% reporting improvement at 1 year, 86% at 2 years and 75% at 3 years. One patient achieved complete remisson off all medication. Although one-third of patients presented with myasthenic respiratory crisis at diagnosis, no patients required ventilation or ICU admission for respiratory crisis after thymectomy.
Conclusions: Thoracoscopic thymectomy offers a safe approach in children with JMG with little morbidity and a short hospital stay, but the role of surgery appears to be adjuvant to long-term medical management, making the disease more amenable to pharmacological treatment and reducing the likelihood of respiratory crisis.
Troubles and Complications in MIS
Complications of Laparoscopic Splenic Procedures in Children
Introduction: The purpose of this study is to analyze the complications of our laparoscopic splenic surgery during the 16-year period—from 1995 to 2010.
Materials and Methods: The total number of 348 pediatric patients underwent laparoscopic splenic procedures:
Laparoscopic splenectomy (LS) was performed in 285 patients (11 months–17 years) for hematologic or non-traumatic splenic diseases. Hematologic indications for LS were hereditary spherocytosis in 169 cases; thalassemia in 31 cases; immune thrombocytopenic purpura in 56 cases; sickle cell disease in 5 patients; and other variants of hemolytic anemias in 15 cases. LS was also performed in 9 patients with benign spleen tumors (hamartoma, 5; lymphangioma, 2; hemangioma, 2). Simultaneous laparoscopic cholecystectomy (LC) for calculous cholecystitis was accomplished in 83 cases (29.1%). 61 patients aged from 1.5 to 17 years with benign non-parasitic splenic cysts (true epithelial–endothelial or mesothelial, 20 (32.8%); pseudocyst, 29 (47.5%); cystic lymphangiomas, 12 (19.7%)) underwent laparoscopic cyst resection. Laparoscopic detorsion and retroperitoneal splenopexy was performed in 2 patients—12- and 14-year-old girls with wandering spleen.
Results
Complications:
Laparoscopic splenectomy (285 patients)
One case (0 < 4%) of conversion due to technical problems with laparoscopic equipment; 3 cases (1%) of early postoperative bleeding: 2 on the first postoperative day; 1 on the second day after LS (caused by acute pancreatitis). Two patients were successfully treated laparoscopically; in one case laparotomy was performed. Postoperative pancreatitis with considerable increase of pancreatic enzimas blood levels took place in 58 patients (20.3%). Nowadays (since 2005) all the patients before LS are premedicated with Octreotide and the frequency of pancreatitis decreased to 4%. A platelet count in 7 children (2.4%) after LS was higher then 1000 in 1 mg. No additional therapy was assigned, and no complications occurred. There were no cases of recurrence of hematologic symptoms caused by surgical problems (splenosis, lost accessory spleens, etc.);
Laparoscopic splenic cyst resection (61 cases):
One case of intraoperative diaphragm injury was treated with laparoscopic suturing. There were 2 cases of recurrence in the patients with cystic lymphangiomas. Laparoscopic splenectomy was performed in these cases. In other 59 patients functional, anatomic, and cosmetic results were excellent (including 10 other cases of cystic lymphangiomas) and there were no indications for any additional treatment during the period of observation from 6 months to 15 years.
Laparoscopic splenopexy (2 cases), no complications.
Conclusion: LS in children provides excellent functional and cosmetic results and is associated with very low complication and conversion rates. LS is undoubtedly our method of choice for all children with benign pathology requiring splenectomy. The patient's age, the splenic size, and the severity of the disease are not the limitations for laparoscopic treatment. Laparoscopic spleen-sparing techniques are safe, effective, and minimally invasive for the treatment of benign non-parasitic splenic cysts and wandering spleen in children.
Laparoscopic Management of Ureteral Complications after Urological Laparoscopic Procedures in Children
Introduction: Laparoscopy may have a place in the treatment of vesicoureteral reflux (VUR) and Pelvi-ureteric junction (PUJ) obstruction as an alternative to open surgery. Laparoscopy combines the advantages of a minimally invasive procedure with the safety and high success rates of the open approach. However, a sometimes laparoscopic procedure fails and redo-procedures may be required. We report our initial experience in Laparoscopic management of ureteral complications after urological laparoscopic primary procedures.
Materials and Methods: Between May 2005 and May 2010, 100 children with PUJ obstruction or VUR were treated by laparoscopy, and were: 63 renal's units in 46 children with VUR, and 54 PUJ obstructions, the mean age was 50 months (2–200 months). These patients underwent Laparoscopic Pyeloplasty in PUJ obstruction and Laparoscopic Extravesical Trans-peritoneal Approach (LETA) in VUR. Laparoscopic approach was feasible in 100% in VUR and 96% in PUJ obstruction. There were three ureteral complications with peritonitis at beginning of series: two ureteral perforations in VUR, and one PUJ leakage. The mean age was 41 months (21–60 months), the mean delay between surgery and reintervention was 9 days (7–15 days). The diagnosis was confirmed by CT-Scan in all cases.
Results: Laparoscopic approach was feasible in 2 of 3 cases. In cases of ureteral perforation, a combined laparoscopic and endoscopic procedure was performed. The JJ stent was placed by cystoscopy and the ureter was sutured by intracorporeal stitches. In case of PUJ leakage, the JJ stent was placed by laparoscopy and the ureter was sutured by intracorporeal stitches. The mean operative time was 12O min. There were no peroperative complications. All patients were feed on the first day. The mean hospital stay was 4 days. Mean follow-up was 18 months (12–30 months). All patients were asymptomatic after removal of the JJ stent.
Conclusions: LP and LETA have been proven safe and effective with comparable results and complications rate similar to open surgery. Complications decrease with the learning curve and the experience to be the key factor to achieve better results. Surgical team experience with incidence and management of complications will be used by next generations of laparoscopic urologic surgeons to shorten their learning curve.
Urology
Intraabdominal Laparoscopy-Assisted “Open” Vessel Ligation: Successful Outcome on Testicular Vessels has Potential Application for Treating Varicocele
Aim: We developed a technique for ligating vessels intraabdominally in a similar fashion to conventional open ligation without the need for complicated maneuvering or clips. We applied our laparoscopy-assisted “open” ligation (LOL) technique to the testicular vessels to assess its efficacy for the surgical treatment of varicocele.
Methods: Twenty male 8-week-old Wister rats were the subjects for this study. In the LOL group (n = 10), a 5 mm trocar was inserted in the epigastrium using the open Hasson technique, and carbon dioxide was insufflated to 3 mmHg. A 0-degree laparoscope was introduced through the epigastric trocar. A 3 mm grasper was inserted in the right lower quadrant without a trocar to expose the testicular artery and vein (TAV) by retracting fat tissue near the left inguinal ring toward the contralateral side. A lapa-her-closure (LHC) needle loaded with 3-0 SurgiPro was inserted directly into the left lower quadrant at the point where the TAV should be, advanced under the vessels, and the suture material released leaving the other end outside the insertion site. The LHC was then withdrawn a little and advanced again, but this time, over the vessels to grasp the end of the suture material just released and bring it outside the insertion site. The 2 ends were then tied as in any conventional open procedure and the knot passed through the insertion site and tightened around the vessels. This whole procedure was repeated again proximally. The scope was then used to confirm that each tie was adequate before the vessels were ligated under laparoscopic control. In the open group (n = 10), laparotomy was performed through a lower midline abdominal incision. The left TAV were ligated with two 3-0 SurgiPro ties, and then ligated between the ties. In both groups, right TAV were left intact. All rats were sacrificed 2 weeks postoperatively, and both testes were examined with hematoxylin and eosin (H&E) to observe if there was necrosis of germinal cells and seminiferous tubules. At sacrifice, the abdominal cavity was also examined macroscopically.
Results: Treatment time ranged from 5 to 7 minutes for the LOL group, and 7 to 8 minutes for the open group. Postoperative recovery was uneventful. Macroscopic examination of the abdomen failed to identify any adhesions between the ligated TAV and the small bowel in any rat. Histopathology of the treated left testis showed coagulative necrosis of the germinal cells and seminiferous tubules in all rats from both groups. No histopathologic changes were observed in the untreated right testes from both groups.
Conclusion: Our technique obviates the need for laparoscopic maneuvers and clips and allows the operating surgeon the comfort of hands-on control. It would appear our technique is as effective as open ligation and recommend it be considered for laparoscopic vessel ligation.
Laparoscopic Pyeloplasty in Children: Evaluation of Safety, Efficacy, and Gastrointestinal Morbidity
Aim: To evaluate the safety and efficacy of laparoscopic pyeloplasty through retrospective analysis of cases performed by a single institution.
Patients and Methods: Fourty three laparoscopic pyeloplasties were performed on 23 female and 18 male (total: 41) patients between 2003–2010. Mean age was 6.5 years (2 months −17 years). The affected side was left in 24, right in 14 and bilateral in 3 patients. Transperitoneal approach was used in all cases, and transmesocolic way was used on left side affected cases if exposition was enough. Ultrasonography was repeated during postoperative period and MAG-3 dynamic renal scintigraphy were repeated 1 year after operation. Gastrointestinal system was evaluated for possible adhesive complication.
Results: All operations were completed without conversion to open surgery. Transmesocolic approach was successfull in 14 of 26 affected left kidney. Dismembered pyeloplasty with limited pelvic reduction was performed in 40 kidneys. Ureteropyelostomy was done in 2 with aberrant vessel and Fenger type pyeloplasty was done in 1 with intrarenal pelvis. DJ catheter insertion succeeded in all cases except 5 in which tube pyelostomy had to be performed. Perirenal urine collection in 1 and renal pelvicalyceal bleeding in another 1 were managed conservatively. Transient hypertensive attack was seen in 1 patient. One patient whose DJ catheter had to be removed on 8th postoperative day because of bladder irritation, developed perirenal urinoma which was treated with percutaneous drainage and DJ catheter re-insertion. The mean postoperative hospitalization time was 3 days (2–8 days). The mean postoperative follow-up was 1.7 years (3 months-7 years). Renal pelvis AP diameter decreased in all patients with a mean of 58% (range: 6–90%). Parenchymal thickness either increased or stayed steady in all patients with mean values of 32.7% (range: 10–75%) and split renal functions increased or stayed steady in all with a mean of 10.8% (range: 1.8–27.5), except one. Although decreased renal pelvis PA diameter, persistent hydronephrosis with signs of obstruction was seen in 2 patients. One of these patients underwent balloon dilatation. There were no gastrointestinal complications related to procedure during followup period.
Conclusion: Laparoscopic pyeloplasty can be safely and efficiently performed in childhood period. Transmesocolic approach can be used in appropriate left side cases. Transperitoneal approach does not cause additional gastrointestinal morbidity.
Laparoscopic Versus Open Pyeloplasty for Ureteropelvic Junction Obstruction in Children: A Systematic Review and Meta-Analysis
Background: Laparoscopic pyeloplasty (LP) is widespread performed for the surgical management of ureteropelvic junction (UPJ) obstruction. However, the true effectiveness and potential advantages of LP in children remains controversial.
Purpose: To comprehensively review the available evidences in the literature on the use of LP versus open pyeloplasty (OP) for UPJ obstruction in children.
Methods: Published studies until the end of July 2010 were searched from Medline, Embase, Web of Science, and Ovid databases, using “pyeloplasty,” “laparoscopy,” and “ureteropelvic junction obstruction” as the search terms, with English language as a limit. A systemic review and meta-analysis was performed using the odds ratios (ORs) for dichotomous variables, and weighted mean differences (WMDs) for continuous variables.
Results: Out of 1381 studies, 8 studies for UPJ obstruction in children were selected for comprehensive review. Two randomized controlled trials (RCTs) and 6 non-RCTs, comprising 674 cases of LP and 7315 cases of OP, met the inclusion criteria. The OP has significantly reduced operative time compared to LP (WMD = 59.00; 95% confidence interval [CI] = 41.15 to 76.85; P < 0.00001), whereas the duration of hospital stay was significantly shorter in the LP group (WMD = −0.40; 95% CI = −0.77 to −0.03; P = 0.03). No difference was observed between LP and OP regarding to overall postoperative complications (OR = 0.97; 95% CI = 0.55 to 1.70; P = 0.90) or the rate of success (OR = 1.66; 95% CI = 0.65 to 4.27; P = 0.29).
Conclusions: LP is a minimally invasive, safe and effective therapy method for UPJ obstruction in children, with shorter hospital stay and excellent outcomes, and without additional risk of postoperative complications. Due to the publishing bias, a series of RCTs are necessary to explore the efficiencies of LP in the management of UPJ obstruction in children.
Retroperitoneoscopic Pyeloplasty in Infants
Aim: To evaluate i) the ability to perform retroperitoneoscopic pyeloplasty in infancy ii) to compare it with retroperitoneoscopic pyeloplasty in older children.
Methods: All patients who underwent retroperitoneoscopic Anderson Hynes Pyeloplasty since January 2005 were studied prospectively the data were collected. The data were subdivided in two groups—Group A: all children under one year of age; Group B: all children above one year of age. The groups were compared and results analyzed.
Results: Since January 2005, 81 children (age 4 weeks to 14 years) (weight 2.5 kg to 42 kg) underwent retroperitoneoscopic Anderson Hynes pyeloplasty. Of these 32 patients (6 right side, 26 left side) belonged to group A and 49 patients (11 right side, 38 left side) belonged to group B. Mean operative time in group A was 128 minutes and in group B was 114 minutes (p > 0.05). Feeding was commenced 12–18 hours after surgery in all patients. There was one conversion to open in group A and none in group B. The mean hospital stay in Group A was 4.2 days and Group B was 3.5 days (p > 0.05).
Conclusion: Retroperitoneoscopic pyeloplasty could be performed equally well in infants as compared to older children. The operative times were comparable. The size of the infant or left side pyeloplasties did not pose any significant technical challenges.
Using Conventional 3- and 5-mm Straight Instruments in Less for Consecutive Pediatric Cases of Pyeloplasty
Background: Laparo-Endoscopic Single-site Surgery is still mainly limited to a few relatively simple procedures in pediatric surgery. We performed LESS pyeloplasty in consecutive hydronephrosis in children with conventional straight instruments and ports. The peri-operative data were reviewed in these cases to evaluate the technical feasibility.
Methods: From Dec. 2009 to Aug. 2010, there are 22 consecutive cases of hydronephrosis, with mean age of 56.9 months (2–134); 18 of them were boys, the other 4 were girls. Twelve of them were presented with recurrent flank pain, the others were detected by ultrasound. All were investigated with isotope renograph and ultrasound. For surgical technique, a semicircle incision was made on the circumference of the umbilical ring. Three conventional ports were inserted inside this incision, one 5 mm for camera and two 3 mm for instruments. Conventional laparoscopic instruments and 30 degree camera were used for Anderson-Hynes pyeloplasty. A F4.7 or F3 pigtail stent was introduced through one of the instrument port. A drainage is placed beside the anastomosis, and comes out from the umbilical ring incision. The stent was removed 6 weeks postoperatively.
Results: All cases were successfully completed with no need for extra-umbilical incision. The mean operative time is 198 min (150–270). All could tolerate oral food intake on postoperative day 1. Of the 20 cases who have had the pigtail stent removed 6 weeks postoperatively, 1 (5%) developed symptoms of anastomosis obstruction and a renal stoma was placed through the flank incision. No other significant complications occurred in all cases.
Conclusions: LESS pyeloplasty is technically feasible in children. Using 3- and 5-mm ports and instruments is a viable option over the expensive multi-channel single port and bent or articulating instruments.
Outcomes of Robotic Ureteral Reimplantation after Failed Deflux Surgery
Background: Surgical options for correcting vesicoureteral reflux continue to grow. Robot-assisted laparoscopic (RAL) ureteral reimplantation is a newer approach and its utilization continues to grow. A critical eye should be used to assess the success of new surgical techniques. One important focus is success rates when prior surgery has failed.
Objective: After receiving institutional IRB approval, we performed a retrospective chart review of extravesical RAL ureteral reimplantations performed at our hospital between October 2007 and May 2010. We compared the operative times and success rates in patients with no prior surgery compared to the patients who had prior Deflux surgery.
Results: A total of 17 cases (23 ureters) were performed between October 2007 and May 2010. Of these cases, 4 patients (5 ureters) had prior, but failed Deflux injection. T-tests and chi-squared tests were run to compare age at surgery, length of stay, operative times and resolution on follow-up x-rays. Mean age for patients with no prior surgery (group A) was 6.5 years versus 5.2 years in the patients with failed Deflux population (group B). Length of stay was similar in both groups at 1.31 days versus 1.25 days (Group A versus B). Length of follow-up was 14.8 months versus 13 months (Group A versus B). The amount of time for docking the robot was similar at 2 hours and 4 minutes versus 2 hours and 12 minutes (Group A versus B). The resolution rate on follow-up voiding cystourethrogram (VCUG) was 89% versus 100% in groups A and B, respectively.
Conclusion: Although our series is very small, it is encouraging. As with any new technique, it is important to understand success rates in multiple scenarios. Intuitively, we expected prior Deflux surgery to make the tissue dissection more challenging. We expected prior surgery to cause longer operative times and possibly lower success rates. It is exciting that the 4 patients (5 ureters) with prior Deflux surgery had high success rates and comparable operative times. RAL ureteral reimplantation provides another minimally invasive surgical technique for correction of reflux. We understand the strength of studies with a prospective design. Therefore, we are conducting a prospective study to analyze outcomes of Deflux, open ureteral reimplantation, and RAL ureteral reimplantation.
Transvesicoscopic Cross-Trigonal Ureteroneocystostomy in Children: A Single Center Experience
Purpose: To evaluate the safety and efficacy of transvesicoscopic ureteric reimplantation technique in children.
Patients and Methods: Seventeen ureteric units in eleven patients underwent transvesicoscopic “Cohen” ureteroneocystostomy between years 2003 and 2007, and the results were retrospectively analyzed. There were 4 boys and 7 girls. All patients had vesicoureteric reflux, except one with paraostial diverticula. Six patients underwent bilateral, and 5 patients underwent unilateral transvesicoscopic reimplantation (a total of 17 units).
Results: Transvesicoscopic procedure was successfully completed in all patients. Mean operation time was 3.6 hours in unilateral and 5.1 hours in bilateral cases without perioperative complications except pneumoperitoneum development in two cases. In early postoperative period, two patients developed macroscopic hematuria. Mean hospital stay was 3.8 days (3–5 days) except for one patient who suffered from urinary tract infection and needed longer hospitalization. Mean follow-up period was 4.5 years (3–7 years). Only one patient with bilateral vesicoureteral reflux had passive unilateral grade I vesicoureteral reflux on postoperative cystogram with a success rate of 92% (94.2% of ureters). That patient did not have clinical complaints and was followed conservatively. One patient has also recurrent urinary tract infections without reflux.
Discussion: Transvesicoscopic cross-trigonal ureteroneocystostomy can be safely performed with high success rate in children.
Retroperitoneal Laparoscopic Adrenalectomy for Adrenal Tumor in Children
Abstract Withdrawn
Treatment of Pediatric Varicoceles: A Comparative Study of Laparoscopic Varicocele Ligation with Palomo and Ivanissevich Technique
Purpose: We evaluated our experience in the treatment of male children with varicoceles using laparoscopic varicocele ligation and investigated the effect of two different surgical technique: Palomo and Ivanissevich retrospectively.
Methods: Between January 2005 and January 2010, 36 children with varicoceles were treated with laparoscopic varicocele ligation in our department. All patients underwent laparoscopic treatment of unilateral varicoceles. They were divided into Palomo group and Ivanissevich group. Palomo group included patients who underwent ligation of testicular veins and artery but Ivanissevich group underwent ligation of veins alone. Testicular volume was evaluated by ultrasound measure before the treatment and during the follow-up.
Results: Patient ages ranged from 9 to 15 years. There were 22 patients in Palomo group and 14 patients in Ivanissevich group. The average operation time was 59 ± 8 minutes in Palomo group and 60 ± 11 minutes in Ivanissevich group. In Ivanissevich group, dilated spermaductus associated veins were ligated together with the main testicular vessels in two patients. All patients were discharged in 24 to 48 hours hospital stay after the surgery. There were no technical failures. No obvious scrotal edema developed in all patients. At an average follow-up of 24 months (range, 8 to 36), 30 patients were asymptomatic and had marked reduction in the size of the varicoceles. During the follow-up, two recurrent varicoceles were identified in both groups. Slight hydrocele was developed in two patients in Palomo group and being observed due to the small size. We found no testes had obvious catch-up growth and also no evidence of testicular atrophy after surgery according to the ultrasound measure.
Conclusion: Laparoscopic varicocele ligation is a mini-invasive surgery with a highly successful and safe method to treat varicoceles in male children. There were no difference between the Palomo technique and Ivanissevich technique in the treatment of varicocele. Further experience and long-term follow-up are required.
Meta-Analysis of Lymphatic Sparing Versus Lymphatic Non-Sparing Varicocelectomy in Children and Adolescents
Background: Lymphatic sparing varicocelectomy (LSV) is emphasized for the surgical repair of varicocele. However, the true effectiveness and potential advantages of LSV over lymphatic non-sparing varicocelectomy (LNSV) in children and adolescents remain exclusive.
Methods: Published studies until August 31, 2010, were searched with the terms “lymphatic sparing varicocelectomy,” “varicocele,” “adolescent,” and “children” from Medline, Embase, Ovid, Web of Science, and Cochrane databases. Randomized controlled trials (RCTs) and observational clinical studies (OCSs) with a comparison of LSV and LNSV were included. A systemic review and meta-analysis was performed using the odds ratios (ORs) for dichotomous variables.
Results: Out of 117 studies, two RCTs and six OCSs were eligible for inclusion criteria, comprising 609 cases of LSV and 399 cases of LNSV. The hydrocele (OR = 0.16; 95% confidence interval [CI] = 0.09 to 0.29; P < 0.00001) and testicular hypertrophy (OR = 0.09; 95% CI = 0.03 to 0.29; P < 0.0001) rates of LSV were significantly less than those of LNSV. However, no significant difference was observed between LSV and LNSV in the recurrence (OR = 0.69; 95% CI = 0.35 to 1.37; P = 0.29) or catch-up growth (OR = 1.84; 95% CI = 0.90 to 3.80; P = 0.10).
Conclusion: LSV is valuable in reducing the postoperative hydrocele and testicular hypertrophy, with similar recurrence and catch-up growth rates with LNSV. Due to the publishing bias, a series of RCTs are necessary to explore the efficiencies of LSV in the management of varicocele in children and adolescents.
Video Abstracts
Cool Tricks
Left Transaxillary Esophageal Lengthening for Short Esophagus
The management of complicated gastroesophageal reflux in children includes the patient with a shortened esophagus. This condition, thought for some years to be congenital, is acquired, and can be the result of any process that subjects the distal esophagus to a chronic inflammatory process. Examples of this include not only chronic untreated GERD, but also such conditions as giant paraesophageal hernia, esophageal atresia, repeated fundoplications, and longstanding pulmonary lower lobe chronic inflammatory processes usually treated surgically.
Management of GERD with fundoplication in these situations requires lengthening of the esophagus. Failure to address this length issue will result in excessive tension and subsequent failure of the fundoplication. One solution to lengthening the esophagus is Collis gastroplasty. Lengthening the esophagus using this technique involves moving the GEJ and the angle of His distally. Using this technique allows the acquisition of approximately 6 cm of additional esophageal length using a portion of the lesser curvature of the stomach. The approach as described by Collis utilizes a thoracic approach. The utility of this approach is the mechanical advantage of creating the neoesophagus from superior to inferior. This lengthening maneuver is not easily accomplished from the abdomen.
This video illustrates the combination of the abdominal and thoracic approaches to make this maneuver easier and, using a minimally invasive technique, avoiding an open thoracotomy.
Laparoscopic Single-Stage Radical Colpohysterectomy and Vaginal Replacement in a Persistent Rhabdomyosarcoma
Introduction: Multimodal treatment of rhabdomyosarcoma arising in the female genital tract includes systemic chemotherapy, as well as surgery and/or radiotherapy for local control. Providing that this management carries a 5-year survival in excess of 80% and survival into adolescent and adult life is becoming more commonplace, doing a reconstructive procedure at the time of radical surgery is an option The aim of this video is to present the technical details and tricks used in a laparoscopic radical treatment of a uterovaginal rhabdomyosarcoma and simultaneous vaginal replacement.
Case presentation: A 16-month-old girl presented with a botryoid tumor arising from the upper vagina. Debulking of the tumor under vaginoscopy was diagnostic for embryonal rhabdomyosarcoma. Staging studies excluded the presence of distant disease. Because of concern of microscopic residual disease we classified her as group II A according to the IRSS. This treatment schema calls for 10 weeks of 3 agent multiagent chemotheraphy followed at week 13 by local control maneuvers. No evidence of gross residual disease was observed but vaginoscopic histologic sampling of upper vagina and cervix was positive for neoplasic cells.
Operative technique: The patient received preoperative bowel preparation and perioperative intravenous antibiotics. We used a 4 mm 30 degree lens; two 3 mm working ports in each lateral quadrant; and a 5 mm suprapubic one for the bipolar sealer. The surgeon stood on the left. The infundibulopelvic ligaments with ovarian blood supply were kept intact and the uteroovarian ligaments sealed and cut to start uterine resection. The round ligaments were divided. The uterine vessels were then sealed and divided. The uterus was gently manipulated developing the paravesical and pararectal spaces and dissecting the vagina from the bladder caudal to its mid portion. There were no visible lymph nodes. A combined perineal dissection was used to complete vaginal resection, starting with a circunferencial dissection of the distal vagina to the point where it could be everted extracting the specimen through the perineum, which was sent for frozen section evaluation. A balloon catheter was used in this space to maintain the CO2 intrabdominal pressure. A segment of distal sigmoid was isolated creating the mesenteric windows of the selected piece of bowel using the linear stappler sutures inserted through the perineal dissection In this way we use the space created for the neovagina as a natural orifice to introduce a 12 mm port and stappler (NOTES concept) achieving better cosmetic results. The proximal transected colon was also exteriorized through this space to introduce the envil of the circular stappler and reintroduced into the abdomen afterward. Colo-colonic continuity was reestablished using a circular mechanical suturing device introduced through the rectum. The vaginoplasty was completed from the perineal side using 5/0 absorbable sutures.
Results: Operative time was 300 min. The patient was discharged home on the fifth postoperative day. Follow-up imaging, performed 17 months after surgery, demonstrated no evidence of disease. She is just starting to be toilet trained with no evidence of urinary incontinence.
Gastrointestinal & Hepatobiliary
Laparosopic Resection of Gastric Giant Cavernous Hemangioma in a Child
Introduction: Gastric hemangioma in children tends to be rare; there are just a few cases previously reported. Upper gastrointestinal bleeding is the most common symptom; this could be severe and life threatening. All the cases reported had been treated by gastric resection, which had been done through an open approach. We present a case report of one child with giant gastric hemangioma treated by laparoscopic approach.
Case report: A 7-year-old boy who suffered from hypovolemic shock with hematemesis and melena had a hemoglobin level of 4.3 g/dL when admitted. He was transfused and afterward became hemodynamically stable. An endoscopy was performed resulting in consistent findings of hemangioma in the gastric fundus without affecting the esophagus. An angioresonance showed a vascular malformation covering the fundus of the stomach. The procedure was carried out using a 4-port laparoscopic approach. The setup was the same used for the esophageal surgery. Observing a large cavernous hemangioma located in the anterior and upper gastric fundus, we proceeded to release the short gastric vessels; afterward, we performed an intraoperative endoscopy to exclude involvement of the gastroesophageal junction. Then, it was resected with a harmonic scalpel and reconstructed the stomach with two layers of 2-0 silk suture. Throughout the procedure there were no intraoperative complications. Surgical time lasted around 90 minutes. The postoperative period was uneventful. The nasogastric tube was withdrawn on the second postoperative day, shortly after the patient started a liquid diet. The patient was discharged from the hospital on the fifth day after the surgery. The histopatologic report stated gastric cavernous hemangioma. An actual follow-up of 6 months has shown no recurrence of bleeding.
Discussion: Gastric hemangiomas as a very rare disorder in children usually manifests bleeding that may be severe as it happened with our patient. Due to the irrigation of the stomach, some forms of treatment such as embolization are not always possible leaving the resection as the only option. Most of these treatments are carried out conventionally; however, in this case we were able to perform the resection of giant hemangioma through laparoscopic approach achieving a more rapid recovery of the patient. The use of harmonic scalpel allows a better control of the bleeding; as well intraoperative endoscopy outlines the extent of the injury which makes it possible to perform a better gastric reconstruction.
Laparoscopic Resection of a Primary Retroperitoneal Teratoma
Introduction: A 15-year-old girl presented after several months of vague abdominal pain to a peripheral emergency department and was diagnosed by abdominal sonography with a retroperitoneal mass of unknown etiology. Despite ancillary magnetic resonance imaging and serologic analysis a definitive etiology was not established. The child was referred to pediatric surgery for assessment of a suspected adrenal mass versus duodenal duplication cyst. Surgical resection was recommended for definitive diagnosis and treatment and a laparoscopic approach was selected.
Methods: The procedure was approached with a laparoscopic technique using 3 ports, two 5 mm ports in the left upper and right lower quadrants and a transumbilical 10 mm port. The duodenum was mobilized via a partial laparoscopic Kocher maneuver exposing the lesion and its intimate association with the abdominal great vessels. Direct and magnified visualization provided by the laparoscope allowed the use of hook cautery and sharp dissection in order to free the lesion from the adventitia of the IVC and juxtareanal abdominal aorta. An endocatch retrieval bag was used to extract the lesion, intact, via the umbilical incision.
Results: The patient recovered well and was discharged home. She had complete resolution of her abdominal symptoms. Follow-up revealed no recurrent or residual lesion and near imperceptible cosmetic results. Final pathologic analysis confirmed a mature teratoma without evidence of dysplasia.
Conclusion: Laparoscopic resection of a primary retroperitoneal teratoma is feasible and safe in the pediatric patient. It should be considered as an alternative approach to an exploratory laparotomy for resectible retroperitoneal masses with potentially less morbidity.
Placement of a Permanent Gastric Electrical Stimulator
This video depicts the case of a 15-year-old male with severe gastroparesis implanted with a permanent gastric electrical stimulator. This technique has been used on approximately 25 patients at our institution. This video depicts the technique and we discuss the implantation during the video.
Miscellaneous
Laparoscopic Resection of a Right Adrenal Pheochromocytoma
Purpose: To describe the technique of laparoscopic right adrenalectomy for a pheochromocytoma.
Methods: A 17-year-old male with persistant hypertension was diagnosed with a right adrenal pheochromocytoma. After undergoing pre-operative treatment with propranolol and phenoxybenzamine the patient underwent a laparoscopic resection. The patient was placed in a modified left lateral decubitus position with the right side elevated 45 degrees. Four 5 mm ports were used for the procedure. Dissection was accomplished primarily with the Ligasure Force Triad (Covidien, Boulder, Co) and monopolar hook cautery.
Results: The procedure was completed successfully laparoscopically. Operative time was 90 minutes. Tumor manipulation was minimized until the draining vein was ligated. The patient had an uncomplicated post-operative course and was discharged on the third post-operative day.
Conclusion: Laparoscopic resection of an adrenal pheochromocytoma is a safe and effective technique given the appropriate pre-operative preparation.
Robotics
Robotic Resection with Roux-En-Y Reconstruction of a Choledochal Cyst with a Long Common Bile Duct/Pancreatic Cuct Common Channel
A 21-month-old girl presented with acholic stools, jaundice, and mid-epigastric/right upper quadrant abdominal pain. Her liver function tests were elevated including a total bilirubin of 11, amylase of 575, and lipase over 4000. A CT scan at an outside institution demonstrated a dilated intra and extra hepatic biliary system with a long common channel from the confluence of the common bile duct and pancreatic duct. A significant amount of sludge was present. An ERCP was successful which decompressed the sludge from the bile system and a stent was placed. Her bilirubin and other laboratories returned to normal soon thereafter but the dilatation persisted. Over the next several weeks, she did well and eventually underwent an elective robotic resection of her choldochal cyst with a roux-en-y choledochaljejunostomy reconstruction and stent retrieval. The procedure was performed using the da Vinci Surgical robot (Intuitive Surgical, Sunnyvale, CA) and four 5 mm ports and one 12 mm port. We began the procedure using the 8.5 mm 3D HD scope at the umbilicus and resected the cyst robotically and removed the stent. The Roux limb was constructed by first marking the bowel with vicryl sutures and then undocking the robot and eviscerating bowel through the umbilical site after extending this site to a 12 mm size. A hand sewn jejunojejunostomy was created extracorporeally and then dropped back into the abdomen and the abdomen reinsufflated. The robot was then used to construct the choledochaljejunostomy. She had no complications and has remained asymptomatic following the procedure. We present a video demonstration of this robotic operation.
Single-Incision Laparoscopic Surgery
Single-Port Laparoscopic Adrenalectomy
Introduction: Single-port laparoscopy is an exciting technique that has been successfully employed for many common abdominal procedures. However, its utilization for retroperitoneal tumors has been less widespread. This video demonstrates a single-port laparoscopic adrenalectomy.
Methods: The patient is a 16-year-old girl (49 kg) who was found to have a 3.2 cm calcified mass in the right adrenal gland during work-up for scoliosis. At operation, an ACS Triport was placed in the right subcostal location. A 5-mm, 30-degree endoscope and two 5-mm straight working instruments were used for dissection. A 5-mm retractor was placed in the epigastrium to retract the liver. The main adrenal vein, superior vascular pedicle, and inferior vascular pedicle were identified and ligated using a 5-mm clip applier. The adrenal gland was removed intact.
Results: The operative time was 124 minutes. There was minimal blood loss. The patient started a liquid diet the night of surgery. She was discharged to home on the third postoperative day. The pathology revealed ganglioneuroma. No further treatment was needed.
Conclusion: Single-port laparoscopy can be used successfully in the management of tumors of the retroperitoneum. Advantages, such as improved cosmesis, are beneficial in the pediatric population.
Single-Site Laparoscopic Intussusception
This video will present a technique of single-site laparoscopic reduction of intussusception. The procedure is performed in a 5-month-old child who had a failed pneumatic reduction. The procedure was performed entirely with reusable 3.5 mm instruments and trocars.
Single-Incision Laparoendoscopic Ovarian Cystectomy for a 22 cm Serous Cystadenoma in an Adolescent Female
Single-incision laparoscopic surgery (SILS) has developed as an alternative to many surgical procedures in an effort to reduce postoperative pain and abdominal scarring. Limitations to application of this surgical approach in pediatric patients are due to a lack of surgical expertise as well as the need for specialized instruments. We describe a patient in whom an excision of a large ovarian serous cystadenoma was performed through a single transumbilical incision using conventional laparoscopic instruments. The patient is a 16-year-old female who presented with a presumed pregnancy due to progressive lower abdominal distention. Ultrasound and CT imaging showed a large 22 cm cystic mass arising from the right adnexa. Alpha-fetoprotein and beta-HCG levels were within normal limits. Through a 2 cm transumbilical incision, 7 liters of serous fluid were aspirated from the cyst. The puncture site was oversewn and the cyst wall was placed back within the peritoneal cavity. Ovarian preserving cystectomy was then performed. Our operative time was 70 minutes. There were no intraoperative complications. The patient recovered uneventfully and was discharged home the following day. Postoperatively, there were no complications and no visible scar was identified. In conclusion, cystectomy for benign lesions of the ovary can be safely performed through a single transumbilical incision with standard laparoscopic instrumentation. The procedure is also technically feasible and confers an excellent cosmetic result.
Miller Children's Hospital
Purpose: Splenic torsion is a rare condition in children. Surgical treatment can be a challenge and, traditionally, requires a laparotomy or a standard laparoscopy using multiple incisions. We wish to report our case of splenic torsion managed with single-incision laparoscopic splenopexy.
Methods: The operation was performed with the patient positioned at a 30-degree left side up on a Bean Bag. A transumbilical incision was made and a specially designed multi-port device was inserted. The spleen was detorsed with laparoscopic instruments. A “U” shape was made in a 20 × 25 cm mesh. The mesh was placed around the splenic hilum as a sling and stapled to the lateral abdominal wall using the hernia tack device.
Results: The total operative time was 123 minutes. There were no intraoperative complications and blood loss was minimal. A mini-grasper through a stab incision was needed to help reduce the spleen due to it extremely large size. The patient was started on PO intake on POD#1 and advance to normal diet on POD#2. She was discharged on POD#8. At a six month follow-up, the patient is doing well without complication and has a viable spleen per ultrasound.
Conclusion: SIL approach to complex splenic disorders such as splenic torsion is technically challenging but is feasible and offers a cosmetically superior incision to standard techniques.
Thorax
Right Thoracoscopic Approach to Ea/Tef with Aberrant Right Subclavian Artery
A newborn male with VACTERL association was diagnosed with esophageal atresia, distal tracheoesophageal fistula, and high imperforate anus. Preoperative echocardiographic assessment showed normal arch anatomy but with an aberrant right subclavian artery with origin from the left-sided descending aorta. The infant underwent diverting colostomy and thoracoscopic repair of esophageal atresia.
The operative findings during esophageal repair included
Right thoracoscopy provided excellent exposure.
The upper esophageal pouch ended blindly at the level of the subclavian artery that was crossing from left to right.
There was no limitation or challenge presented by the presence of the aberrant right subclavian artery.
Repair of the esophageal atresia and tracheoesophageal fistula using primary handsewn anastomosis using standard MIS techniques was achieved without difficulty.
Postoperatively, there was no leak or other complication of this procedure. There were no airway or anesthetic problems related to the subsequent posterior sagittal anorectoplasty or subsequent reversal of diverting colostomy. Currently, the child is 9 months of age and thriving. This case video nicely demonstrates the anatomic relationships between the aerodigestive and vascular structures in this congenital anomaly.
Thoracoscopic Segmentectomy for a Congenital Arterio-Venous Malformation in the Superior Segment of the Right Lower Lobe
Purpose: To demonstrate the technique of segmental resection of the lung in the case of a giant arterio-venous malformation in the right lower lobe in a 5-year-old, 16-kg girl.
Methods: Following left mainstem intubation the patient was put in a left lateral decubitus position. Three ports were used to perform the procedure. A pre-operative MRI showed the AVM appeared to be confined to the superior segment of the right lower lobe with a large feeding vessel coming directly off the pulmonary artery and venous drainage directly into the superior pulmonary vein. The procedure was started by completing the posterior aspect of the major fissure and identifying the superior segment artery, which was sealed and divided. The Draining vein was then identified in the fissure and mobilized and divided with an endoscopic stapler.
The lung parenchyma was then divided along the segmental plane between the apical and basal segments using the Ligasure Force Traid (Covidien Energy based Devices, Boulder, CO) The segmental bronchus was divided sharply and closed with 3-0 PDS suture and the feeding arterial branch was divided with the endoscopic stapler.
Results: The procedure was completed successfully thoracoscopically. Blood loss was less the 20 cc. The operation took 140 minutes. The chest tube was left in for 4 days because of persistent serous drainage. The patient was discharged on the 5th post-operative day. Follow-up MRI at 6 months shows complete resolution of the AVM with no evidence of recurrence.
Conclusion: Thoracoscopic segmental lung resection for congenital lung lesions is a safe and viable technique.
Thoracoscopic Patch Repair of a Left-Sided Congenital Diaphragmatic Hernia in a Neonate
Introduction: Congenital diaphragmatic hernias (CDH) have traditionally been repaired via an open laparotomy or thoracotomy. In recent years, minimally invasive CDH repair has been shown to be equivalent to the open operation. At our institution, thoracoscopic repair has become our preferred approach for neonates requiring minimal ventilatory support. In this video, we present a thoracoscopic repair using a Gore-Tex patch for a left sided Bochdalek hernia in a 3-day-old infant.
Methods: A full-term male infant, with an antenatally diagnosed left sided congenital diaphragmatic hernia, was intubated immediately after birth. APGARS were 7 at one minute and 8 at five minutes. The initial venous pCO2 was 56 and oxygen index was 4. The infant was weaned on the ventilator and had an oxygen index of 2 and PIP of 24 on the morning of surgery. Babygram demonstrated the stomach and numerous loops of small bowel to be located in the chest. The hernia repair was approached thoracoscopically, and after reduction of the viscera, the infant was noted to have absence of diaphragm laterally. A thoracoscopic left CDH repair was performed utilizing a 2 mm Gore-Tex patch. Prior to inserting the patch, 2-0 Tevdek sutures were pre-placed on the anterior and lateral leaflet of the Gore-Tex. The patch was inserted through the 5 mm trocar site and the pre-placed sutures were retrieved with an Endoclose device and tied around a corresponding rib.
Results: The patient's post-operative course was uneventful. He was extubated on post-operative day three and started on enteral feeds on day 5.
Conclusions: Thoracoscopic patch repair of congenital diaphragmatic hernias in neonates is feasible and can be done safely as demonstrated in this video. We believe pre-placing sutures on the anterior border of the Gore-Tex patch, prior to inserting it into the chest, saves time and allows for a more uniform repair of the defect. Patients with CDH defects requiring a patch closure should be considered for thoracoscopic repair.
Educational/Technical points: In this video, we describe and demonstrate the technical points utilized for performing a thoracoscopic patch repair of a left sided congenital diaphragmatic hernia.
Robotic Thymectomy
An 8-year-old girl presented with severe weakness. Work-up revealed myasthenia gravis and she was treated with Mestinon. However, she had a severe relapse on 2 additional occasions but these occurrences were more severe requiring intubation. Steroids were added to her medical regimen and eventually her overall symptoms improved. She was referred to our institution and a total thymectomy was planned. We performed a robotic total thymectomy using the da Vinci surgical robot (Intuitive Surgical, Sunnyvale CA) approaching the thymus through the left chest using a 12 mm camera port and two 5 mm robotic instrument ports. We present a video demonstration of this robotic thymectomy.
Urology
Laparoscopic Mitrofanoff Continent Stoma
Introduction/Objective: The continent apendicovesicostomy described by Mitrofanoff is widely used in patients with voiding dysfunctions to provide urinary continence and an easier way for catheterization. The laparoscopic approach for this procedure has been recently described and still remains a quite new technique. In this video we show a modification of previous laparoscopic techniques using only 3 port pneumovesicum and transabdominal stitch.
Patient and Methods: A 12-year-old boy with diagnosis of Prune Belly syndrome and history of posterior urethral valve, previously resected, with bilateral vesicoureteral reflux (VUR).
Bilateral ureteal reimplantation.
Secondary voiding dysfunction with augmented capacity (1270 ml) and post void residual urine associated with recurrent urinary tract infections (UTI). A three trocar approach was decided. We used a 10 mm umbilical trocar and two 5 mm trocar in the right and left flank. Monopolar energy was used for the dissection of the mesoapendix. The tip of the appendix was exteriorized trough the right flank incision. An 8 FR catheter was inserted to clean the lumen of the appendix with a idodinepovidone solution.
The anterior wall and dome of the bladder were dissected using monpolar hook and blunt dissection, then a submucosal tunnel was created using monopolar hook dissection. The bladder was filled with CO2 at 12 mmHg trough a previously inserted Foley catheter to assist the dissection.
The base of the appendix was ligated using two extracorporeal Roeder knots and then divided. A hole was made in the vesical mucosa at the distal end of the submucosal tunnel. A transparietal stitch was used to hang the bladder and appendix together to facilitate the anastomosis. The appendix base was sutured to the vesical mucosa using interrupted Polidyoxanone (PDS) stitches with intracorporeal knots. The submucosal tunnel was then closed over the appendix using extracorporeal Roeder knots of the same material. The tip of the appendix was then exteriorized trough the 10 mm umbilical trocar and the umbilical anastomosis was finished in the same way as conventional surgery.
The mean operatory time was 180 minutes. Discharge was made at the second postoperative day. No complications were recorded during the surgical procedure.
Conclusions: Laparoscopic Mitrofanoff is feasible. More experience with this new procedure is required to reduce mean operatory time.
Poster Abstracts
Basic Science
Modification of the F.L.S® Training-Box for Pediatric Surgery
F.L.S® training program has showed short- and long-term efficiency for surgical skill training. However, skills and size have been studied for adult surgery. In case of paediatric surgery, the surgeon is forced to work in a reduced space with very short distance between ports and using smaller devices in size and diameter. To improve F.L.S efficiency for paediatric surgeons, the authors through collaboration between surgical simulation team and laparoscopic paediatric surgeons have adapted the F.L.S training box for paediatric surgery.
Main modifications were
a 3.15 and 4.7 inch distance between ports insertion using 3 to 5 mm ports
a total working space limited to 7.8 × 7.8 × 6 inches
the introduction of a tube between the two ports to mimic camera's place and risk for collision instruments
the use of paediatric surgery stiches (5/0–6/0) for exercises
the possibility to tilt the support for plots, penrose drain
Theses modifications should allow developing specific training support and curriculum for paediatric surgeons.
Histomorphologic Evaluation of Rabbit's Soft Tissue Changes on Implantation of Polytetrafluoroethylene Diaphragmatic Patch (“Ecoflon,” Sankt-Peterburg, Russia)
Background: The repair of large congenital diaphragmatic defects in the neonate continues to be a challenge. Different types of synthetic patches are used for closure of large diaphragmatic defect in congenital diaphragmatic hernia. Polytetrafluoroethylene (PTFE) is the synthetic material most widely used for reconstruction in instances of partial and complete diaphragmatic agenesis. New synthetic PTFE patch “Ecoflon” was invented with two different functional surfaces. Textural macroporous surface through which the connective tissue is growing helps to fix and stabilize patch. And the smooth microporous surface which provides the minimum germination of a connecting tissue and protection from adhering.
This study evaluates the novel material for use in diaphragmatic reconstruction on growing rabbits.
Materials: 18 growing rabbits were anesthetized and underwent laparotomy. The mean age of animals was 3.1 ± 0.7 month. PTFE “Ecoflon” patches were sutured circumferentially with 6-0 prolene to parietal peritoneum. All animals survived the operation, and were killed at days 15 (9 animals) and 30 (9 animals) postoperatively. Histological examination of the patch was performed in each animal.
Results: Histology findings showed the following:
“Ecophlon” PTFE patch does not cause rejection of implant.
“Ecophlon” PTFE patch possesses good integration and strong fixation to surround tissues.
“Ecophlon” PTFE patch does not cause inflammatory changes.
Evidence of connective tissue and small capillary ingrowth.
Active migration of fibroblasts in layers of PTFE patch.
“Ecophlon” PTFE patch preserve its own structure in an organism without formation rough contractures and deformations in a zone of implantation.
Conclusion: We would like to emphasize that the evaluation was carried out on growing animals. Based on histomorphological evaluation, we consider that Ecophlon PTFE patch could be used for diaphragmatic repair in neonates.
A Novel and Precise Evaluation Model for Psychomotor Skills in Pediatric Endoscopic Surgery
Purpose: Psychomotor skill is absolutely necessary for endoscopic surgeons. Pediatric surgeons are required for advanced psychomotor skill in manipulating the forceps because of the small working space. We devised tasks and parameters to evaluate psychomotor skills during endoscopic surgery and investigated their validity.
Methods: Sixteen novice medical students (N) and 10 expert surgeons (E) who had performed over 50 endoscopic surgeries participated in the study. We evaluated psychomotor skill by asking the participants to move forceps in a straight-line space as shown in figure 1 mimicking the small working space of pediatric endoscopic surgery. Three-dimensional position measurements of the forceps tips were analyzed with an electromagnetic tracking system (AURORA; Northern Digital Inc. CANADA) as shown figure 2. The following parameters were evaluated: efficiency of spatial distance, summation of spatial deviation, integration of deviation, motatsuki time, and motatsuki distance. Motatsuki means hesitation in achieving the desired goal point. The definition of the summation of deviation and integration of deviation were shown in figure 3. Data are expressed as mean ± SD. A two-way repeated measure ANOVA and the Bonferroni method for multiple comparisons were used to identify differences at a significance level of p < 0.05.
Results: There was no difference in the efficiency of spatial distance with the dominant (right) hand (N, 1.8 ± 0.8; E, 1.2 ± 0.1) but there was a significant difference (p < 0.001) with the non-dominant (left) hand (N, 1.7 ± 0.2; E, 1.2 ± 0.1). The summation spatial distance (mm) between the dominant (N, 716.1 ± 425.2; E, 130.9 ± 137.0) and the non-dominant hands (N, 579.1 ± 176.8; E, 119.7 ± 87.4) was significantly different (p < 0.05). Moreover, the integration of spatial distance (mm2) was significantly different (p < 0.01) between the dominant (N, 929.9 ± 374.8; E, 319.9 ± 137.0) and non-dominant hands (N, 790.2 ± 141.7; E, 258.4 ± 102.0). The motatsuki time (s) of the dominant (N, 1.1 ± 0.4; E, 0.5 ± 0.2, p < 0.05) and non-dominant (N, 1.0 ± 0.2; E, 0.6 ± 0.3, p < 0.01) hands was significantly different. The motatsuki distance (mm) of the dominant hand (N, 25.6 ± 4.4; E, 19.7 ± 3.7) was significantly different (p < 0.05) but there was no difference with the non-dominant hand (N, 22.4 ± 4.0; E, 18.4 ± 2.1).
Conclusions: Our evaluation task model discriminated the level of psychomotor skill required for safe and precise pediatric endoscopic surgery. We suggest that the dexterity required for endoscopy can be evaluated using this simple and sensitive testing procedure.
Colorectal
Laparoscopic Repair of Anorectal Malformations: The Red Cross Children's Hospital Experience
Objective: Patients with anorectal malformations are repaired using a Posterior Saggital Anorectoplasty (PSARP). Recently, a minimally invasive technique, laparoscopic-assisted anorectoplasty (LAARP), has been performed at Red Cross Children's Hospital. This study was designed to assess the outcome of this procedure and address a perceived concern regarding increased complication rates.
Methods:
Operative technique: Laparoscopic mobilisation of the rectum was performed with hook diathermy. Fistulae were divided with scissors and in most cases fistulae stumps were not closed. A STEP port was introduced through the centre of the external sphincter and the rectum pulled through. Standard anoplasty was then performed. A detailed case note review of all patients undergoing LAARP was conducted, identifying patients from the database of surgical procedures held by the Department of Paediatric Surgery and the colorectal database of the Anorectal Clinic. Patients attending routine clinic appointments were interviewed using the Krickenbeck standardised questionnaire to assess bowel function.
Results: Between September 2005 and June 2009, 24 patients underwent LAARP. No patients were known to be HIV positive. Sixteen patients had associated anomalies. Median age at surgery was 7.5 months (2.6–15.0). Subtypes of anorectal malformation were as follows: Vestibular, 2; Bulbar, 9; Prostatic, 7; Vesical, 3; and 3, no fistula. One patient was converted to PSARP. There was a 16% early complication rate. Dilatation difficulties occurred in 62.5%. Redo anoplasty for anorectal stenosis was required in 33%. Twenty-three patients have had their stoma closed. Eleven patients had difficulties with follow-up; 5 lived away from Cape Town and 6 were poor attenders.
Thirteen patients had regular follow-up and were analysed further. Toilet training had been completed or was nearly complete in 7 patients. Five patients had a good or satisfactory outcome, despite two requiring a redo anoplasty for stenosis due to non-compliance with dilatations. A poor outcome due to incontinence or regular soiling was noted in 2 patients.
Six patients are awaiting toilet training or are unable to train due to incontinence. Four are complex cases due to non-compliance with dilatations, poor nutrition or poor sensation. All four have required at least 1 redo anoplasty or dilatation under anaesthetic.
Conclusions: Outcome has been difficult to assess in the majority of cases. Despite using a minimally invasive technique, anal stenosis post surgery has been a particular problem. The causes appear to be multifactorial but poor compliance with dilatations is a leading factor.
Education and close supervision of post-operative dilatations is essential prior to closure of colostomy. Regular long-term follow-up and support is also required.
Primary Neonatal Laparoscopic-Assisted Anorectal Pull-Through (LAARP) for High Anorectal Malformation
Only a handful of primary neonatal laparoscopic-assisted anorectal pull-through (LAARP) procedures for high anorectal malformations have been reported, due to concerns about peritoneal soiling with meconium from the distended, obstructed rectum, and inadequate visualization of the anatomy. While limited in number, comparative series of laparoscopic-assisted and traditional posterior-sagittal anorectoplasty have, however, shown equivocal success rates. Good results with neonatal primary open procedures (using a Pfannenstiel incision mini-laparotomy or posterior-sagittal approach) have been reported. We report a primary LAARP done in a neonate with long-gap oesophageal atresia without a distal tracheo-oesophageal fistula, and an imperforate anus with recto-bulbourethral fistula, representing an ideal case for LAARP approach due to the undistended nature of the bowel and sterile meconium. During the same-procedure a gastrostomy was facilitated by laparoscopy. Our modifications to Georgeson's original technique are easily applied in resource-constrained situations. Further evaluation of the applicability of LAARP in the management of infants with anorectal malformations is needed, including assessment of the long-term outcome.
Cool Tricks
Cystoscopy-Assisted Percutaneous Removal of Impacted Urethral Stone: A Case Report
Background and Purpose: Although cystolitholapaxy is possible in children, the instruments are not available everywhere. For tiny impacted urethral stone, an alternate technique is described.
Case Report: A 3-year-old boy came with retention of urine and dysuria. On examination bladder was full, supra-pubic region was tender, and a stone could be felt at posterior urethra. We planned push back and supra-pubic cystolithotomy. After general anesthesia the stone was pushed back by instillation of lignocaine jelly into urethra. Then, a cystoscope was introduced and stone was found inside urinary badder. Under cystoscopic view a 5 mm laparoscopic port was inserted into bladder just above the pubic symphysis in the midline. A 5 mm tissue holding forceps was introduced through this port and the tiny stone was grasped and brought out along with the port. The port site was closed by a single stitch. Penile catheter was kept for 5 days.
Results: The boy did well in the post-operative period and voiding was normal after removal of catheter.
Conclusions: Impacted posterior urethral stone can be retrieved by simple percutaneous technique.
Laparoscopic Inguinal Preperitoneal Injection (LIPI): Novel Technique for Inguinal Hernia Repair—Preliminary Results of Experimental Study
Background: Inguinal hernia repair is the most common procedures in pediatric surgery. Suture techniques for laparoscopic inguinal hernia repair in children are easy to perform and popular with a low recurrence rate and morbidity. The aim of this study was to evaluate the effect of laparoscopic preperitoneal injection of 3-dimesional gel on closing of the inguinal hernias in laboratory animals.
Materials and Methods: Under general anesthesia, we performed peritoneoscopy by 12 male Chinchilla rabbits weighing 1200 to 1400 g. Endoscope was introduced in abdominal cavity and bilateral deep inguinal rings were identified. The needle Tuohy with the injectable polimeric bulking agent DAM+ (3-Dimensional Polyacrylamide gel with Ions of Silver “Argiform,” Bioform®) was introduced preperitoneally. The implant was then injected across the entire orifice of the deep inguinal rings and draped over the cord structures. After completion of bilateral repairs, the rabbits were extubated and observed in animal laboratory. Then the second laparoscopy was performed 6 months after and the deep inguinal rings were inspected.
Results: The postoperative course was uneventful in the all animals. There were no operative or postoperative complications. At second laparoscopy no reopening to the entire orifice of the deep inguinal rings were noted. Accurate placement the polymeric agent and adequate coverage of the vas deferens was accomplished in all animals.
Conclusion: This study demonstrates that the biopolimeric implant gives good postoperative results and a stabile trend of closing inguinal hernias in long-term follow-up. In conclusion, we hope that the injectable polimeric bulking agents can be used for treatment of inguinal hernias at pediatric patients after additional animal and human researches.
Immediate Laparoscopic Repair of Large Traumatic Abdominal Wall Hernia in a 2-Year-Old Child
Introduction: Traumatic abdominal wall hernia is a rare type of hernia caused by blunt trauma that does not penetrate the skin but has enough force to disrupt the underlying fascia and allow for subcutaneous herniation of bowel contents. We describe the first laparoscopic repair of a traumatic abdominal wall hernia in an acute setting in a 2-year-old child.
Case Report: Our patient was a 2-year-old boy with no medical history who presented hemodynamically stable with a GCS of 12 after having been accidentally hit by his grandmother's car. There was palpable bowel just underneath the skin on the left side of his abdomen. CT imaging confirmed a traumatic left anterior abdominal wall hernia that appeared to contain both small bowel and transverse colon. The patient was taken for immediate exploratory laparoscopy and herniorraphy. During surgery, a big 7–10 cm defect in the abdominal wall was found extending from near the midline to the left flank. After the procedure, the patient did well and was discharged on post-operative day 5. At 1 and 3 months of follow-up there were no scars, pain, or recurrence.
Operative Technique: Two 5 mm one-step expandable ports were placed in the patient's abdomen and exploratory laparoscopy was performed. A 5 mm 30 deg telescope was introduced once pneumoperitoneum was achieved. On inspection, there was a large traumatic left-sided abdominal wall defect with a hernia. The omentum and small and large bowel were seen to have herniated through the defect. No other injuries were seen. After exploratory laparoscopy was completed for abdominal trauma, repair of the defect was started. A GraNee needle (R-Med, Inc., Oregon, OH) was used to place several sutures through the abdominal wall defect. This was helped by a laparoscopic needle holder from inside. Only two 5 mm ports were used for the entire repair. Using the GraNee needle technique, the two ends of the defect were brought together with the sutures tied subcutaneously leaving no scars. Approximately 10–12 (2-0 Vicryl) interrupted sutures were placed in total, which took about an hour. Excellent results were obtained.
Conclusion: We report the first case of a successful laparoscopic repair of a traumatic abdominal wall hernia in a child. Additionally, this repair was done in an acute setting (in conjunction with an exploratory laparoscopy), which has not been previously described in a child. We were compelled to perform an exploratory surgery due to suspicion of bowel injury and decided that it would be best to perform the herniorrhaphy at the same time. This approach allowed us to perform a one-step operation on the night of admission, at which point all significant internal injury was ruled out and the hernia repaired using our new technique. The laparoscopic approach also conferred significant benefit to the patient by decreasing pain, hospital stay and delivering cosmetic benefit. We recommend this technique for any patient with traumatic abdominal wall hernia.
Laparoscopic Splenectomy: Comparison Between Anterior and Posterior Approaches
Aim: Splenectomy, except for an emergency purpose, is now performed through a laparoscopic approach. There are mainly two ways for laparoscopic total or partial splenectomies. For the classic anterior dissection of the splenic vessels, patient is placed in dorsal position and 4 to 5 trocars are required to elevate the spleen and proceed to vessel divisions. With a posterior approach of the pedicle, patient is placed in lateral position and 3 trocars are sufficients, because gravity helps to provide traction on the various ligaments and to present hilar vessels and pancreas tail. The aim of our study was to compare surgical complications of those two approaches of laparoscopic splenectomy.
Methods: We reviewed 84 medical records of patient operated on for hematologic disease between January 1993 and December 2009.
Results: There were 47 anterior and 37 posterior approaches. Sex, disease, median age, median operative time, median blood lost, median hospital stay, and associated laparotomy were not different between the two groups. Pre- and post-operative complications included haemorrhage (5), bowel injury (1), diaphragmatic wound (1), pancreas tail section (1), and parietal haematoma (1) in the anterior group (9 cases) versus 1 hemorrhages in the posterior group (p < 0.02 Qi2 test). There were 4 laparotomies owing to surgical complications in the anterior group, none in the posterior group.
Conclusion: Splenectomy through laparoscopic approach is an effective technique. Posterior dissection of the vessels provides less operative complications in children.
Laparoscopically Assisted Repair of Congenital Intestinal Atresia
Purpose: Laparoscopic-assisted surgery to repair jejuno-ileal atresia in newborns combines minimally invasive identification and isolation of the atresia with open repair of the defect.
Surgical Technique: Three newborns with jejuno-ileal atresia, two of whom were diagnosed prenatally, underwent laparoscopic-assisted repair of their congenital abnormality. One was type II (two ends connected by a fibrous scar without mesenteric defect) and two were type IV (multiple and separate atretic segments with mesenteric defects). An Endoloop was used to deliver the distal segment of the atretic bowel in type IV atresia through the umbilical port incision.
A peri-umbilical incision was made and a 5 mm cannula was inserted via an open technique. Carbon dioxide pneumoperitoneum (5–8 mmHg) was achieved, and two 3 mm cannulas were inserted in the inguinal creases. The site of pathology was easily determined by the transition point between dilated and decompressed bowel. Distal bowel was examined for evidence of additional atresia. Exteriorization of the atretic segment(s) was performed through the umbilical incision. In the type II atresia case, the proximal and distal ends were in continuity. In the type IV atresias, the distal end was ensnared with an Endoloop (Ethicon Endo-Surgery, Johnson and Johnson, Cincinnati, OH). The proximal loop was grasped with an endoscopic bowel grasper. Instrument and Endoloop were simultaneously removed with the umbilical port, exteriorizing proximal and distal bowel segments through the umbilical incision. In one patient, multiple atresias were found. Patency of the intestinal tract was confirmed by instilling saline through the distal segment and into the colon. Anastomoses (single or multiple) were performed in a standard fashion outside the abdomen, after which the intestines were returned into the peritoneal cavity.
Results: No perioperative complications were encountered and all three patients had uncomplicated courses.
Conclusion: Laparoscopic-assisted surgery for intestinal atresia in the newborn combines a virtually scarless approach with the ease of an open repair. The use of Endoloops facilitates identification of the atretic segments and atraumatic exteriorization for repair.
A Right-Sided Congenital Diaphragmatic Hernia Repaired Microthorascopically
Purpose: A case of right-sided (CDH) repair in a newborn using a microthoracoscopic approach is reported. The case is discussed with specific emphasis on the so-called “liver-up” phenomena.
Methods: A right-sided CDH with the liver up and intestinal prolaps was treated using 2 mm instruments exclusively including a newly developed 2.4 mm miniscope. The patient was a newborn female, 39 + 2 GW, birth weight 3170 g. A diaphragmatic hernia with a thin peritoneal sack covering the prolapsed organs was found. Closure of the diaphragmatic defect was achieved with non-absorbable interrupted sutures in one layer.
Results: The procedure was completed successfully. Intraoperative visualisation was excellent and the reposition of the prolapsed organs including the liver was uncomplicated. Despite the small tip of the 2 mm instruments, it was possible to reduce the liver without puncturing the organ, although required patience. The operating time was 102 min. The intraoperative and postoperative courses were completely uneventful. At follow-up five months post-operative, no scares were visually noticeable at the former miniport sites.
Conclusion: The microthorcoscopic right-sided CDH repair was performed easily. In selected cases the minimal invasive approach to the right-sided CDH with the liver up is feasible. The intrathoracal insufflation certainly helped reducing the liver. The cosmesis is superior compared to any open approach or even to the conventional thoracoscopic surgery.
Primary Gastrostomy Button Placement in Children Using a Percutaneous Endoscopic Technique: A Prospective Analysis
Purpose: Percutaneous endoscopic gastrostomy (PEG) tube placement is a popular method of obtaining enteral access in children, but delivery systems that place buttons primarily are used less frequently than traditional delivery systems. The purpose of this study is to describe our experience using the Microvasive One Step ButtonTM for primary placement of low profile gastrostomy buttons in children using a PEG technique.
Methods: Clinical data were collected prospectively on consecutive patients requiring gastrostomy tube placement from February 2009 though September 2010. Preop assessment included an upper GI study to exclude malrotation. All patients received parenteral antibiotics prior to incision. The majority of procedures were performed by a team consisting of a surgical resident (endoscopy) and an attending pediatric surgeon (gastrostomy tube placement). Gastrostomy buttons were placed using the “pull” technique, and control gastroscopy was performed to confirm intraluminal tube position. Laparoscopic guidance was utilized in 3 patients with ventriculoperitoneal shunts in place. Enteral feedings were initiated on the first post-operative day.
Results: Thirty-eight consecutive patients underwent endoscopic placement of low-profile gastrostomy tubes placed using this technique. Mean age was 42 ± 72 months, and 53% (n = 20) were female. Mean weight was 12.5 ± 15.3 kilograms, and 19 patients (50%) weighed less than 5 kilograms. Mean operative time was 22.3 ± 8.8 minutes. None of the procedures were aborted or converted to an alternative approach. Major post-operative complications occurred in 6 patients (15.8%). These were tube dislodgement (n = 4, 10.5%), infected hydrocele (n = 1, 2.6%), and worsening reflux requiring a protective fundoplication (n = 1, 2.6%). All dislodged tubes had pulled back into the tract, and were replaced under anesthesia with Mic-KeyTM buttons using endoscopic or fluoroscopic guidance. There were no cases of visceral injury, esophageal perforation, bleeding, or death. Gastrostomy tubes were first exchanged at least two months following initial placement either in the clinic or with sedation according to parental preference.
Conclusion: This technique is a safe option for primary button placement in pediatric patients including neonates. Advantages include primary button placement, sutureless technique, and an acceptable complication profile.
Operational Report and Technically Observation of the Recently Developed 2.4 mm Mini Scope During its Routine USE
Purpose: To report the technical maintenance, steadiness, illumination, visualisation, fragility and durability of the newly developed mini scope while its routine use.
Methods: We conducted a prospective study to introduce a new mini scope for the purposes of the microlaparoscopy in paediatric surgery. Beginning in 2007 five prototypes and consecutively from February 2009 six serially manufactured and commercially available mini scopes (2.4 mm in diameter, 0°, 18 cm length, Storz, Tuttlingen, Germany) were used routinely. The parameters of illumination, distance view, reflection, parallax error, depth perception, handling of the scope during the procedure, the need for replacement of the mini scope with a 5-mm standard scope, effect of the different light cables on the total optical capacity of the mini scope and the fragility of the mini scope were collected and analyzed. These parameters were measured based on subjective impressions of the surgeons on a scale from 1–5, where 1 was poor, 2 not sufficient, 3 sufficient, 4 good, and 5 excellent.
Results: During the study period, three scopes were mechanically broken during the maintenance. The breakage was located at the connection point between the scope stem and the head. Continues decrease of performance during the first six months of the use resulted in taking off from the operative use in four scopes. The suspected reason therefore was the damage of the lenses due to over bending of the scope during the surgery. Based on subjective impressions of the surgeons, the view of distant objects was rated as sufficient, on average, while the view of nearby structures was, on average, rated as good.
Conclusion: The mechanical instability of the small-diameter scope is a noticeable problem during its routine use. To eliminate this disadvantage of the mini-scope, further technical solutions have to be found, e.g., anti-bending device and additional strengthening of the junction point. However, the overall Illumination benefit of the new mini scope is superior compared to the standard scope for the adult microlaparoscopy.
Laparoscopic Mucosectomy: A Great Option
Aim: To evaluate laparoscopic mucosectomy for variety of pathologies where complete excision will be difficult.
Methods: Laparoscopic mucosectomy was performed in patients with choledochal cyst, oesophagogastric tubular duplication cyst, and intrathoracic oesophageal duplication cysts. In all these patients after the cyst was opened and contents evacuated, a submucosal plane was created by gentle sharp and blunt dissection. In all the patients it was possible to generate a good plane of dissection and mucosectomy was performed easily except in tubular oesophagogastric patients. The mucosa of gastric part of the tubular duplication was difficult to dissect due to inflammation and ulceration, whereas oesophageal part was extrememly easy.
Results: In all 42 patients underwent laparoscopic mucosectomy (37 patients of choledochal cyst, 2 patients with oesophagogastric tubular duplication cyst, and 3 intrathoracic oesophageal duplication cysts). The age group was 2 months to 18 years. There was no significant blood loss and none of the patients required conversion to open surgery. The postoperative recovery was uneventful.
Conclusion: Laparoscopic mucosectomy can be performed safely in difficult situations without causing significant morbidity in children. It is a good alternative for choledochal cyst, tubular gastrointestinal duplications, or oesophageal duplication cyst.
A Safe, Cheap, and Easy Way to Remove the Vermiform Appendix During a Laparoscopic Appendectomy in Children
We describe our technique to remove the vermiform appendix during an acute or complicated appendectomy in children.
Methods: A laparoscopic technique with three 5-mm trocars is used for the appendectomy. To remove the appendix from the abdominal cavity we use the finger of a latex free glove number 7, 7.5, or 8. The finger of the glove (FG) is cut at its base and a partial horizontal incision is made at the distal quarter. A 5-mm Johann grasper is passed inside the FG and both introduced into the abdominal wall through one of the trocar's incisions (generally at the lower right quadrant). The FG remains at the abdominal wall, verifying that both extremities of the FG are out of the abdominal wall. One Kelly clamp is applied at the external part of the FG to avoid its intra-abdominal displacement. With the Johann grasper the base of the appendix is grasped and the appendix is removed in an axial way. The intra-abdominal part of the FG needs to be stabilized with another grasper during the removal procedure. Once the appendix is out of the abdominal cavity the FG is removed from the abdominal wall verifying its complete integrity.
Results: we have removed almost 220 appendices using this technique without complications. We have had only 1 immunosuppressed patient that developed an infection of the trocar sites. The time that takes to remove the appendix with this technique is 2 to 4 minutes.
Conclusion: Our technique is easy, safe, feasible, cheap, and very useful to avoid the contamination of the abdominal wall while extracting the vermiform appendix during a laparoscopic appendectomy in children.
Laparoscopic-Assisted Placement of Ventriculoperitoneal Shunts in Children
Purpose: To describe a simple technique for laparoscopic-assisted placement of ventriculoperitoneal (VP) shunts for hydrocephalus and review our case series of pediatric patients undergoing this procedure for both primary shunt placement and shunt revision.
Methods: All patients undergoing shunt placement in the last 3 years were reviewed. These procedures are performed in collaboration with neurosurgeons and pediatric surgeons. For the abdominal portion, a 4-mm port is placed via the umbilicus and the abdomen is insufflated and inspected. In patients with significant adhesions from previous shunts or surgery, a 3-mm grasper is introduced through a stab incision to divide these adhesions and assist in placement of the catheter. In all other patients, no other instruments are used. A free area of the peritoneal cavity is chosen, a stab incision is made in the skin only, and the catheter is tunneled from the cranial incision to this incision. An 11-FR percutaneous introducer kit is used to place the distal (peritoneal) portion of the shunt into the abdominal cavity under direct visualization using a Seldinger technique. The introducer sheath is used to direct the catheter to the desired area of the abdomen.
Results: Initially, laparoscopic-assisted placement of VP shunts was used sporadically in patients suspected of having a hostile abdomen. Due to the ease of the technique, we have instituted its use for all patients with hydrocephalus regardless of previous shunt or surgical history. From 2007 to present we have performed 38 procedures on 33 patients. The patients ranged in age from 4 days to 17 years with a mean age of 4 years 10 months. The average weight was 19.5 kg with a range of 1.3 to 83.9 kg. The mean follow-up is 11.6 months (range 1 to 34 months). There were 8 patients with post-op complications, including infection and shunt malfunction. Of these, 2 (5.3%) patients developed shunt infections requiring externalization and subsequent revision of the shunt. There were 5 (13%) patients with shunt malfunctions three of which were proximal shunt malfunctions and the other two distal malfunctions. All shunts were successfully placed with no conversions. Postoperative LOS is 1–2 days in most cases and all patients have had minimal scars and discomfort. In addition to the usual benefits of laparoscopy including direct visualization, less pain, less adhesion formation, and cosmesis, there have been no wound complications such as leakage from the incision, incisional hernia, or wound infection with the use of the percutaneous introducer. Although, it is difficult to separate the length of the two portions of the procedure, the abdominal portion of this procedure routinely takes less than 15 minutes, and in many cases less than 10 minutes.
Conclusion: Laparoscopic-assisted VP shunt placement is a safe and effective method of shunt placement for hydrocephalus in children. All of the traditional benefits of laparoscopy are realized with complication rates that compare favorably to laparoscopic and open series reported in the literature. It is now our preferred technique in all cases.
Laparoscopic Gastroscopic Transgastric Cystogastrostomy and Cholecystectomy for Pseudopancreatic Cyst After Gall Stone Pancreatitis in Children
Background: Several techniques have been described for the management of pseudopancreatic cyst. They could be open, laparoscopic, or endoscopic. The open technique leads to big scar and has its associated morbidity and the laparoscopic techniques described so far are cumbersome and technically challenging. The endoscopic techniques have poor results as the opening is small and tends to close easily.
We describe our combined technique of laparoscopic, gastroscopic, transgastric cystogastrostomy for pseudopancreatic cyst in children.
Case report: A 15-year-old girl presented to the ER with abdominal pain. She was diagnosed with gall stone pancreatitis. She had high levels of amylase and lipase and CT scan showed necrotizing pancreatitis. She was managed conservatively. She subsequently developed pseudopancreatic cyst which was diagnosed on the CT scan. She was then taken to the OR for surgical management.
Techniques: Under anesthesia a pediatric pentax gastroscope was introduced in to the stomach. Then, a 5 mm step port was placed in the umbilicus. Three more 5 mm step ports were placed under vision. Two ports on either side of the umbilicus and 1 just under the costal arch to retract the gall bladder. Using these ports the gall bladder was first removed. Then, the stomach was insufllated with air from the gastroscope and 2 pexy sutures with 3’0’ vicryl were placed to pexy it to the abdominal wall using Granee needle. A 12 mm port was then directly introduced into the stomach under vision of the gastroscope. One of the other ports used for gallbladder removal was the also introduced into the stomach under vision. The 5 mm 30 deg telescope was then introduced into the stomach and the stomach was continuously insufflated with low flow. The pseudocyst was easily identified on the posterior wall. A laparoscopic needle was then introduced through the port into the cyst to confirm the position of the cyst. A harmonic scalpel was the introduced in to the stomach and an opening was made into the posterior wall of the stomach in to cyst. Once this was achieved a 30 mm endoGIA stapler was then introduced through the 12 mm port and a stapled cystogastrostomy was achieved. The cyst contents were suctioned and the cyst was irrigated with saline. Gastric port sites were closed with 3’0’ vicryl interrupted sutures.
Patient tolerated procedure well and was started feeds on 4th post operative day. She was discharged home on the 6th post operative day.
She was followed up in clinic at 4 weeks and 3 months post-op. She had well healed scars and was feeding fine with no other problems.
Conclusion: Laparoscopic Gastroscopic Transgastric Cystogastrostomy is a safe technique for pseudopancreatic cyst in children. We recommend the use of this technique in suitable cases.
Tricks and Hints to Facilitate Videosurgery Using Stitches, Stylets, Tubes, Special Knots and Patient Positioning
Background: Laparoscopic and thoracoscopic procedures generally require visceral traction or retraction, in order to allow good exposure of the target organs and to perform all the important procedures. Most surgeons usually introduce an instrument through an additional orifice or trocar, to be handled by a second or even a third assistant, who is usually a less experienced surgeon or nurse. Each trocar forms a scar and carries its risk for complications. The aim of the authors is to present many tricks and hints to facilitate videosurgery using transparietal sutures, special knots, stylets, luminal tubes, and patient positioning to avoid the use on unnecessary or dangerous extra instruments and ports, making videosurgery really minimally invasive.
Patients and Methods: In over 2300 patients, many techniques for application of transparietal staying sutures to retract or pull the liver, stomach, bowel, bladder, rectum, gallbladder, ovaries, lungs, ureters, etc., could be helpful in almost all laparoscopic and thoracoscopic procedures, to allow the use of one, two or three ports in most operations. Sliding knots could be used to anchor some organs and close the lumen of some viscera. Changing the position of the patient took advantage of gravity to make bowel, omentum, lung, stomach, etc., to fall down and go off the operating field. Fine stylets could be used to substitute larger instruments for retraction, introduced through 1–2 mm stab wounds. Endorectal or gastric tubes could mobilize the organ onto different directions to facilitate some procedures.
Results: All the described techniques proved to be very useful and reduced the number of ports or orifices to a maximum of 2 or 3 ports in most operations, leading to the expected advantages of using less trocars. Staying sutures and stylets had the function similar to fingers, hands, and retractors in open surgery. Keeping the retracted viscera steady and away, and avoiding the participation of a second or third assistant, inadverted lesions of organs did not occur, the working space inside and outside the patient were much favored. Many cases that could otherwise be converted to open surgery had more chance to be accomplished laparoscopically due to better exposure. Each type of operation required specific tricks resulting in elegant and fast operations.
Conclusions: The surgeon should apply the different technical maneuvers to facilitate laparoscopic or thoracoscopic procedures in order to keep the viscera in steady positions, to use the minimum of trocars or extra hands and to make the operations safer, cheaper, faster, and easier.
Gastrointestinal & Hepatobiliary
Laparoscopic Splenectomy Without Stapler
Hypersplenism nowadays is treated laparoscopically. The hilar vessels are usually sealed by stapler.
Since year 2008, 20 patients have undergone laparoscopic splenectomy in Shiraz University of Medical Sciences. The age range was 7–17 years with a mean of 13. Seventeen patients had Major Thalassemia and three had spherocytosis. The mean operation time was about 80 minutes. The mean size of the spleen was 16 × 5 × 7 cm. The splenic vessels were only sealed with Ligasure and no stapler werre used. Two patients were converted to open laparatomy due to bleeding and for three patients small transverse incisions were used to deliver the spleen out. Spleen extraction was by endobag in 15 patients. Post operation there were no complications and they only received daily penicillin V orally. The mean hospital stay was about 3 days.
The patients were followed for 6–24 months and there were decreaed need of transfusion and no late complication.
In conclusion, laparascopic splenectomy using Ligasure is a safe procedure in patients with hypersplenism and splenomegally.
Laparoscopic Resection of a Giant Solid Pseudopapillary Neoplasm of Uncinate Process of the Pancreas in a Child
Introduction: Solid-pseudopapillary neoplasm (SPN) of the pancreas is a relatively uncommon tumor, especially in children. To our knowledge, 9 cases of laparoscopic resection for solid pseudopapillary neoplasm of pancreas, which included only 2 cases in pediatrics, were published in the English literature and laparoscopic resection of uncinate process of the pancreas has never been reported.
Case Report: A 10-year-old girl suffered from recurrent abdominal fullness. The abdominal CT revealed a homogenous, cystic content, tumor, 5.6 × 5 × 6 cm, over pancreatic head. According to preoperative MRCP, there was a safe margin between neoplasm and main pancreatic duct. It was decided that a surgical intervention for the lesion, and a laparoscopic approach was elected. The patient was placed in supine modified lithotomy position with the surgeon standing between her legs. Four working ports, 5 mm, were used. The Kocher maneuver was performed with the aid of a Harmonic Scalpel (Ethicon Endo-Surgery, Cincinnati, OH) to expose pancreatic head and uncinate process. The inferior vena cava, transverse colon, duodenum, and pancreas were clearly identified.
Results: Operative time was 480 minutes and blood loss estimated in 500 ml with no blood transfusion. Postoperative hospital stay was 4 days. The patient did not have postoperative pancreatitis or pancreatic leakage. Final pathology confirmed the diagnosis of solid pseudopapillary neoplasm of pancreas. The patient was discharged following an uneventful postoperative course.
Conclusion: As experience with minimally invasive techniques continues to grow, laparoscopic pancreatic resections appear to be safe and feasible in children with SPN and should be considered for patients suffering from pancreatic neoplasms.
Laparoscopic Hiatus Hernia Repair in Children
Objective: To assess the outcome of laparoscopic hiatus hernia repair in children.
Methods: This was an observational study of prospectively collected data on 312 children undergoing anti-reflux surgery between July 1998 and March 2010. Follow-up ranged from 1 month to 127 months (median 15 months). 30 of the children had laparoscopic hiatus hernia repair performed concomitantly with laparoscopic fundoplication. Absolute failure rate was defined as recurrence of symptoms necessitating re-do surgery. Statistical analysis was performed using Stata version 7.
Results: 30 of the 312 children had a hiatus hernia at the time of fundoplication. The characteristics of these 30 children were as follows: median age at operation 2.7 yrs (range 0.4–16.32 yrs) and median weight 14.5 kg (range 5–35.9 kg). 19/30 were neurologically impaired (63%). All children underwent pre-operative radiological investigation; however, the hiatus hernia was missed in 26%. 28 patients underwent suture repair of the defect and 2 patients required a patch repair. Overall failure rate of anti-reflux surgery for the 312 children was 9.9%. Symptomatic hiatus hernia recurrence occurred in 6 of the 30 (20%) children who had undergone hiatus hernia repair. At redo surgery, all had recurrence of the hiatus hernia and one also had a wrap dehiscence. Failures occurred with both the suture (n = 5) and patch repair (n = 1).
Significant difference Chi-squared test p = 0.05.
A multivariate logistic regression analysis of all anti-reflux surgery was performed using age, weight, neurological impairment, type of fundoplication (Nissen or Thal), oesophageal atresia, presence of hiatus hernia, seniority of the operating surgeon, and length of follow-up as possible risk factors for failure. Presence of a hiatus hernia significantly increased the risk of failure (odds ratio 5.37, 95% confidence interval 1.71–16.8, p = 0.004). There was an increased risk of failure associated with Thal versus Nissen fundoplication (odds ratio 3.2, 95% confidence interval 1.34–7.65, p = 0.009) and presence of neurological impairment (odds ratio 4.69, 95% confidence interval 1.16–18.9, p = 0.03). No increased risk of failure was associated with the other factors.
Conclusions: Hiatus hernia repair in children is associated with a 20% risk of operative failure requiring redo surgery. The risk of failure is significantly higher than following fundoplication alone. Failure occurred following both suture and patch repairs. The best definitive repair of hiatus hernia is still unclear. Hiatus hernias were noted more frequently during surgery than predicted by preoperative upper gastrointestinal contrast study.
Background: Supported by the evidence presented by Aziz and co-workers and by the Cochrane collaboration in 2006, we decided to switch from open to laparoscopic appendectomy in October 2007. The purpose of this study was to evaluate the safety and feasibility of a swift transition from an open to a laparoscopic approach for acute appendicitis in children.
Materials and Methods: A total of 655 patients underwent appendectomy during 2007–2008, 349 with laparoscopic technique and 306 with open technique. An evidence-based protocol was developed to minimize complications and shorten the learning curve. This protocol provided a standardized laparoscopic surgical technique, including selection and positioning of ports, method of stump ligation, and removal of the appendix from the abdomen. All patients subjected to appendectomy for acute appendicitis were prospectively followed from October 2007. For comparison all patients operated between January and October 2007, predominantly with open technique, were reviewed.
Data are presented as medians. A significant difference is considered when p < 0.05. (ns = non-significant).
Results: 39% of the patients were girls and the median age was 11.3 years. 3.4% of the patients in the laparoscopic group were converted to open technique. The frequency of negative appendectomies was 2.1%. The operating time was shorter in the open group, 37 versus 51 minutes (p < 0.0001). After 25 procedures the operating time for laparoscopic surgeons was comparable to the open technique, 37 versus 43 minutes (ns), decreasing further to 39 minutes after 50 laparoscopic appendectomies and to 28 minutes after 70 laparoscopic appendectomies. The postoperative hospital stay was shorter in the laparoscopic group than in the open group, 2.0 versus 2.8 days (p = 0.023) but similar in 2008, 2.0 versus 1.9 days (ns). There was no difference in the frequency of intra-abdominal abscess formation: 4% in the laparoscopic group and 5% in the open group respectively (ns).
Conclusions: Our data support the safety and feasibility of a swift transition from open to laparoscopic appendectomy in a high-volume university hospital with a diversity of laparoscopic skills. We used a strict protocol and thorough training to support a short learning curve. The learning curve should be considered to consist of about 25 laparoscopic procedures to attain operating times comparable to open surgery. As a secondary outcome, our transition from open to laparoscopic surgery for acute appendicitis has benefitted us in performing other more advanced minimally access procedures.
Double Hand Ligasure® Technique May Facilitate Laparoscopic Splenectomy
Aim: Laparoscopic splenectomy may be challenging especially in patients with large spleens. Tissue sealing device (Ligasure®) is a useful instrument for the dissection of the spleen and its attachments. It is widely used by most surgeons. We hypothesized that Ligasure® in both hands might be even more advantageous and it may ease the dissection of the spleen.
Patients and Methods: Three patients with hereditary spherocytosis (all males, 3, 13, and 16 years old) underwent laparoscopic splenectomy. Laparoscopy was performed with standard four trochar technique. We applied two Ligasure® in right and left hands. We evaluated technical advantages of Ligasure® in both hands in the laparoscopic splenectomy.
Results: We found that Ligasures® in both hands provides cutting and sealing with both hands and this maneuver facilitates the dissection of the spleen. In all three cases the splenectomy has been performed more easily. The shotest time of surgery was 35 minutes. No complication has been experienced. In one patient, a cholecystectomy has also been carried out.
Conclusion: Tissue sealing devices (Ligasure®) are very useful instrument in laparoscopic splenectomy. Two Ligasures® in both hands eases the dissection of the spleen.
Laparoscope-Assisted Diagnosis and Treatment for Small Intestinal Atresia and Stenosis in Children-A Report of 12 Cases
Objective: To retrospectively analyze the laparoscope-assisted diagnosis and treatment for small intestinal atresia and stenosis in children.
Methods: From September 2009 to February 2010, 12 infants with small intestinal atresia and stenosis underwent laparoscope-assisted surgery at this center. Among the patients, 1 was diagnosedas jejunum stenosis, 2 as type duodenum atresia, 3 as type atresia (25%), 6 were type Atresia (50%). No evident dilated abdomen was noted on the patients with jejunum stenosis or type duodenum atresia, and the laparoscopic operation were performed to remove the septum and restore the intestinal continuity. On the patients with type and type atresia, the bowel dilated evdently, laparoscopic inspection was performed to identify the location and the type of the malformations, and then the proximal and distal ends of the atresia were exteriorized through the umbilical port site for end-to-oblique anastomosis.
Results: The operative time for jejunum stenosis, type duodenum atresiaranged from 80–100 minutes, (average, 92 minutes). The operative time for type and type atresia ranged from 40–65 minutes (average 48 minutes). The incision of umbilical port is about 1.5–2 cm long. One premature infant was abandoned by the parents, all the other cases recovered from surgery. Feeding was started between postoperative day 3 and 7. No dilated abdomen and vomit was noted. The patients were discharged from hospital between postoperative day 9 to 16, with no mortality rate in the group. Eleven cases were followed-up for 1–6 months; no severe complication was noted.
Conclusion: Laparoscopy-assisted surgery is minimally invasive and rendered good outcomes in diagnosis and treatment for congenital intestinal obstruction.
Exploration in Indicator of Turning Laparotomy and Prevention of Complication in Laparoscopic Cyst-Excision with Roux-Y Hepatoenterostomy for Choledochal Cyst
Background: To explore the indicator of turning laparotomy and prevention of complication in laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy for the treatment of choledochal cyst in children.
Methods: Under the guidance of laparoscope, cholecystography was operated to understand the expansion condition of choledochus, and abnormality of intrahepatic duct and pancreatic duct. Laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy were carried out.
Results: Fourty-eight cases of choledochal cyst were examined with B-ultrasound and CT before operation. Fourty-six cases were carried out with laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy. Two cases turned to laparotomy becaused of severe inflammation of cyst wall and much bleeding. Anastomotic leakage appeared in one case after operation, because the drain stabed anastomotic stoma with the child's dysphoria and much unsteady. The case was carried out with laparotomy and anastomosis. Pancreatic leakage appeared in one case after operation, disappeared after being drained 1 month. The operation times were 2.5–6.5 hours. The patients were aged from 4 months to 14 years. Conclusions: Laparoscopic excision of choledochal cyst and Roux-Y hepatoenterostomy for the treatment of choledochal cyst was effective and safe procedure in children. But the laparotomy must be carried out in heavy inflammation of cyst wall, longer time of operation and the deformation of intrahepatic duct and pancreatic duct. The key is the skilled technique, the cautious procedure and the careful nurse.
Resection of a Duodenal Web Using Single-Incision Pediatric Endosurgery
Background: A single-incision pediatric endosurgery (SIPES) approach is used in many centers for routine cases such as appendectomies, cholecystectomies, or splenectomies. More complex procedures are still infrequently performed. We report our first SIPES duodenal web resection with tapering of the dilated proximal doudenum.
Materials and Methods: A 9-month-old girl with Down syndrome was admitted to our hospital with chronic nonbilious vomiting, a massively dilated stomach, double-bubble on abdominal X-ray, and gastric pneumatosis. An upper gastrointestinal endoscopy showed duodenal web with a pin-point hole in the center. After antibiotic treatment, gastric decompression, and resolution of the pneumatosis, she was taken to the operating room for laparoscopic duodenal web resection.
Results: The operation was performed through a 2 cm incision in the umbilicus using a proprietary single-incision trocar. The duodenum was mobilized, fixed to the anterior abdominal wall using a suture, and a longitudinal duodenotomy was performed at the transition zone from dilated to collapsed duodenum. Identifying the papilla, the duodenal web was incised using electrocautery hook and the duodenotomy was closed transversely using a polyglecaprone suture. The dilated proximal duodenum was tapered to normal caliber using an articulating endoGIA stapler. The procedure took 209 minutes. Postoperatively, the patient was feeding well, gaining weight, and had no appreciable scar at a follow-up of 6 months. An upper gastrointestinal contrast study at that time was normal. No complications were noted.
Conclusion: Resection of a duodenal web in an infant using the SIPES approach is a reasonable alternative to conventional triangulated laparoscopy that can be performed safely with good functional and cosmetic postoperative results.
Laparoscopic Pancreaticojejunostomy for Pancreatic Ductal Dilatation in Children
Background: Laparoscopic surgery is widely development in pediatric surgery. However, the number of reports on pancreatic surgery is still very small in children. In this article, we describe laparoscopic pancreaticojejunostomy for children with congenital pancreatic ductal dilatation.
Methods: Three children with recurrent pancreatitis and pancreatic ductal dilatation underwent laparoscopic pancreaticojejunostomy between November 2005 and February 2010. Following longitudinal splitting the dilated pancreatic ducts, a side-to-side Roux-Y pancreaticojejunostomy was performed.
Results: The time required for surgery was 103 to 154 min, and blood loss was minimal without necessity for blood transfusion. The average hospital stay period after the operation was 4 to 6 days. As postoperative complication, pancreatic juice leak not occurred in these cases. All the patients had been followed up and no pancreatitis recurrence.
Conclusions: Laparoscopic pancreaticojejunostomy for children with congenital pancreatic ductal dilatation is safe and effective.
A Simple, Safe, and Quick Technique for Laparoscopic Gastrostomy Placement at the Time of Laparoscopic Fundoplication
A simple, safe, and quick technique for laparoscopic gastrostomy placement at the time of laparoscopic fundoplication.
Gastrostomy placement is a common procedure in pediatric patients with dysphagia or failure to thrive. Options for gastrostomy tube insertion at the time of laparoscopic antireflux procedure include laparoscopic gastrostomy, percutaneous endoscopic gastrostomy (PEG), and open gastrostomy.
We describe a simple, safe, and quick technique for gastrostomy tube placement in infants using the existing ports from laparoscopic fundoplication (four-port-technique). After a small gastric perforation was placed at the proposed gastrostomy site using a hook electrocautery, a gastrotube was inserted percutanously at the site of the left epigastric port after removing the port. Under laparoscopic supervision and elevating the stomach against the gastrotube, the tube was inserted into the stomach. The gastrotube balloon was inflated and the stomach was elevated to the ventral abdominal wall through traction on the gastrotube. The gastrotube was fixated under mild traction with the external plate. No additional sutures or exteriorization of the stomach were needed. Between 2007 and 2010 we used this technique in 9 patients undergoing laparoscopic gastrostomy placement at the time of laparoscopic fundoplication. The diagnoses underlying the necessity of gastrostomy placement were mitochondrial encephalopathia (2), epileptic encephalopathia (4), hypoxic encephalopathia (2), and complex cerebral malformation (1). The patient age ranged from 7 months to 11 years. The follow-up time ranged from 3 to 36 months.
Intraoperatively no additional port had to be placed, but in 1 patient the gastrostomy site differed from the left epigastric port site due to a small stomach. No major PEG-related complications were recorded. In 4 patients, minor PEG tube problems arose in the postoperative period. All were easily treated on an out-patient basis. The described technique provides a simple, safe and effective approach for gastrostomy placement. It does not require a combined laparoscopic and endoskopic approach, nor additional suture fixation or exteriorization of the stomach.
Laparoscopic-Assisted Choledochoscopyfor Obstructive Jaundice in Infant
The management of common bile duct stones in neonates has not been clearly fully standardized. We report the case of a 5-week-old boy, weight 3800 g, with a severe obstructive jaundice and mild anemia. The preoperative work-up reveled 2 stones (3/4 mm) located in the middle part of the choledochus and a rare form of hemolytic anemia. Under laparoscopic control, a 6 French cystoscope was introduced in the gallbladder and then in the choledocus allowing retrieving one of the two calculus; a drain was left in place allowing to flush the second calculus throught the papilla at day 3 postoperatively. Recovery was uneventful; follow-up was 9 months. This strategy could be an alternarive to endoscopic retrograde stone extraction to manage impacted choledocholithiasis in neonates and infants.
Laparoscopic Nissen Fundoplication: From Five to Three Trocar Approach
Aim: To review a single-institution experience of laparoscopic Nissen fundoplication in the treatment of gastroesophageal reflux disease.
Patients and Methods: A retrospective chart review of 121 children who underwent laparoscopic Nissen fundoplication was performed. Demographic data of the patients, operation times, duration of hospital stay, success rates, presence of intraoperative and postoperative complication, and presence of postoperative reflux were evaluated. Five trocars were used at the beginning; two for liver and stomach retraction, two working ports, and one for camera port. The number of trocars was decreased to three, with one umbilical camera port and two working ports and liver retraction was performed using a “Cook retractor” or a 3–5 mm port.
Results: The mean age of the patients was 63.6 months (53 days–23 years); 14 of the patients were ≤6 months. 38.8% of the patients were female and 61.2% were male. Neurological impairment was associated in 62 of the patients (51.2%). Mean of operative times was 43.2 minutes (25–135). The duration of operation was longer in neurologically impaired patients since concomitant gastrostomy was also performed in the same session in most of these patients. None of them were converted to open procedure. There were no intraoperative complication and mortality. Mean of feeding time was 1.8 days (1–3). Mean length of hospital stay was 4.1 days (1–19). The length of hospital stay of neurologically impaired patints was longer. In 3 of the patients, distal esophageal reflux was found in Trendelenburg position during barium swallow three weeks after the operation. 2 of the patients were reoperated laparoscopically with no complication.
Conclusion: Laparoscopic Nissen fundoplication is a safe and feasible approach in children with gastroesophageal reflux disease. The number of trocars can pare down to three, having even better cosmetic results. Furthermore, by decreasing the number of trocars, there is no need for an extra person for retraction purpose. This must be especially considered in busy surgical centres.
Persistent Hyperinsulinemic Hypoglycemia of Infancy Laparoscopic Pancreatectomy in the Neonatal Period
Laparoscopic near-total pancreatectomy was performed to a 22-day-old neonate with the diagnosis of persistent hyperinsulinemic hypoglycemia who was refractory to pharmacological treatment and no specific lesion could be demonstrated in the imaging techniques. The infant had no problem in the follow-ups for the 6 months. The aim is to emphasize the feasibility of minimal invasive surgery in pancreatic surgery by demonstrating the surgical technique details of this case.
Laparoscopy in the Diagnosis of Lower Gastrointestinal Bleeding with Negative Isotope Scan in Children
Objective: To investigate the application of laparoscopy in the diagnosis of lower gastrointestinal bleeding with negative isotope scan in children.
Methods: 15 children with hemorrhage of lower digestive tract from January 2004 to May 2009 were reviewed in our hospital. 6 patients were accompanied by the abdominal pain, performance of 2 patients was hemorrhagic shock, 5 patients manifest by repeat bleeding in stool more than two times, and 2 patients have blood in stool for the first time. Before the surgery, stomach mucosal scanning was performed in all patients.
Results: 6 patients obtain the dystopia stomach mucous developing, 9 examples for negative result. All patients received laparoscope investigation. And, Meckel's diverticulum was found in ten patients, intestines redundant abnormal in 3 patients, colon parietal vessel lump in 1 child, and allergic purpura in 1 patient. All patients were cured with corresponding treatment.
Conclusions: Although Meckel's diverticulum is the most common cause in hemorrhage of lower digestive tract in children, and positive results were often obtained because of dystopia stomach mucous. In more situations the isotope scanning is the negative result. Laparotomy made the baby guardian difficult to accept, but the laparoscopy was easily acceptted by the patient and the guardian. It has enormous help in discovering the cause of lower gastrointestinal bleeding.
Laparoscopic Cysto-Gastrostomy is a Safe Option for Pancreatic Pseudocyst Treatment
Pancreatic pseudocysts are common sequelae of pancreatic trauma. Although one-third or more of pancreatic pseudocysts might resolve spontaneously, interventional therapy is required for most. The management is based upon the pseudocyst size and presence of symptoms. Those requiring interventions are often drained using several available options. We reported a case on the operative management with minimally invasive technique by laparoscopic transgastric cystogastrostomy.
Case Report: A 7-year-old boy was referred at our institution for an abdominal trauma from a bicycle handlebar with an isolated pancreatic body rupture. The nonoperative management was complicated on day 5 by a portal thrombosis releated by heparin therapy. A large pancreatic pseudocyst developed after the blunt abdominal trauma with oral intake intolerance. Preoperative radiographic CT scan and ultrasound found a single cyst bulging into the posterior wall of the stomach and the median cyst diameter was 90 mm. Surgical treatment was performed with a delay of 34 days.
Laparoscopy cystogastrostomy was realised by a transgastric approach. Only 3 ports were used to complete this operation. Operative time was 110 min. Cystogastrostomy was performed by using an Harmonic Scalpel through the small cystotomy and gastrotomy openings on the posterior wall of the stomach. The anastomosis was completed by interrupted absorbable suture with 3/0 stitchs. Gastrotomy opening on the anterior wall was also closed by suture technique. Mean time to initial and goal feeds was 3 and 6 days, respectively. Patient was readmitted on the 20th postoperative day because of pancreatitis. Endoscopy found no partial closure of the cystogastrostomy and no need for futher operative intervention. The boy remained asymptomatic upon recovery from his pancreatitis and one year follow-up was uneventfull.
Conclusion: A laparoscopic cystgastrostomy, using a trans-gastric surgical technique, offers a safe and less invasive procedure than laparotomy for pancreatic pseudocyst drainage with minimal morbidity and rapid recovery. In our opinion, laparoscopic cystgastrostomy should be considered as an appropriate first-line treatment for pseudocysts in children.
Laparoscopic Anatomical Dextralateral Hemihepatectomy at Tumor of Liver
Of all malignant tumors in children, from 1% to 4% are initial hepatic tumors. Since July 2008, 13 laparoscopic operations were performed in N.N. Blohin Scientific Research Institute of children's hematology and oncology, a subdivision of Russian Academy of Medical Sciences. These operations included different segmental resections and hemihepatectomies. This article is a report of anatomical dextralateral hemihepatectomy (followed by lymphodissection) performed to a 10-year-old girl who was admitted to the hospital in December 2009 with right lobe hepatic tumor, found in the end of September 2009. After further diagnostics a tumor was found to be a hepatoblastoma of the right hepatic lobe. According to ultrasound and tomography data the tumor had unspecified shape and was 6.1 cm by 9.0 cm by 7.0 cm in its size, located in V-VII hepatic segments. Alpha-fetoprotein level was 1245 ME/ml. Two courses of neoadjuvant polychemotherapy were performed. After the course of polychemotherapy no decreasing in the size of the tumor was noted. Alpha-fetoprotein level lowered down to 215 ME/ml. In December 2009 (08.12.2009) the patient underwent laparoscopic dextralateral hemihepatectomy, cholecystectomy, lymphodissection of the hepatoduodenal ligament, and a hepatica communis. Patient positioning during surgery—supine, legs spread. Artificially intra-abdominal CO2 pressure—10 mm Hg. Five operational ports were set: 10 mm—paraumbilical port, 12 mm—right iliac port, 5 mm—right hypochondrium (mid-axillary line), 10 mm—left hypochondrium, 10 mm—umbilical (midclavicular projection). Intra-abdominal revision data: no evidence of tumor dissemination, tumor location—right hepatic lobe, segments SV-VII, size—10.0 cm by 8.0 cm by 8.0 cm. Right triangular, falciform and coronary ligaments were dissected with ultrasound dissector. Bile duct and biliary artery were allocated and blocked with surgical clips. Lymphodissection of the hepatoduodenal zone to celiac trunk. A. hepatica communis was visually examined up to its left and right branches. Right hepatic artery was dissected and blocked with surgical clips (2 clips for proximal end, 1 clip for distal end). Then, visual examination of the portal vein was performed up to its left and right branches. Right branch was blocked with surgical clips and dissected (2 clips for proximal end, one clip for the distal end). Right hepatic vein was allocated near hepatic caval port; parenchymal resection line was visually explored according to the demarcation line.
Cholecystectomy: A 5 mm and 10 mm endoscopic instrument named “LIGA SURE” was used to perform coagulating short hepatic veins and for dissecting liver parenchyma. Right hepatic vein was treated with ENDO GIA 30 endoscopic suture device.
Dextralateral hemihepatectomy: Haemostasis—argon plasma coagulation. Dissected sample was put into a container and evacuated through a 5 cm incision in the right iliac area. Operation duration: 480 min, blood loss—400 ml. Eight days later the patient was discharged from general care unit in satisfactory condition for further home treatment. The following report shows that performing anatomical dextralateral hemihepatectomy (followed by lymphodissection) in children is possible. But, it is still necessary to investigate exact indications for such kinds of operational intervention.
Laparoscopic Management of Pancreatic Pseudocysts in the Pediatric Population: A Report of Two Cases and a Review of Treatment Modalities
Background: In children and adolescents pancreatic pseudocysts have traditionally been drained via open or percutaneous approaches. Over the past decade, minimally invasive techniques for the internal drainage of pancreatic pseudocysts have been applied to the pediatric population. However, because children rarely require surgical intervention for pancreatic pseudocysts, there is a paucity of information in the literature describing the management of this condition using minimally invasive surgical techniques.
Methods: We describe two patients who developed large, symptomatic, and persistent pancreatic pseudocysts following bouts of severe pancreatitis. The first patient is a previously healthy thin 12-year-old male with idiopathic pancreatitis who developed a 12 cm pseudocyst. The patient had symptoms of gastric outlet obstruction associated with significant pain. A computed tomography (CT) scan done 5 weeks following the onset of symptoms demonstrated a persistent pseudocyst with a mature fibrous rind. The second patient is also a 12-year-old male who is obese and who presented with gallstone pancreatitis complicated by a 10 cm pseudocyst. After 5 weeks, a CT scan demonstrated a persistent pseudocyst with a thick rind. Both patients underwent a laparoscopic cystgastrostomy to further manage their persistent pancreatic pseudocysts.
Results: Both operations were completed laparoscopically utilizing a 3-trocar technique. For the second patient who presented with gallstone pancreatitis, a combined cystgastrostomy and cholecystectomy was performed. In each case, a 5 mm trocar was placed through the umbilicus to accommodate a 30 degree, 5 mm laparoscope. Two 12 mm trocars were placed to the right and left of midline in the upper abdomen to allow for an endoscopic stapling device to be introduced at various angles and from different trajectories. The anterior wall of the stomach was opened with the endoscopic bipolar cautery device. In both cases, the exact position of the pseudocyst was confirmed by aspirating cyst contents using a long needle passed transabdominally. Once the exact location of the pseudocyst was confirmed, the posterior wall of the stomach was opened using the monopolar electrocautery, allowing for direct entry into the pseudocyst. Cyst contents were aspirated, and a cystgastrostomy was initiated using the endoscopic stapling device via one of the 12 mm trocars. The cystgastrostomy was completed by extending the anastomosis with the endostapler passed through the opposite 12 mm trocar. Once an adequate anastomosis was completed, the anterior gastrotomy was closed using the stapler. In the second patient, the cholecystectomy was completed without the need for additional trocars. Both operations were completed without complication and with minimal blood loss. The operative time was 96 minutes for the first case and 244 minutes for the combined cystgastrostomy and cholecystectomy. The mean post-operative length of stay for the 2 patients was 9 days.
Conclusion: It is our belief that a laparoscopic cystgastrostomy, utilizing a 3-trocar technique, is a safe and feasible approach for the internal drainage of persistent pancreatic pseudocysts in children. The endoscopic bipolar cautery device and the endoscopic stapler are useful tools to create the anterior gastrotomy and complete the anastomosis, respectively.
Laparoscopic-Assisted Right Hemicolectomy for Appendiceal Carcinoid Tumor in Children
Appendix is the most frequent carcinoid tumors locations in children. Diagnosis is generaly done on pathologic examination of the appendicular specimen. Simple appendectomy is generally a sufficient radical operation but in a 2 cm or larger tumor case right hemicolectomy is required. We reported 3 cases of laparoscopic-assisted hemicolectomy for large carcinoid appendiceal tumor in the pediatric population.
Cases Report
Case One: Astrid C., 13 years old, was refered for a carcinoid tumor discovered on the appendicular specimen. Appendectomy was performed by right iliac fossa incision. Pathological examination found a 2 cm large diameter carcinoid tumor of the appendicular apex. Tumor infiltrated submocosa, muscular and serosa layers, without nervous infiltration on immunohistochemy technic. Chest X-ray and abdominal computer scan were negative as 5 HIAA serum analysis. Right laparoscopic-assisted hemicolectomy was performed with 4 ports and an anastomosis realised by a 3 cm right upper abdominal transverse incision. Pathologic examination of the specimen found 31 hyperplasic lymph nodes without anomaly on 8 cm ileum and 19 cm colonic bowel resection. Post-operative course was unenventfull and the girl discharged on 4th operative day.
Case Two: Solveig L., 13 years old, was operated in our institution for acute appendicitis. Appendicular abces was found on laparoscopic procedure with epiploic and ovarian adhesions. On the specimen a 2 cm large appendicular carcinoid tumor infiltrated from the mucosa to the serosa without meso appendicular invasion was found. Right laparoscopic-assisted hemicolectomy was performed with the same procedure. Pathological examination of the specimen found 29 lymph nodes without carcinoid cells. Post-operative course was uneventfull and the girl discharged on the 4th day.
Case Three: Elias B., a 14-year-old boy, was opereted by right iliac fossa incision in our institution for acute appendicitis. A 1.8 cm carcinoid tumor was found on pathologic examination with meso appendicular involvment. A right laparoscopic-assisted hemicolectomy was performed with only 3 ports and an anastomosis performed by the previous abdominal incision in the right iliac fossa. Pathological examination found 19 normal lymph nodes on a 7.5 cm ileum and 18 cm colonic resection. Post-operative course was uneventfull and the boy discharged on day 4.
Conclusion: Laparoscopic-assisted right hemicolectomy is a safe option in children with appendiceal carcinoid tumor. The goal in this indication is to complete the appendectomy by a large bowel and lymph nodes resection. It can be easily realised by the laparoscopic-assisted procedure with an extra abdominal anastomosis performed by the previous right iliac fossa incision or in a small right upper abdominal transverse incision.
Minimal Invasive Management of Bile Duct Thermal Injury Following Laparoscopic Cholecystectomy
Introduction: Bile leakage remains a serious complication after laparoscopic cholecystectomy. Injury to the bile duct may be caused by laceration, transsection, excision, clipping, devascularisation, or thermal injury.
Case Report: A 13-year-old girl was admitted to the hospital because of bile stones. Laparoscopic cholecystectomy and postoperative course were uneventful, on the 5th postoperative day she could be discharged from hospital.
Three days later she was admitted again because of abdominal pain. Repeated ultrasound examination showed increasing free abdominal fluid.
Due to signs of biliary peritonitis on the 10th postoperative day laparoscopic revision was performed. Bile leakage of the choledochal duct in the region of the cystic duct stump (lateral injury to extra-hepatic bile duct or Siewert III) could be localised.
As the leak was very small, only a peritoneal drainage was inserted.
After an unsatisfying course with persisting secretion of bile (300 ml per day) ERCP was performed and after sphincerotomy a transpapillary endoprothesis was placed.
Further course was uneventful and the girl recovered completely.
Two months later the endoprothesis was removed; ERCP showed no stricture.
Conclusion: The risk of common bile duct injury varies between 0.4% and 0.6% after laparoscopic cholecystectomy.
In our case etiology is still unknown. We suppose, that our complication was caused by thermal injury due to the use of monopolar coagulation leading to the partial necrosis of the choledochal duct`s wall.
Time between operation and presentation of symptoms ranges from immediately after surgery to 3 months later.
In our patient first symptoms of biliary peritonitis appeared at the 8th postoperative day and finally endoscopic treatment was successful.
Laparoscopic Treatment of Gastric Duplications in Children
Background: Gastric duplication cyst is a rare anomaly that requires surgical resection. The objective is to analyze the usefulness and technical feasibility of completely laparoscopic treatment of gastric duplication.
Patients and Methods: Retrospective study of four patients diagnosed and treated for gastric duplication during the last 3 years in our center. We analyzed the prenatal diagnosis, localization, measurement, clinical presentation, age at diagnosis and surgical treatment, surgical technique, post-operative, and histological confirmation.
Results: Three of the four patients who underwent surgery had a prenatal diagnosis and intra-abdominal cystic mass detected on fetal ultrasound and fetal MRI.
The size ranged from 2 to 3 cm in diameter and were located in the fundus (two cases), lesser curvature (one case), and juxta-pancreatic (1 case). Surgical resection was through the laparoscopic approach, with a case made with DaVinci robotic surgery. The use of endo-staplers has proved very useful. The range of age at the time of surgery is between 10 days and 13 years. In the first case post-operative complications in the form of gastric perforation in bed marsupializations cyst that required reoperation. There was histological confirmation of gastric duplication cyst communicating not in all cases.
Conclusions: Gastric duplications are considered benign congenital lesions can be detected in fetal life through prenatal diagnosis. Currently, surgical resection is totally laparoscopic block of choice, regardless of size or location of the malformation.
Thoracoscopic vs. Thoracotomic Repair of Esophageal Atresia: A Retrospective One-Centre Study
Background: Treatment of esophageal atresia is challenging. Thoracoscopic correction was first reported in 2000 by Rothenberg. In our institution we started this technique in 2006.
Aim: To review our results regarding surgical correction of esophageal atresia by thoracotomy (group I) versus thoracoscopy (group II).
Methods: Retrospective chart review was performed of patients undergoing repair of esophageal atresia, admitted to our centre between January 2005 and July 2006 (group I) and July 2006–July 2010 (group II). Patient characteristics, surgical, and postoperative were compared between patients who underwent correction by right thoracotomy and patients treated thoracoscopically. Statistical analysis was performed using the Chi-square, Fisher's exact, or Mann-Whitney U test as appropriate. P < 0.05 was considered statistically significant.
Results: In the study period 40 patients underwent correction of esophageal atresia by thoracotomy (group I, n = 20) or by thoracoscopy (group II, n = 20). Gestational age and birth weight were comparable for both groups. Associated anomalies were present in 7 (4 group I vs. 3 group II) patients. All patients presented with a type C atresia according to Gross' classification, except for 2 patients in the thoracotomy group (type D).
Median [IQR] time in days between birth and surgery differed between both groups; group I 1 [1–2] vs. group II 2 [1–3] (P = .018). Operative time including anaesthesia was significantly different in favour of the thoracotomy group (P = .011).
Postoperative mechanical ventilation was comparable for both groups as was time to first enteral feeding. However, time to oral feeding showed a trend in favour of the thoracoscopic group; median [IQR] time to first oral feeding was 7 [4–12] days in group I and 5 [3–7] days in group II (P = .055).
Complication rate was comparable between both groups regarding: anastomotic stricture, acute life threatening events, recurrence of the fistula, and missed fistula in type D atresia. Esophageal dilatations for anastomotic strictures were performed in 9 patients in group I and 10 patients in group II of which 4 (group I) vs. 7 (group II) needed 3 or more dilatations. Two patients in the thoracoscopic group were diagnosed with mediastinitis due to anastomotic leakage.
Laparoscopic Nissen fundoplication was performed in 4 patients with life threatening events, due to gastro-esophageal reflux (2 in each group). Two of them were also treated with minimally invasive aortapexy because of severe tracheomalacia. Length of stay was equal in both groups.
Conclusion: Both surgical techniques show comparable results regarding postoperative course except for a trend in time to oral feeding. This could be explained by more emphasis on fast track postoperative care in the last period. Thoracoscopic repair of esophageal atresia is a feasible technique, although it requires a learning curve. In comparison to the open procedure, it has the same complication rate and has become standard of care in our centre. Long-term results are awaited in respect to esophageal function, scoliosis and cosmesis. To prove the outcome of thoracoscopically correction of oesophageal atresia, a RCT with experienced centres is recommended.
The Prevention and Treatment of Complications in Laparoscopic Choledochal Cyst Excision
Objective: To assess the effectiveness of laparoscopic congenital choledochal cyst excision with Roux-en-Y hepaticojenunostomy and explore the categories and preventions of its complications.
Methods: The clinical data of 75 children who had underwent laparoscopic choledochal cyst resection were retrospectively reviewed from June 2002 to May 2010 in our institute. The causes of intraoperative and postoperative complications and follow-up problems were analyzed.
Results: The total laparoscopic cyst excision and the intracorporeal hepaticoenterostomy were successfully completed in 74 children. 21 cases with biliary stenoses in the porta hepatis were treated by ductoplasty meanwhile. The conversion was required in 1 case due to intrapancreatic choledochocele involving pancreas and duodenum. The intraoperative or perioperative complications were oberved in 5 cases including portal vein injury in 1 case, temporary bile leakage in 2 cases, a torsion of the jejunal Roux loop in 1 case, and stress ulcer in 1 case. During a follow-up period of 3 months to 7.5 years, one case developed hepaticojejunal anastomotic stricture in a type cyst. The mortality rate was 0% in this series.
Conclusions: To minimize the risk of complications, total excision of the cyst is ideal, but a small proximal cuff of hepatic duct is retained for type cyst to aid in the hepaticojejunal anastomosis. A slit on one end of the stenotic ducts will render the anastomosis in an oblique orientation, widening the lumen for type cyst. Morbidity rates of laparoscopic intervention are comparable with the results of the open procedure. Laparoscopic excision and reconstruction can be safely performed in children with a choledochal cyst with satisfactory results.
Laparoscopically Assisted Roux-en-Y Duodenojejunostomy for Superior Mesenteric Artery Syndrome
Objective: To evaluate the effectiveness of laparoscopically assisted Roux-en-Y duodenojejunostomy for superior mesenteric artery syndrome.
Methods: From May 2003 to August 2010, 9 children (aged 6 to 13 years) with superior mesenteric artery syndrome underwent laparoscopic Roux-en-Y duodenojejunostomy. Among them, 3 were boys and 6 girls. The procedure was performed using 4 trocars, Treitz's ligament first was dissected, and the jejunojejunal anastomosis was made by exteriorizing the proximal jejunum through the umbilical incision. At last, the retrocolic Roux-en-Y duodenojejunostomy was done with the distal end jejunum and the section of duodenum which was enterectasis under the laparoscope.
Results: All procedures were completed successfully. Operative time was 2 to 3.5 h, and the blood loss was 15.2 ± 3 ml. The patients had complete resolution of their preoperative symptoms and a normal growth and development at 1–72 months follow-up.
Conclusions: Laparoscopic Roux-en-Y duodenojejunostomy is a safe and excellent technique for the superior mesenteric artery syndrome, and it may offer patients the benefits of decreased pain, a shorter hospital stay, and less postoperative disability.
Diagnosis of 46,XY Disorders of Sexual Development in Girls with Inguinal Hernia: A Call for Laparoscopic Hernia Repair
Introduction: XY,46 Disorders of Sexual Development (46,XY DSD) including Complete Androgen Insensitivity Syndrome (CAIS) and other rare disorders linked to androgen synthesis and androgen receptor function are characterized by a normal female phenotype as well as external genitalia but a male XY karyotype and testes. These disorders are associated with a high incidence of inguinal hernias.
We present a case with a girl with bilateral inguinal hernias, later diagnosed with an androgen synthesis defect.
Case: A 2-month-old girl with bilateral inguinal hernias and a right-sided palpable gonad was admitted for laparoscopic inguinal hernia repair. At surgery, on the right side structures resembling a vas deferens and testis were found next to the hernia sac. On the left side a small hernia opening and a vas deferens was noted in the inguinal canal, but the gonad was not possible to retract to the abdominal cavity. There was in addition no uterus or adnexa within the abdominal cavity. A right-sided laparoscopic gonad biopsy was performed and the hernias were repaired leaving the gonads in the inguinal canal bilaterally.
The patient was diagnosed with a 17-beta hydroxysteroid dehydrogenase type III-deficiency (HSD17B3 deficiency), causing a defect testosterone synthesis and a female phenotype. The patient later underwent bilateral gonadectomy.
Discussion: The HSD17B3-deficiency is a very rare condition resembling CAIS, both associated with a high frequency of inguinal hernias presenting in childhood. Different screening tools have been suggested to diagnose these patients at presentation of the inguinal hernia, including karyotyping all girls undergoing inguinal hernia repair, inspection of visible gonads at surgery and perioperative measurement of the vaginal length. Laparoscopic hernia repair in girls gives the opportunity to inspect the gonads and internal genitalia and diagnose these disorders in a routine clinical setup.
We propose a recommendation for the laparoscopic approach in inguinal hernia repair in all girls, especially those with bilateral hernias. This will now be routine in our department.
Laparoscopic-Assisted Excision of Giant Abdominal Lymphangiomas of the Small Bowel Mesentery
Background: Abdominal cystic lymphangioma (ACL) is a rare benign tumor arising from mesenteric, omental or retroperitoneal lymphatic system. In children, it can present as poorly symptomatic abdominal mass or, more frequently than adults, it can have an acute onset for rapid growth, bowel obstruction, inflammatory or hemorrhagic complications. The complete surgical excision is the treatment of choice, and recurrence for incomplete resection has been reported. When adherent to bowel loops, intestinal resection may be required. The authors report their experience with transumbelical laparoscopic-assisted excision of giant ACL
Patients and Methods: From 2006 to 2009, 2 male patients (age 13 and 3 years, respectively) were surgically treated for giant ACL, arising from the small bowel mesenterium. The first patient presented an asymptomatic 20 × 12 cm cystic abdominal mass with internal septa evidenced during a routine ultrasound. The second case presented with vomiting and intermittent abdominal pain; at ultrasound a 20 × 10 cystic mass was evidenced. Both patients underwent a three-trocar transumbelical laparoscopic-assisted excision of the giant ACL, with intestinal resection of 8 cm of jejunum in the second case.
Results: A macroscopically complete excision of the mass was achieved in both cases. The postoperative course was uneventful, and no recurrence was observed in the follow-up (54 and 12 months).
Conclusion Minimally invasive approach to abdominal cystic lymphangioma can be considered the treatment of choice, even in case of giant mass. Complete laparoscopic or lap-assisted excision has been both described as valid and safe approach in children, even in emergency. Laparotomic excision should be reserved to cases with doubt of malignancy, sclerotherapy to unresectable lesions.
Laparoscopic Repair of Giant Congenital Paraesophageal Hernia
Background: Paraesophageal hernias are most commonly seen in patients who have previously undergone a Nissen fundoplication. Congenital paraesophageal hernias are particularly rare. We describe a successful minimally invasive approach in two patients with a giant congenital paraesophageal hernia.
Case Reports: The first child was a 5-year-old boy who presented with chronic anemia and a poor appetite. A large cystic mass in the right hemithorax proved, on an upper GI series, to represent near-total herniation of the stomach into the chest. The second patient, a 13-month-old girl, presented with persistent vomiting for over a month. Again, diagnosis was made with an upper GI series after a chest x-ray suggested the presence of a giant paraesophageal hernia.
Operative Technique: A periumbilical incision was made for initial trocar insertion. The abdomen was insufflated to 10 mm Hg. Most of the stomach was seen herniated into the thorax through a large diaphragmatic defect in both cases. No additional abnormalities were observed. Three additional trocars were placed (bilateral subcostal and epigastric). The stomach was fully reduced into the abdomen, and the peritoneal sac was dissected circumferentially along the edge of the diaphragmatic defect, thereby exposing the crura. No attempt was made to resect the intrathoracic portion of the sac. Once the hiatus was fully exposed, the posterior crural defect was closed with interrupted silk sutures. Additional sutures were placed anteriorly over a bougie to complete narrowing of the hiatus. A full 360 degree Nissen fundoplication was performed in a standard fashion. Anchoring sutures were placed to secure the wrap to the diaphragm.
Results: The first patient recovered well and has had no complications from his surgery. The second child had a partial recurrence of her hernia 14 months after repair, requiring reoperation. This was also performed successfully laparoscopically. She has had a very small, but persistent hiatal hernia, which has been asymptomatic.
Conclusions: Giant congenital paraesophageal hernias are rare. A laparoscopic approach to repair is feasible, even in very young children.
Fiberendoscope Treatment of Intussusception in Children
Background: The non-operative treatment of intussusceptions does not enable to evaluate completely injury degree of intussuscepted intestine and determine possible etiologic factors.
Aim: This study describes endoscope treatment of intussusceptions and gives more deep understanding of the factors contributing to it.
Methods: 92 colonoscopies were performed under general anesthesia in children from 6 to 14 months of age, between 1985 and 2010. All patients were divided in 4 groups depending on the length and severity of illness. I group–11 patients (11.9%) were admitted in 6 hours after disease onset, II group–32 patients (34.7%) in 12 hours, III group–28 patients (30.4%) in 24 hours, IV group–21 patients (22.8) in 30 hours. For the majority of patients' illness was advanced because of intestinal dyspepsia on a background of viral infection or diet disturbances. There were performed endoscope pneumatic reductions after visual assessment of intussuscepted bowel.
Results: In the I group intussusception treatment by colonoscopy was done in 11 (100%) patients; in the II group, 32 (100%) cases; in the III group, 26 (92.8%); and in the IV group, 15 (71%) cases. Endoscope treatment was done totally in 86 from 92 (93.4%) cases. The valve of Baugin and 10–15 cm in length terminal ileum were observed usually after endoscope pneumatic reduction. Flat-form, malclosed, slit-like, immature valve of Baugin with hemorrhages was visualized in all cases. There was condition of inflammation in distal ileum, with hypertrophic lymphoid follicles, that were distributed in high density fashion. The ileitis was affirmed morphologically. Endoscope treatment was last 20–25 minutes and there were not any complications.
Veryfication of pediatric patients according to disease onset and endoscopic disintussuception.
Conclusions: Intestinal dysfunction and viral infections are well-known causes of intussusception in children under 2 years old. Lymphoid follicles are usually hyperplasive in childhood and infections may cause progression of hyperplasia which reduces the lumen of ileum and makes the centers of intestinal infringement. On the basis of our investigations we made suppose, that the viral infections in conjunction with functional immaturity of Baugin's valve, with III degree hyperplasia of lymphoid follicles in terminal ileum might be important etiologic factors of intussusception in childhood.
Functional Evaluation of Colonic Conduit in Esophageal Replacement: Long-Term Follow-Up and a New Grading Score of Motility
Background and Objective: Over the last 30 years more than 850 esophageal replacements have been performed in our department mostly for caustic injuries and esophageal atresia. The technique has evolved from gastric pull-up to colon replacement, initially subcutaneously, then retrosternally. In the last 13 years transhiatal oesophagectomy with posterior mediastinal colon replacement was started.
This study was designed to evaluate the long-term outcome of colonic conduit used for esophageal replacement. Two main items were concerned about the neo-esophagus; motility together with clinical status.
Patients and Methods: Thirty cases of esophageal replacement were studied from December 2007 to June 2010 regarding clinical and functional outcome. All patients had one year or more for follow-up postoperatively. Informed consent provided by parents and acceptance of the ethical committee of the institute were obtained. Clinical evaluation included vomiting, aspiration, dysphagia, dyspnea, weight loss, and chest infections. Motility was evaluated by manometeric and Contrast studies of the conduit. Introduction of the pressure catheter was done during endoscopic examination and the study was done at least six hours after recovery from anesthesia. Procedure was done in supine position to give time for the bolus to reach stomach and excluding the effect of gravity.
Results: Most of the children (26 cases) scored between 80–100% Karnofsky score (Good/Excellent QoL) while only 4 cases scored 60–70% (Fair QoL). Clinical records included heart burn (2 cases/6.7%), dysphagia (5 cases/16.7%), food impaction (1 case/3.3%) and adhesive intestinal obstruction (2 cases/6.7%). Most of these complications were intermingled with each other, i.e., combined in some cases and solitary in others. Most of complications were managed conservatively.
Primarily, manometeric graphs of most of cases (26) showed +ve motility (86.7%). The variation between the findings was noticeable and a new grading system, perhaps more accurate in determining the propagated waves was created that included grades 0 to IV. Accordingly, eleven cases (36.7%) showed [grade II] motility, 15 cases (50%) showed [grade I] motility and only 4 cases (13.3%) showed complete absent motility [grade 0]. However, no case showed neither grade III nor IV motility. The Slow transit by contrast imaging was recorded in 5 cases (16.7%).
Endoscopic findings included three cases (10%) of redundancy; one of them showed also upper cervical anastomosis stricture combined with mild degree of hyperemia. Another case of redundant colonic conduit had lower colo-esophageal anastomosis narrowing which responded to dilatation. One case (3.3%) showed mucosal ulcer in the residual lower part of the esophagus caused by reflux. However, 25 cases (83.3%) were found comparable to normal colon with no abnormal findings.
Conclusions: Perfect conduit for replacement of the native esophagus does not exist. Motility is present in the colonic conduit but by the nature of colonic physiology, i.e., in respose to bulk of swallow. Currently, there is no proof that it imitates esophageal motility after replacement. Yet, Colonic conduit for esophageal replacement is an acceptable substitute functionally and clinically presented by good quality of life post-operatively on the long-term follow-up.
Laparoscopic-Assisted Excision of Choledochal Cyst: A Single Centre Experience
Background: Choledochal cysts are rare congenital anomalies in which there is cystic dilatation of the biliary tree. Excision of the cyst with Roux en Y formation is advised and this is traditionally performed via laparotomy. In recent years there have been increasing reports describing a laparoscopic repair. We began performing laparoscopic-assisted excision of choledochal cyst with extracorporeal roux en Y formation in 2002 and report our experience.
Methods: A retrospective case-note analysis of all laparoscopic-assisted choledochal cyst excisions was performed.
Techniques: A 5 mm or 10 mm port was used at the umbilicus (depending on the size of patient) with two 3.5 mm or 5 mm working ports, one on either side (the right port slightly lower than the umbilicus and the left port slightly higher). A Nathanson liver retractor was used and a further 3.5 mm or 5 mm assistant port was usually placed in the left flank. Once the cyst had been defined and the gall bladder taken off the liver, the distal end of the duct was clipped. An extracorporeal roux en Y loop was created via the umbilical port. The length of loop ranged from 11 cm to 30 cm. Retro-colic placement of the Roux loop was performed in the majority of cases. The choledochojejunostomy was completed laparoscopically after re-establishing the pneumoperitoneum.
Results: Eight patients underwent laparoscopic-assisted excision of choledochal cyst between 2002 and 2010. There were five female and three male patients. Median age at presentation was 9 months (range 0 to 13 years). Two patients presented antenatally; three with jaundice and failure to thrive; one with abdominal pain and jaundice; and one cyst was an incidental finding on abdominal ultrasound scan. There were 6 type I choledochal cysts and 2 type IV cysts according to the Todani classification.
The first two patients in the series were converted to an open procedure due to difficulty visualising the distal common bile duct. One of these patients had previously undergone laparotomy resulting in dense supracolic compartment adhesions. There were two post-operative bile leaks requiring laparotomy. One was in a patient who required conversion to an open procedure and the other in a laparoscopic-assisted case. Mean hospital stay was 11 days (range 4 to 17). Median follow-up was 35 months (range 2 weeks to 7 years). Four patients had deranged liver function tests pre-operatively but all liver function tests normalised during follow-up. Post-operative ultrasound scan of the liver and residual ducts was normal in 7 cases and showed mild residual dilatation at the distal end of the common hepatic duct in one case.
Discussion: In our series, the first two patients required conversion to an open procedure. 5 patients underwent laparoscopic-assisted excision without complication. Laparoscopic-assisted excision of choledochal cyst can be performed safely in centres with a small number of cases per year, providing advanced laparoscopic skills are available for the technically difficult anastomosis. Retro-colic placement of the Roux loop facilitates a laparoscopic anastomosis.
Does the Topical Administration of Steroid Reduce the Number of Balloon Dilatations Required in the Management of Oesophageal Stricture?
Introduction: Despite a lack of good evidence, steroids are often used in conjunction with balloon dilatation in the management of oesophageal stricture. Published literature describes the administration of steroids via three standard routes; intravenous, oral and direct injection into the stricture.
Our centre has recently introduced topical administration of Budesonide as part of our routine management of oesophageal stricture. Our early impression is that topical steroids have proven to be beneficial, particularly in resistant strictures secondary to caustic injury.
Hypothesis: We believe that the use of topical steroid therapy in the management of oesophageal stricture may reduce the number of oesophageal dilatations required, due to the reduced frequency and severity of re-stricturing.
Method: A retrospective case review was performed to identify all patients who had undergone oesophageal dilatation with administration of topical Budesonide.
Results: 12 patients were identified. These included strictures secondary to caustic injury, chronic inflammation (GORD, eosinophilic oesophagitis), anastomotic stricture secondary to repair of trans-oesophageal fistula and oesophageal atresia, oesophageal web, and oesophageal perforation secondary to Hodgkin's Lymphoma.
Budesonide was commenced following initial dilatation in 6 patients, preventing comparison of clinical course pre-administration. Of the 6 patients where clinical course could be compared before and after administration, only 2 showed a reduction in interval between dilatations following topical steroid therapy. Patients who have received topical Budesonide do, however, appear to have improved clinical outcome.
Discussion: This study is limited primarily by the small number of patients who have received topical Budesonide in their management of oesophageal stricture. Due to this being a relatively new intervention, we have limited long-term follow-up. Although the data currently available does not provide strong support for our hypothesis, our positive clinical experience has led to the incorporation of topical Budesonide in our routine management of oesophageal stricture. We suggest that this should further be investigated with a randomised-controlled trial.
Video-Assisted Surgery in the Management of Parasitic Abdominal Cysts
Hydatid cyst is a parasitic disease caused by the tapeworm Echinococcus granulosus (EG). Incidences in Chile have been reported ranging from 1.9 per 100.000 to 43 per 100.000 inhabitants in endemic areas. Mortality associated with this disease is 6.2 per million. Preferred location of hydatid cyst is the liver (48%), followed by the lung (30%). It can occur at any age, been frequent in the pediatric population. Surgical treatment should be indicated when the cyst is larger than 5 cm diameter or when is complicated by rupture or infection. Medical treatment with albendazol may be added to decrease risk of recurrence. Different surgical options have been described cystostomy and drainage, cystostomy and capitonnage, cystectomy and partial liver, lung or spleen resections, having different rates of complications and recurrence. The purpose of this report is to show our experience in the surgical management of abdominal hydatid cyst by minimally invasive surgery (MIS).
We retrospectively reviewed 4 cases with abdominal hydatid cysts, 3 hepatic and 1 spleen cysts. Two male and 2 female, 5 to 10 years old. Presenting symptoms was fullness and the presence of an abdominal mass. Diagnosis was confirmed preoperatively in 3 patients by the presence of a liver cyst (1 case, Type CL and 2, type CE1; Acta Tropica 2003; 85: 253–61) in radiologic images (Ultrasound and/or abdominal tomography), those 3 patients presented with eosinophilia and presence of EG IgG antibodies using enzyme-linked immunosorbent assay. Plain chest radiography was done to rule out lung hydatid cyst. Patients were treated with albendazole 10 mg/K/day, 1 month prior to the operative procedure and 2 months after. Hydatid cyst was not suspected preoperatively in the patient with the spleen cyst; diagnosis was performed during laparoscopic exploration, this patient received albendazol for 2 months after the surgical procedure.
MIS was planned and completed in all cases, our surgical option was cystostomy and drainage in 3 cases (2 liver/1 spleen) and 1 hepatic cyst was treated with cystostomy and capitonnage, 2 to 3 ports were used to perform a video-assisted surgery. A 2 cm incision was performed, the cyst was exteriorized through the incision and was isolated surrounding it with impregnated gauzes with 30% saline solution. Two 14 G needles were placed carefully through the cyst wall, one for constant aspiration of the cyst content and the second for irrigation of 30% saline solution, that was retained in the cyst for at least 3 minutes. Treatment was completed after the cyst was sterilized. There were no intra-operative or postoperative complications. Hospital stay was 24 hours. No recurrences were observed during follow-up period.
Selected cases can be benefit of MIS combined with medical treatment; video-assisted technique is effective in the eradication of abdominal hydatid cysts, with no complications in this series.
Omental Multicystic Mesotelioma: The Laparoscopic Approach
Introduction: Among the diagnoses of abdominal pain and abdominal cystic tumors in children, omental cysts should be considered, characterized by a single or a few large cyst clusters with cuboidal epithelium suggesting inclusion cysts. An uncommon disease before age 18 is the omental multicystic mesothelioma (OMM), with multiple cysts of various sizes forming clusters, with the possibility of spreading benign implants over the peritoneum. We found fewer than 150 cases ever published in the extensive literature, mostly in adults. The objective is to present the first problable case of a child presenting OMM successfully treated laparoscopically.
Case Report: A 10-year-old boy was admitted with a history of 2 previous episodes of acute abdominal pain at the mesogastrium, vomiting and no other symptoms. Imaging tests included radiography, ultrasonography and computed tomography, showing an irregular multicystic mass of uncertain origin, in close relation to the intestines at the mesogastrium and the left side of the abdomen. Laparoscopy revealed a multicystic omental tumor, containing serous amber material similar to that from lymphangiomas, with two areas of prior twisting and some cystic implants in the pelvis. Using three ports (10, 5, and 5 mm), total omentectomy was performed by removing the entire tumor with free margins, as well as removal of the implants through the umbilicus. The patient was discharged the following day and has been asymptomatic after one year of follow-up. The aesthetic is excellent and the periodic imaging has shown no recurrence. The pathological report required immunohistochemistry to confirm the diagnosis of OMM by the absence of endothelial cell markers and PGF (excluding lymphangioma), negative for glandular markers (excluding mesenteric and classic omental cysts) and positive for protein related to Wilms tumor.
Conclusion: The OMM can be found in children, diagnosis is facilitated by immunohistochemistry and can be successfully treated by laparoscopy.
Cardiac Mucosa and Gastroesophageal Reflux Disease in Pediatric Patients
Background: Cardiac mucosa has been shown to be an abnormal metaplastic epithelium that results from the effects of gastroesophageal reflux on esophageal squamous epithelium. The aim of our study was to identify the relationship between the presence of cardiac mucosa in a pediatric population with clinical evidence of gastroesophageal reflux disease.
Methods: We conducted a retrospective study at Valley Health System (Ridgewood, NJ) were a total 186 endoscopies were performed at this institution from 2006 to 2008. Only 93 patients had complete endoscopic and clinical records available. The presence of cardiac mucosa, oxyntocardiac mucosa and intestinal metaplasia was assessed with our biopsy protocol. These results were compared with other histologic features, such as esophagitis, gastritis, Helicobacter pylori, and the presence of goblet cells, and more importantly with clinical symptoms of the patients.
Results: Our results show that forty nine (52.6%) of the pediatric patients had evidence of carditis defined by the presence of cardiac mucosa, oxyntocardiac mucosa or both. Eight (8.6%) patients had no evidence of carditis, despite clinical evidence of GERD and 32 (34.4%) had inadequate biopsies. Most common indication for EGD was abdominal pain. The mean age was 9.4 years (1 month–21 years). No statistical difference was found between carditis in males or females (P = 0.701). All patients with carditis have associated either acute or chronic eosphagitis. Only 43 (46.2) patients with carditis had associated acute or chronic gastritis. Two patients with carditis had H. pylori infection. One patient had carditis with intestinal metaplasia.
Conclusions: In conclusion >50% of the patients with clinical evidence of reflux disease have presence of metaplastic changes represented by cardiac mucosa that is associated with either acute or chronic esophagitis in all patients. The presence of cardiac mucosa, oxyntocardiac mucosa or the both is an abnormal epithelium that occurs in the esophagus secondary to gastroesphagela reflux disease (GERD). The prevalence of carditis is higher in patients with clinical evidence of GERD.
Miscellaneous
Paraovarian Tumors in Children: An Underdiagnosed Entity
Background: Paraovarian tumors constitute 10% of pediatric adnexal pathology, but are rarely reported in the literature. Identification of paraovarian tumors may be challenging, and result in needless dissection and iatrogenic injury to both ovary and tube.
Aim: To analyze a series of paraovarian tumors encountered intraoperatively, examine their salient features and address diagnostic and management considerations.
Material and Methods: A retrospective case series which includes 24 girls who underwent surgery for paraovarian tumors during an 10-year period (2000–2009).
Results: The presenting symptoms were adnexal torsion (N = 12, 50%), symptomatic adnexal mass without torsion (N = 11) and giant abdominal cyst (N = 1). The diagnosis was made preoperatively in only one patient. All paraovarian tumors but one were correctly identified by meticulous intraoperative evaluation. Adnexal sparing surgery was performed in 23 patients and adnexectomy was undertaken in one.
Conclusion: Paraovarian lesions are rarely diagnosed preoperatively. Intraoperative diagnosis, especially of a large mass or displaced adnexal structures may be challenging. Correct identification of these tumors is the key to appropriate management and adnexal preservation during surgery. It hinges on a high index of suspicion and on meticulous inspection.
Prospective Comparative Assessment of Ultrasonography and Laparoscopy for Contralateral Patent Processus Vaginalis in Inguinal Hernia Presented in the First Year of Life
Background and purpose: Contralateral inguinal exploration in children with unilateral inguinal hernia is still controversial. The aim of this study is to present an evidence-based justification for contralateral inguinal exploration among our population after comparing ultrasonography and laparoscopy.
Methods: Over three years period 246 patients, (207 boys and 39 girls) with unilateral inguinal hernia who presented in the first year of life underwent US examination using a 10-MHz linear transducer. Operative trans-inguinal contralateral laparoscopic exploration was done in all cases. Results were compared prospectively as regard sensitivity and specificity of US and laparoscopy.
Results: We showed left side incidence in males of 50.7% while right side predominate in females (69.2%). Prematurity represented 24.6% of males only and 30.8% among left sided cases. 64.6% of cases diagnosed in the neonatal period. We consider positive patent processus vaginalis (PPV) US when types I–III according to Toki's et al* were reported. US confirm patent PPV in 30.5% of cases whom confirmed laparoscopically in 91.7%. Sonographic assessment of contralateral PPV gve sensitivity of 91.7% and specificity model of 87.7%. We have positive laparoscopic exploration of 35.8% among all groups. The cost of negative laparoscopy is 50$ while positive laparoscopy costs 100$ as compared to second admission which costs 500$.
Conclusions: Since in our community there is high incidence of consanguinity, preoperative assessment of contralateral hernia should be considered in cases presented in the first year of life and premature infants. US give is a highly sensitive tool in experienced hands to diagnose contralateral hernia. Laparoscopic exploration is safe, rapid and sure method of diagnosis even in infants. We recommend the laparoscopic exploration in all cases presented in the first year of life as saving second admission with significant lowering of costs.
Transaxillary Subcutaneous Endoscopic Excision of a Lymphangioma of the Neck
Introduction: Benign neck lesions in children are common and most of them need surgical excision. Scarring as a result of the surgery can be unsightly and disturbing for the patient and parents.
The transaxillary approach transfers the scarring associated with neck surgery to the axilla area.
Case Report: A 6 month old female patient presented at our institution with a 3 cm × 2 cm cystic mass in the left posterior triangle of the neck. An MRI scan confirmed the diagnosis of a lymphangioma.
A 5 mm incision was made parallel to the lateral border of the pectoralis major muscle. A 5 mm camera port was used and secured to the skin with a nylon suture. A 30° telescope was inserted and used as a dissecting tool. Two additional 3 mm ports were inserted 3 cm from each side of the camera port, and were used for the laparoscopic instruments.
This lymphangioma was completely excised during this procedure. Operating time was 55 minutes.
Conclusion: This minimal invasive procedure offers an easy and effective way to remove this small lymphangioma whilst avoiding neck scarring. This minimal invasive technique should, however, be avoided in patients with large or complex lymphangiomas which extend around vital structures in the neck.
“Sign here Please”: An Audit of the Consent Process in a Paediatric Surgical Department
Abstract Withdrawn
Prospective Assessment of Laparoscopic Herniotomy in Children: Tertiary Center Experience from Developing Country
Introduction: Inguinal hernia is a common pediatric problem, and herniotomy has been its standard of care. Laparoscopy became widely used in the management of pediatric inguinal hernia (PIH) due to its increasingly wide range of advantages.
Aim of the Work: The aim of this work is to assess prospectively laparoscopic herniotomy in children in a tertiary center with limited resources in developing country.
Patients and Methods: 56 consecutive children with unilateral PIH were treated by the same group along 18 months period from July 2008 till March 2010. All cases were subjected to laparoscopic exploration followed by laparoscopic herniotomy as a day case surgery. Laparoscopic herniotomy was performed as closely as possible to the classical open technique. Exclusion criteria included: prematurity, less than 6 months of age, irreducible, recurrent or bilateral cases. Operative findings and post operative results and complications were assessed. The patients were followed for a period ranged between 6 and 24 months.
Results: We have 56 cases with male: female as 42:14 and 12 of them presented in the first year of life. Age ranged between 6 months and 15 years. 32 presented as RT sided hernia with 12 associated with contralateral patent processus vaginalis (PPV) as compared to 24 cases Lt sided with 10 contralaetral PPV upon laparoscopic exploration. 2 cases show adhesions and 2 cases with direct defect that dealt with laparoscopically in the same session. Hydrocele of the hernia sac reported once. Operative time ranged between 18 & 40 min in unilateral cases (mean: 20.5 min) while reported to be between 25 & 60 min in bilateral cases (mean: 42.5 min). All operations were completed laparoscopically without conversion. Post operative pain last for a period ranged between 6 and 20 hours (mean: 11.2 hours). Patients regained peristalsis by a mean time of 7 hours post operatively. Two cases of wound infection were reported and treated conservatively. No case of recurrence, testicular atrophy or hydrocele was reported in the follow-up period. Cosmetic outcome was excellent.
Conclusions: Laparoscopic inguinal herniotomy is a feasible and safe in unselected pediatric cases. It provides a superior diagnostic tool to diagnose contralateral hernia or rare types of hernias that can be dealt with in the same session with minimal post operative complications even in developing countries. No special strategies were needed for laparoscopically detected bilateral hernias, as trocar placement could be identical for any side or hernia type. Laparoscopy proved to be a superior alternative to the open repair of inguinal hernias in children since it provides an excellent view on the cord structures and they can be guarded well during the procedure. Larger studies and long-term follow-up are needed to support our encouraging results.
Minimally Invasive Surgery (MIS) of Pediatric Solid Tumor in Infants Under One Year of Age
Background: There is only limited experience of using the minimally invasive surgery (MIS) technique in resecting pediatric solid tumors, specifically in infants. In this paper, we report our experience of laparoscopic or thoracoscopic resection for pediatric solid tumors in infants under one year of age.
Methods: A retrospective review was undertaken of all MIS performed in infants under one year of age with solid tumor between 2005 and 2010 at University of Ulsan College of Medicine & Asan Medical Center.
Results: Over a 6-year period, there were 9 patients who had undergone MIS for tumor resection. The median age and weight at the time of surgery were 1 month (range, 9 days to 8 months) and 5.5 kg (range, 2.7 kg to 9.4 kg). In five patients, the age at the time of surgery was under 1 month of age. There were 4 adrenal tumors, 1 liver mass, 2 intradiaphragmatic masses, and 2 intrathoracic masses. The median size of tumors was 4 cm (range, 2.5–9 cm). The median operation time was 180 minutes (range, 90–250). On average, four ports (range, 3–6) were used and all patients had undergone a successful MIS tumor excision. All patients required the enlargements of umbilical or thoracoscopic port sites and no one required additional incision. There was no postoperative complication encountered. On an average follow-up of 16 months, there was no recurrence observed, even in the 5 patients with malignant tumors. All patients had good cosmetic results.
Conclusions: In infants under one, a variety of pediatric solid tumors can be resected safely by the MIS technique. And this has effective and better cosmetic results.
Evaluation of Web-Based Seminars as a Means of Continuing Medical Education
Background: Continuing medical education (CME) sessions have been shown to impact professional practice and healthcare outcomes; however, the use of web-based seminars, as a means of educating physicians, has not been well defined. In this project, we evaluate the utility of web-based seminars to provide CME.
Study Design: An eight-question survey was developed to better understand the CME habits of physicians. Participants were given a total of 10 minutes to answer the eight questions at a recent CME conference. Responses were entered from remote locations using the participants' personal computers. The incidence for each response was calculated and recorded immediately after the response time ended.
Results: A total of 76 participants responded to the survey. Among the responses, 85% of participants felt web-based seminars were a better use of their time than on-site seminars. Twenty-three percent indicated that they were more engaged by the web-based format versus on-site, 34% indicated they were more engaged by on-site seminars, and 43% stated they had no preference. Eight percent preferred on-site seminars to web-based seminars, and 7% had no preference. Finally, 84% of participants believed this symposium would change their practice in some way.
Conclusions: This study suggests that there exists a major interest in expanding the availability of CME sessions by utilizing the Internet for web-based symposiums. Given the many benefits of online CME sessions, there is also a definite need for these symposiums, and we are likely to see an increase in both attendance and the number of seminars offered over the coming years.
Implementing Dry-Lab Training in Minimal Access Surgery in a Children Hospital
Aim: To establish an in-house minimal access surgery (MAS) skills training laboratory for surgical trainees within a specialist children hospital.
Methods: A paediatric surgical fellow with previous research and teaching experience in surgical ergonomics was tasked to set-up the laboratory. A store room was allocated within the clinical building. Reusable MAS instruments identical to those used in the main theatres were obtained. Invitations were sent to all surgical trainees within the hospital to take part in MAS training sessions. A mid-week afternoon was scheduled for the training sessions when the clinical fellow did not have fixed clinical commitments and the department activities were low. Additional sessions were arranged at mutually convenient times. Attendance was not compulsory. All participants were given an introductory talk (overview of MAS instrumentation and equipment, mechanical and visual limitations, optimal personnel and port positions especially in avoiding paradoxical movements) followed by demonstration and hands-on exercises on basic manoeuvres and suturing/knot-tying under close supervision by the fellow. Exercises include transferring paper-clips, feeding paper-clips into a cotton tape and cutting a circle from the outer glove of a double glove model. The participants were asked to complete each task within 5 mins and number of errors was recorded. Various suturing and knot tying techniques were demonstrated and practised using synthetic materials.
Results: Between December 2009 and September 2010, 22 formal sessions took place (12 scheduled, 10 ad hoc) with one to three participants each. In total there were 41 participant episodes by 27 participants who were mostly from the general paediatric surgery and paediatric urology departments. Other participants include 4 overseas paediatric surgical visitors, a spinal fellow, a gynaecology visiting fellow and 2 medical students. Most only managed a single session, though some with 2–3 sessions with one SHO managed 7 sessions in total. Completion time and error rate improved with subsequent sessions.
Discussion: All participants found the session(s) helpful. However, time constraints were encountered by the participants and the fellow (who was also on the registrar rota) mainly due to patient care commitments. Access to the laboratory was allowed only under supervision to ensure the equipment was not misused but this had limited the unscheduled access which would be useful, e.g., “warm-up” knot-tying practice prior to fundoplication. While it is possible to set-up a MAS skills laboratory for training purposes in a children hospital with few surgical trainees, consideration needed to be taken into account with regards to scheduling of protected training sessions with dedicated supervising staff. A skills laboratory coordinator (e.g., research nurse) would be useful to supervise the practice sessions to be joined by surgeons to supervise specific scheduled training sessions. A structured training curriculum is to be developed and will have an important role for future mandatory training and assessment purposes.
Life and Health Sciences Research Institute (ICVS), Braga
Background and Aim: Gaining skills in laparoscopic surgery requires a lot of training. Besides in vivo training, surgeons have to spend a great amount of time practicing in simulators. Various box simulators have been presented, but most of them are expensive or difficult to construct. The aim of this study was to assess assembling simplicity of a homemade low cost simulator and its performance when compared with common commercial training boxes.
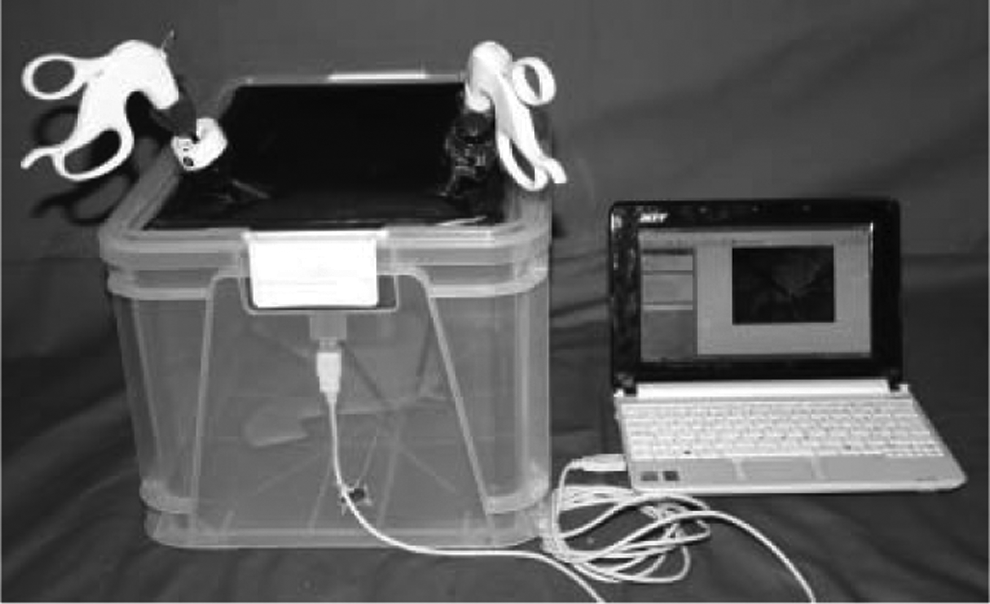
Material and Methods: An endoscopic surgery simulator was assembled in 5-steps using easy-to-find cheap materials (a transparent plastic box, a webcam, a USB cable, adhesive tape, Velcro tape, and a rubber sheet) with an estimated total cost of €35. The assembling steps and the simulator were presented to 30 surgeons (8 residents and 22 specialists), from various specialties, such as pediatric surgery, general surgery, gynecology, and urology. The participants assessed the trainer using common endoscopic training toys or ex-vivo tissue. Then, they completed an anonymous query about the difficulty of constructing the simulator, the ability to build their own simulator, the total cost of the simulator, the need of having one, the advantages and disadvantages of the simulator comparing to other commercial simulators they had tried using a scale from too difficult to too easy.
Results: 83% found the simulator really easy to build. Every participant felt that he/she could do the same simulator themselves. 63% answered that it is very important to have a simulator of your own for initial laparoscopy training. 97% agreed that the simulator was cheap. Comparing to other commercial available box simulators, the majority of participants found the homemade simulator easier to mount and dismount, easier to transport, easier to clean, and easier to use when practicing alone. The majority found quality of light, image, material resistance, and overall endoscopic environment at least as good as the commercial available box simulators they had experienced.
Conclusion: Anyone interested in laparoscopic training can build its own simulator for a small amount of money.
Laparoscopic Splenectomy: Which Technique?
Aim of the Study: Laparoscopic splenectomy is the gold standard for the removal of spleen in both adults and children. This audit is a retrospective review of SCH records, regarding laparoscopic splenectomies and related transfusion requirements, postoperative sepsis and prophylactic antibiotic therapy.
Patients and Methods: Retrospective study of the hospital records from January 2002 to September 2010 for the patients who underwent laparoscopic splenectomy.
Results: 24 cases laparoscopic splenectomies, 11 f (46%) and 13 m (54%), elective admissions.
In one case a single port technique has been used.
Reason for splenectomy: uncompensated haemolysis 18 cases (76%), thrombocytopenia 4 cases (16.66%) and splenic cyst 2 cases (8.33%).
Underlying Condition: Hereditary spherocytosis 14 cases (58%), splenic epidermoid cyst 2 cases (8%), autoimmune haemolytic anaemia 4 cases (17%) and chronic ITP 4 cases (17%).
Preoperative transfusion requirement was necessary in 10 cases, most of them multiple (with RBC), one with platelets.
One case with postoperative sepsis (pneumonia) and postoperative bleeding, requiring blood transfusion 2U. In 3 of the cases a Pfannenstiel incision to remove the spleen was performed (12.5%) one case was hand-assisted laparoscopic splenectomy.
Concomitant laparoscopic cholecystectomy and splenectomy was performed in 3 cases (12.5%). There were 7 cases with gallbladder pathology (29%).
In 4 of the cases accessory spleens were found (17%). One case with recurrent ITP secondary to splenosis required reintervention after 2 years for the removal of multiple splenunculi, laparoscopic/converted to open (previously reported).
Time from the start of surgery until PACU varied from 95 minutes to 365 minutes with a median of 191.5 minutes.
For the division of the splenic hilum a Stapler was used in 3 cases (13%), a further 2 of them with partial splenectomies for splenic cyst, and Ligasure in 21 cases (87%).
Types of retrievers to remove the spleen: Endobag 9 (39%), Endocatch II (Covidien) 12 (53%), hand-assisted laparoscopic splenectomy 1 (2%), Lapsac (Cook) 1 (2%). Incidents: 2 of the Endocatch bags ruptured.
All patients were discharged on prophylactic antibiotic (Penicillin).
Hospital stay varied between 1 and 10 days with an average of 3.33 days.
Conclusions: Laparoscopic splenectomy in children is safe. Division of the splenic hilum with Stapler may be quicker than with vessel sealing technology. The ideal bag retrieval system has yet to be developed. Single port technique may become the future standard.
Retroperitoneal Approach in a Peculiar Case of Gerota Mass
Introduction: The retroperitoneal approach is accepted for a wide spectrum of surgical procedures in paediatric age like total or partial nephrectomy, spermatic vessel ligation, uretero-plasty, retrocaval ureter, stone disease and small adrenal tumors excision.
Mini-invasive procedure must respect in any case the oncological protocols and principles to avoid neoplastic dissemination and recurrence.
We report the ablation of an inusual perineal mass enbedded in the Gerota fat, carried out with retroperitoneal access.
Case Report: A 13-year-old boy without major medical problem was referred to our centre after occasional detection of pararenal mass during radiological examination for pneumonia.
MRI and CT scan showed a well delimited mass inside the Gerota fat, located on the lateral side of the right kidney, measuring 40 mm × 38 mm.
After oncological counselling and radiological review of all the imaging examinations, surgical excision of the mass was strongly recommended because of lack of definitive diagnostic criteria.
The patient was placed in the lateral decubitus on the left flank. We used a 10 mm Hasson trocar was positioned below the 12th rib on the anterior axillary line and 2 operative trocar of 5 mm. Dissection was carried out with Ligasure® and the mass radically excised without ropture or spillage and extracted inside a 10 mm endo-bag thorough the Hasson port site. The patient was discharged 3 days after surgery. The histological examination of the mass was suggestive for an unusual localization of intermixed neuroblastoma.
Discussion: MIS in pediatric oncology requires experience in major oncologic surgery and high skill level in pediatric endosurgery.
The peritoneal approach, following the principles of oncological surgery, is feasible also for peculiar tumour, like the case described.
Transaxillary Subfascial Endoscopic Approach for Persistent Muscular Torticollis in Children
Background: The endoscopic approach is a technical innovation for release of the sternocleidomastoid (SCM) fibrosis in muscular torticollis, where operation scars can be hidden at less conspicuous areas, e.g., at the axilla and hair-bearing scalp. Since the SCM muscle is located beneath the investing layer of deep cervical fascia which is reported to continue to the fascia of the pectoralis major, the aim of the study was to describe and evaluate the preliminary result of transaxillary subfascial approach for persistent muscular torticollis in children.
Methods: A total of four children (two males and two females) were included in this study from January to December 2009. Using a 2-port endoscopic technique, the division of the lower end of the fibrotic SCM muscle was performed through the subfascial working cavern. The subfascial dissection was performed under the fascia of the pectoralis major and above the muscular fibers from ipsilateral axilla with the aid of a homemade dissection balloon.
Results: The mean operating time was 67.5 ± 11.9 minutes (range, 55–80min). There was no serious operative morbidity and the mean follow-up period was 14.8 ± 5.1 months (range, 9–20 months). All patients had complete unrestricted movement of the head and no recurrence was observed during this period.
Conclusion: The transaxillary endoscopic technique, a working cavern created under the fascia of the pectoralis major, offers a safe and straightforward way to surgically manage persistent muscular torticollis while preserving neurovascular structures, exempting extra-dissection of noninvolved tissues and avoiding the potential for poor cosmesis from any neck scar.
Laparoscopic Splenectomy in a Pediatric Reference Center in Peru
Background: Splenectomy in children is indicated mainly for hemolytic diseases. Laparoscopic Splenectomy (LS) is less traumatic and has greater acceptance than the open approach.
Methods: A retrospective analysis of all patients undergoing Splenectomy at our Institution between 2006 and 2010 was performed. Open and laparoscopic splenectomies were done. For LS, we used a 4 port technique in a patient in dorsal decubitus and mild left elevation. Open pneumoperitoneum at 12 or 14 mmHg was installed. Four ports in a “L” layout were put. We started dissection from below to above using ligasure and monopolar coagulation. If there was also indication for cholecystectomy, an additional port was put on the right side for the combined procedure. An endobag is placed and the spleen is removed by the umbilical port previously morcelated. An additional Pfannesteil incision was done for removal of larger spleens.
Results: A total of 32 splenectomies were performed during the period study. Indications were: Hereditary Spherocytosis (20), Portal Hypertension (6), Immune Thrombocytopenic Purpura (5) and Splenic Cyst (1). Twenty LS were performed and 3 required conversion due to non controlled bleeding. Four combined procedures were performed. Average operative time was 118 minutes. In two cases, an additional Pfannesteil incision was made to remove large spleens. Child's acceptance of the procedure was good, and the postoperative evolution was uneventful. Time to initial feeding was 12 hours and patients were discharged at the third postoperative day average. They required use of less analgesia and had excellent esthetic results.
Conclusion: LS has more benefits than open splenectomy in terms of less post operative pain, therefore, less use of analgesia, early initial feedings, early discharge and return to school and plays. Excellent esthetic results are also achieved.
We recommend the use of a 4 port technique in “L” layout, spleen removal through the umbilical port or through an additional Pfannesteil incision for big ones.
Is there a Role For MIS in Pediatric Oncology?
Aim and Objective: To evaluate the role of minimal invasive surgery (MIS) in Pediatric surgical malignancies.
Materials and Methods: A review of patients from 2003 to 2010 in a single institution who underwent minimal invasive surgery (MIS) for Pediatric malignancies. Twenty three children who underwent MIS during this period were identified and followed up. MIS was done for tissue biopsy, resection of residual lesions and also in few children for primary tumor resection. All procedures were done at a single institute.
Results: 23 children underwent a total of 25 MIS procedures. Laparoscopy was performed in 11 patients and thoracoscopy in 12 patients. Of these 6 children underwent primary resection of tumor. MIS was performed for residual lesion in 4 children and in the rest MIS was undertaken for biopsy.
There were 2 conversions, one each in Thoracoscopic and Laparoscopic group. There was no mortality in the series. Adequate tissue diagnosis was obtained in all the patients who underwent MIS for biopsy. Resection of the residual lesion was achieved in 3 children.
Conclusion: MIS is safe and effective in Pediatric surgical malignancies. It provides for near 100% in diagnostic accuracy and in tissue sampling. Is a boon in inaccessible lesions where conventional techniques cannot obtain a biopsy. Has a definitive role in the management of residual lesions. The role of MIS for primary tumor resection remains to be defined.
Minimal Invasive Surgery, The Pharaohs Way
Introduction: The history of minimal invasive surgery started over 5000 years ago.
Aim: To introduce the first minimal invasive surgeon in the history, ANUBIS, The God of the under-world and mummification ANUBIS, was worshipped throughout Egyptian history. He was in the centre of a cult for preserving the human body through the process of mummification, which had mainly advanced in brain evacuation and evisceration. Anubis was originally a god of the underworld and associated with the embalming process and funeral rites. This preservation of the body used a sweet-smelling herbs and plants that would help the deceased. IMHOTEP “Father of Medicine” was worshipped as the god of healing after his death. The main ancient Egyptian medical papyruses are taking into account for these studies. Most of these documents relate to diseases, remedies and the structure of the body as well as incantations and magic spells used as treatments in many cases. The major study of this paper is nasal endoscopy based on transnasal brain removal during embalming by the ancient Egyptians body that started a new medicine era.
A Study Evaluating the Effectiveness of Two-Dimensional and Three-Dimensional Medical Visualization in Anatomy Education
It has been observed that 3D visualization is beneficial to surgical planning and diagnosis as it helps to provide a sense of spatial relation by generating volume representations using the existing 2D medical image data of the patient. A preliminary study with a group of seven subjects identifying anatomical structures with 2D or 3D visualization software suggested that visualization of anatomical features in 3D had value over the traditional images visualized in 2D visualization software. The group was composed of two surgeons that had eight to ten years of experience, and five residents that had one to three years of experience. While the findings suggested at the potential of 3D visualization tools they also hinted at the challenges of moving between a 2D space into a 3D space.
The purpose of this research was to build upon the preliminary results and continue the study with a larger sample size of the same level of experience and knowledge of anatomy. The study aimed to answer the following research question:
What is the impact of 3D visualization over 2D visualization in localization of anatomical features in medical students?
The subjects were randomly divided into two groups: a control group that only used software to interact with the 2D representations using a traditional mouse and keyboard setup and a second group that only used a software to interact with the 3D representations using a gamepad.
The study consisted of four parts:
(1) Pre-test survey—With questions about age, experience with medical 3D visualization tools, computer gaming experience, and gamepad use. These questions were used to examine if correlations existed between previous experience and the study findings.
(2) Software Training—Let the subjects familiarize with the software. Subjects were presented with a quick introduction of the tools and features of the respective software and were allowed five minutes to interact with the software.
(3) Completion of tasks—Subjects were asked to locate three anatomical structures of varying complexities in either 2D or 3D, the Gallbladder, Celiac Trunk, and the Superior Mesenteric Artery (SMA). Subjects were encouraged to think out loud as they performed the tasks, and comments were recorded by an observer. The time taken for the tasks was also recorded as a metric of measurement for this study. Another measurement metric would be the accuracy of the locations identified by the subjects.
(4) Post-test survey’ Questions and feedback on the software in terms of usability and user experience that could lead to future research questions.
The Impact of the Alexander Technique in Improving Surgical Ergonomics and Posture During Minimally Invasive Surgery (MIS)
Introduction: One of the main ergonomic challenges during surgical procedures is the surgeon's posture. Under ideal circumstances during surgery the surgeon's posture would be completely static; such non-movement is not only impossible to maintain but is also impractical, this issue is further compounded during the performance of minimally invasive surgery (MIS) where the surgeon sometimes assumes an awkward posture. There have been numerous reports of work related injuries in laparoscopic surgeons. The Alexander technique (AT) involves the psychophysical re-education of one's body in order to improve postural balance and co-ordination, permitting movement with minimal strain and maximum ease. The purpose of this study is to evaluate the efficacy of the AT in improving posture and surgical ergonomics during the performance of MIS.
Methods: We performed a prospective cohort study in which each subject served as their own control, with IRB approval a total of seven test subjects were recruited from the Urology training program. The subjects underwent a preAT assessment of postural coordination by the American Society for the Alexander Technique instructors, and a preAT assessment of basic laparoscopic skills (FLS). All subjects were instructed on using the AT. The subjects then underwent a postAT assessment of postural coordination and FLS. Additionally each subject was asked to complete a questionnaire on perceived effort before and after the AT education. The preAT and postAT subjective and objective data was tabulated and analyzed with the paired two-tail ‘t’ test for statistical significance.
Results: All seven subjects completed the entire study. Each of the subjects demonstrated improved ergonomics and an improved ability to complete the FLS, there was a statistically significant difference in 3 of the four FLS modules tested. There was subjective improvement in the subject's posture. The time load test–a test of postural endurance demonstrated a statistically significant improvement postAT (p = 0.042). Overall there was significant improvement in the subjects' posture, both at rest and during MIS tasks.
Conclusion: The AT training program resulted in a significant improvement in posture, endurance, and proficiency, accompanied by a reduction in subjective/perceived discomfort during MIS tasks. This is the first report of the AT in improving surgical ergonomics. Improved surgical ergonomics, endurance and posture reduces the occurrence of surgical fatigue. Intra-operative fatigue has a high correlation with surgical errors. An additional benefit of AT training might be a reduction in the incidence of repetitive stress injuries to the laparoscopic surgeons, this is especially important as MIS is evolving further with the implementation of Laparo-Endoscopic Single Site (LESS) surgery, which would appear to be more strenuous on the surgeons who perform these procedures. Further studies investigating the influence of AT on surgical posture, MIS ergonomics and open surgical techniques are warranted.
Laparoscopy and Postoperative Early and Late Ultrasound Follow-Up Results of Ovarian Cysts in Children
Aim: As a non-invasive procedure, ultrasound (USG) has a crucial role in diagnosis and follow-up of ovarian cysts in children. There is no consensus on postoperative follow-up protocol of patients who have been operated for ovarian cyst. In this prospective study, we made postoperative USG with regular intervals to evaluate the postoperative early and late condition of the ovaries following the laparoscopic intervention.
Methods: 40 patients who have been operated by laparoscopy for ovarian cysts between 2005–2010 were included into the study. Preoperative and operative findings and postoperative USG follow-up results were evaluated in this study. The patients had USG on postoperative 1st, 3rd, 9th and 12th months.
Results: A total of 45 ovarian and paraovarian cystic lesions treated by laparoscopy for cystic disease of ovaries. The ages of the patients were between 13/365 days to 18 years. A recurrence was not detected in early and late USG controls on the side which was operated. Only significant finding in our study was to development of the contralateral cyst formation in the late (after 12th months) USG of 5 patients. All of these 5 patients had a second laparoscopic exploration and cyst excision for the contalateral side.
Conclusion: Laparoscopy is an effective treatment modality in children with ovarian cysts. A long-term follow-up of both ovaries by USG and clinical findings provide an early diagnosis of recurrent cysts that may need a second laparoscopic exploration.
Laparoscopy for Ovarian Lesions in Children
Aim: Laparoscopy is a well established diagnostic and therapeutic modality in paediatric surgery. We report our experience in laparoscopic management of ovarian lesions in children.
Methods: Retrospective review of clinical records of patients with ovarian pathology, who were managed with laparoscopy or a lap-assisted procedure.
Results: Over the past five years, fifty two children with an ovarian lesion(s) were operated at our centre with the aid of laparoscopy. The median age of the children at presentation was 13 yrs (range,5 days to 16 years). Most of children had unilateral lesions except two. The main presenting symptom was abdominal pain in 34 cases (65%). Fifteen patients (29%) were noted to have an abdominal mass and 3 (6%) were incidentally diagnosed to have an ovarian lesion. Ovarian cyst with torsion was found in 22 cases (42%). Nine children (17%) were <3 months old. These were antenatally diagnosed as abdominal cysts and found to have an autoamputated ovary on exploration. Of the 52 cases in total, successful cystectomy with ovarian preservation was accomplished in 38 (73%) cases and salpingo-oophorectomy was performed in 14 cases (27%). Conversion to open surgery was required in 2 cases (4%). There were 40 simple cysts (follicular/leuteal/serous) (77%) and 10 mature cystic teratomas or dermoid cysts (21%). One patient (2%) had an immature teratoma. Median operative time was 105 mins (range, 45 to 300 mins). There were no operative or post-operative complications recorded. The median duration of hospital stay was 3 days (range, 1 to 6 days). The patients were followed up 3–6 monthly with clinical and ultrasound assessment. Of the 38 patients who underwent cystectomy with ovarian preservation, 35 (92%) patients showed normal recovery of the involved ovary.
Conclusions: Laparoscopy is safe and effective method of managing ovarian lesions in infants and children.
Reoperative Minimally Invasive Surgery in Infants and Children
Background: Laparoscopic surgery in infants and children has become the standard approach in many pediatric surgical practices. Patients with no prior abdominal surgeries rarely present a contraindication to performing laparoscopic surgery for a variety of problems. Many surgeons eliminate the possiblity of laparoscopic surgery in patients with complex abdominal wall defect repairs and prior abdominal surgeries-especially those having multiple prior surgeries. An aggressive approach to applying laparoscopic surgery to patients with previous abdominal surgeries and following closure of abdominal wall defects has broadened the number of patients undergoing laparoscopic surgery and has allowed these patients to experience the benefits of laparoscopic surgery such as less pain and shorter recovery time for those subsequent operations that were appropriate for laparoscopic approaches.
Purpose: The purpose of this study is to evaluate this institutuion's experience with reoperative laparoscopic surgery.
Methods: Charts were reviewed for all patients undergoing reoperative laparoscopic surgery at our institution from August 2007 to September 2010. Reoperative surgery is defined as a repeat laparoscopic surgery or a laparoscopic procedure following an open operation.
Results: Sixteen patients were identified as undergoing laparoscopic surgery after previous abdominal surgery. The previous surgeries were: laparoscopic gastric or appendix procedures-3, open operations on target organ-3, open operation on entire peritoneum-1, colostomy-3, VP shunt-3, and omphalocele repair-3 (2 primary, 1 biologic prosthesis). The laparoscopic procedures performed in these patients were: lap GT-5, lap-assisted VP shunt-3, lap pull-through for imperforate anus-3, lap colectomy-1, lap sigmoidostomy tube-1, lap Nissen-2, lap appy-1. Fifteen patients successfully underwent laparoscopic procedures. One redo Nissen was converted to open due to extensive scarring.
Conclusion: Reoperative laparoscopic surgery is successful the majority of the time and should be considered when appropriate regardless of the type of prior abdominal surgery.
NOTES (Natural Orifice Transluminal Endoscopic Surgery)
Laparoscopic Gastric Pull-Up by Using the Natural Orifice Translumenal Surgery (NOTES) Technique: A Novel Procedure for Treating Long-Gap Esophageal Atresia (Type A)
Aim: The aim of this study is to develop a novel procedure for treating long-gap pure esophageal atresia. This procedure, which entails the combined use of laparoscopy and natural orifice translumenal surgery (NOTES), enables primary repair without cervical and thoracic incisions and prevents the possibility of postoperative gastroesophageal reflux disease.
Methods: The procedure employed in the feasibility study, which is being conducted using pigs, is as follows. First, a laparoscopic operation, which includes fundoplication, complete mobilization of the stomach, and enlargement of the esophageal hiatus, is performed. Subsequently, NOTES is performed—a small hole is created by electrocautery in the upper esophagus and dilated using a balloon dilator. A flexible endoscope is then inserted into the upper mediastinum via the esophagus, and dissection of the posterior mediastinum up to the abdominal cavity is performed by blunt dissection and air insufflation. Thereafter, gastric pull-up is performed using both laparoscopy and NOTES. Finally, an esophagoesophageal anastomosis is performed.
Results: To date, we have performed this procedure on 5 pigs. First, the abdominal esophagus was incised at the level of the hiatus, since this procedure was developed for treating patients with esophageal atresia. The stomach was released enough to reach the upper mediastinum, and Nissen fundoplication and enlargement of the hiatus by dissecting both the crura were performed. Subsequently, a flexible endoscope was inserted into the upper mediastinum through the entry point at the upper esophagus. Postmediastinum tunnel from the entry point to the abdominal cavity was easily created using air insufflation and blunt dissection that was performed by advancing an endoscope through the mediastinum, and the tunnel was dilated using a balloon dilator. Strings sutured at the stump of the abdominal esophagus were grasped and pulled using the NOTES approach, and the stomach was laparoscopically pushed into the tunnel. However, the gastric pull-up could not be completed. Postmortem investigation revealed that the mediastinum of the pig was too small to contain the stomach. Therefore, we established transesophageal access to the abdominal cavity via the right thorax, and succeeded in pulling the stomach up to the upper mediastinum. The operation time until gastric pull-up was 3 hours and 50 minutes.
Conclusions: Laparoscopic gastric pull-up without cervical and thoracic incision is feasible. The procedure, which is performed concomitantly with fundoplication, can decrease the incidence of gastroesophageal reflux disease. Although gastric pull-up via the posterior mediastinum could not be done in this pig model, it is possible for patients with esophageal atresia. Intraoperative findings and the challenges for clinical application can be presented.
Single-Incision Laparoscopic Surgery
Single-Port Laparoscopic Varicocelectomy Induces Minimal Post-Operative Stress Response in Children
Purpose: Single incision laparoscopic surgery has recently been described in children and regarded as an improved technology leading to less pain and better cosmetic outcome. Compared with the traditional three-port method, it is not known if the single-port method is less invasive. The aim of this study was thus to investigate the post-operative acute inflammatory response in order to evaluate surgical stress in the two approaches in children.
Methods: A prospective, single blinded, case control study was carried out. Fourteen male patients who presented with unilateral varicocele were divided into two groups. Seven children underwent single-port laparoscopic procedure while the other seven children underwent three-port laparoscopic procedure. Pre-operative and post-operative blood samples were taken for the measurement of tumor necrosis factor-α (TNF-α) and interleukin 6 (IL-6) using ELISA. Demographics including the operation time, and complications were recorded. Data were analyzed using unpaired t-test and a p value of <0.05 was taken as statistically significant.
Results: The mean age of our patients was 14.5 years (range, 12–19 years). There was no significant difference between the two groups in terms of operative time, nor was there any complication recorded. The change in serum TNF-α concentration between pre- and post-operatively was 0.324 ± 0.406 pg/ml in the single-port group and 0.329 ± 0.952 pg/ml in the three-port group (p = 0.990). For serum IL-6, the change in pre-operative and post-operative levels was 0.151 ± 0.392 pg/ml and 0.097 ± 0.929 pg/ml (p = 0.899) for the single-port group and three-port group respectively.
Conclusions: Single-port laparoscopic varicocelectomy is safe, effective and produces better cosmesis and minimal surgical stress.
Sutureless Closure of Umbilical Port Site After Single Port Laparoscopic Appendectomy (SPLA) Using N-Butyl Cyanoacrylate Glue
Background: Application of glue to the wound has several benefits. Glue is haemostatic, waterproof, leaves no suture marks, allows examination of the wound possible and allows the child to have a bath/shower the very next day of surgery. Also no wound care or dressing changes are required.
Purpose: The aim of this study is to retrospectively review our experience using tissue glue for umbilical port site closure after SPLA in children.
Methods: Over a period of 1.5 years, 57 children underwent single port laparoscopic appendectomy (SPLA) by a single surgeon at our institution. M: F ratio was 33:24. Median age was 10.8 years (Range 4–17). 11 children (19%) had perforated (advanced) appendicitis and 46 children (81%) had early appendicitis.
Technique: After withdrawal of the umbilical port, the fascia was closed with ‘0’ vicryl sutures. The wound was then irrigated with saline and dried. The skin incision was then approximated with glue in all cases.
All patients were followed in our clinic 3–4 weeks post surgery.
Photographic and patient/parent satisfaction documentation was obtained during their office visit in all cases. Local complication including wound dehiscence, infection and persistent leakage from the wound site, pain or allergic reaction to the chemical were all recorded.
Results: One child with perforated appendicitis developed signs of wound infection and was treated with antibiotics for 5 days successfully. None had any wound dehiscence or local skin reaction/allergy to cyanoacrylate. Scars healed well in all cases and no umbilical scars were visible at follow-up. Both the parent and the patient were extremely satisfied with the excellent cosmetic results.
Conclusion: Sutureless closure of port sites after single port surgery with glue is a safe and effective method for wound closure with excellent cosmetic results, low infection rate and almost no local wound complication.
Comparison of Outcomes Between Single Incision Laparoscopic Appendectomy and Conventional Laparoscopic Appendectomy in Children
Background and Aim: Single incision laparoscopic appendectomy is a more cosmetic technique. However, it remains unknown whether single incision laparoscopic appendectomy has advantages other than cosmesis compared to conventional laparoscopic appendectomy. We retrospectively evaluated outcomes between single insicion and conventional laparoscopic appendectomy for uncomplicated appendicitis in children.
Patients and Methods: Between April 2009 and September 2010, 33 patients underwent laparoscopic appendectomy for acute phlegmonous appendicitis. Twenty-two patients (13 boys, 9 girls) underwent conventional laparoscopic appendectomy (CLA) and eleven patients (8 boys, 3 girls) underwent single incision laparoscopic appendectomy (SLA). Patients with perforated appendicitis or abscess were excluded. Mean patient age was 10.7 years (6 to 15) in CLA, and 9.9 years (4 to 14). We evaluated the surgical duration, length of hospital stay, frequency of postoperative analgesic requirement, duration of postoperative pain, and incidence of complications. We measured the surgical duration in patients managed by a single surgeon (12 in CLA, 11 in SLA). The duration of postoperative pain was evaluated by VRS (Verbal Rating Scale).
Surgical technique: All patients were placed in a supine position. In the CLA group, the first 12 mm trocar was inserted at the umbilicus, using the open Hasson technique. After pneumoperitoneum of 10 mmHg had been obtained, a 5 mm trocar was placed outside the right rectus muscle at about the level of the umbilicus, and another 5 mm trocar in the middle of the lower abdomen. In the SLA group, an intra-umbilical circum incision was made, and a small skin flap was raised to expose the abdominal wall fascia. The first 5 mm trocar was inserted using the open Hasson technique. After pneumoperitoneum, another 5 mm trocar and a 3.5 mm trocar were placed with a triangular orientation at the umbilicus. In both groups, the mesoappendix was dissected using laparoscopic coagulating shears, and the appendix was ligated at the base by two endoloops. Finally, the appendix was removed using a plastic bag.
Results: The surgical duration was 38.7 ± 5.8 minutes for CLA, 53.9 ± 6.7 minutes for SLA. Mean surgical duration was significantly shorter in CLA (p < 0.001). Length of hospital stay was 3.64 ± 0.83days for CLA, 4 ± 0.74 days for SLA. Frequency of postoperative analgesic requirement was 2.32 ± 1.67 times for CLA, 2.0 ± 1.04 for SLA. Duration of postoperative pain was 52.27 ± 19.18 hours for CLA, 54.45 ± 18.59 hours for SLA. These outcomes were similar for both groups. Only one complication, wound infection, was observed in the CLA group.
Conclusions: The prolonged surgical duration in SLA may depend on the learning curve of the surgeon. SLA was not inferior to CLA in length of hospital stay, frequency of postoperative analgesic requirement, duration of postoperative pain, or incidence of complications. Our study suggests that SLA is a feasible technique for uncomplicated appendicitis in children.
The Cross-Technique for Single-Incision Pediatric Endosurgical (SIPES) Pyloromyotomy
Background: Single-incision pediatric endosurgical (SIPES) pyloromyotomy is frequently used for the treatment of hypertrophic pyloric stenosis at our center. Our initial SIPES approach mirrored the conventional, triangulated laparoscopic pyloromyotomy. However, an increased number of perforations were noted on our initial analysis. Thus, a simpler, more straightforward Cross-technique for SIPES pyloromyotomy was developed.
Objective: This study compares the current Cross-technique SIPES pyloromyotomy to the previous standard SIPES operation in terms of efficacy and complication rate.
Methods: The Cross-technique entails grasping the antrum with the surgeon's left hand instrument, retracting towards the left lower quadrant, and thereby orienting the pylorus obliquely towards the right upper quadrant (Fig. 1). The serosal incision and muscular spreading is accomplished using a right-hand instrument that crosses over the left hand grasper. Demographic variables, operative times, estimated blood loss (EBL), complications, conversion rate, and postoperative length of stay were compared statistically.
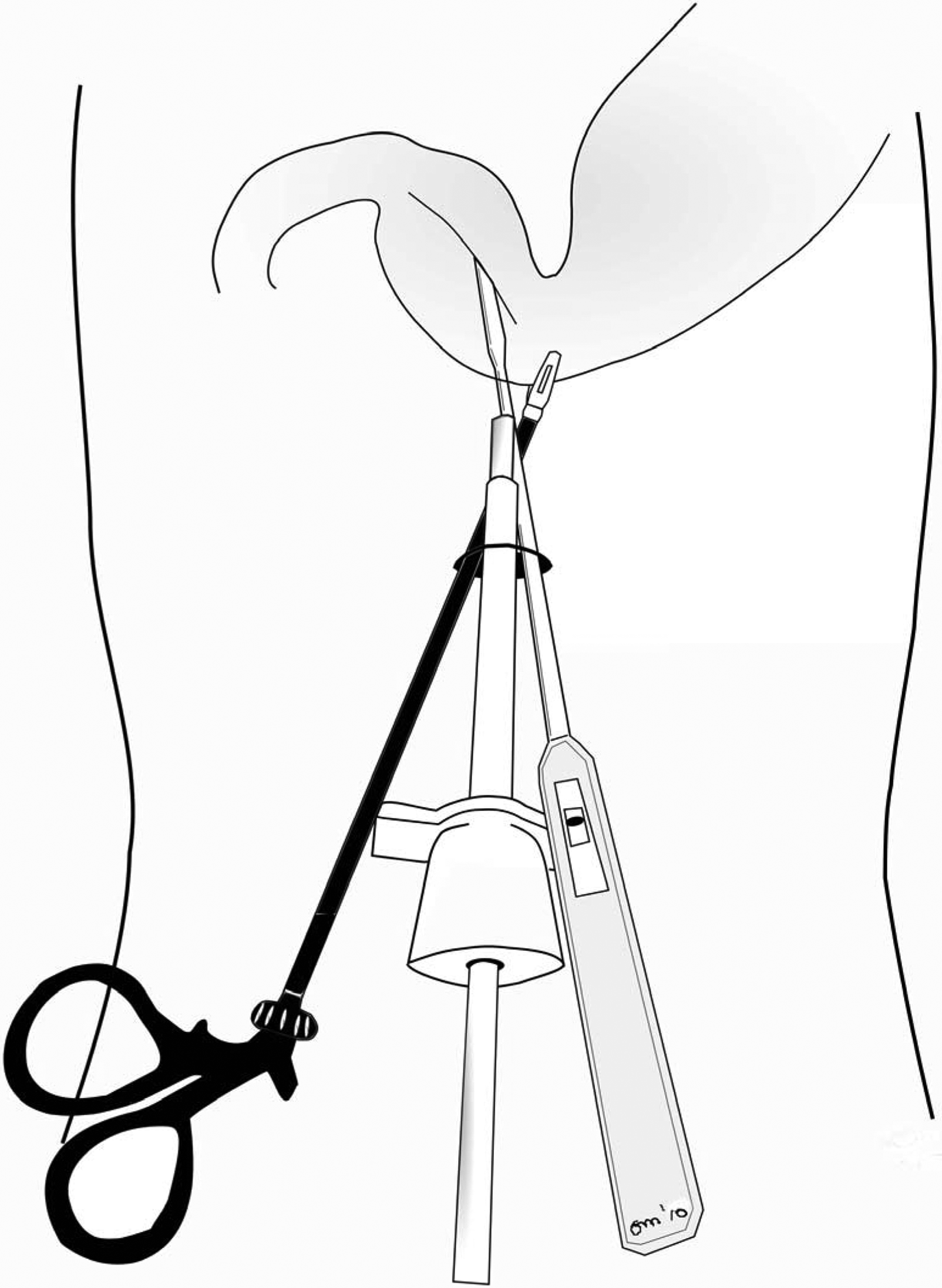
Diagram of the principle of Cross-technique SIPES pyloromyotomy.
Results: A total of 29 Cross-technique patients were compared to 23 in the standard group. The Cross-technique was faster than the standard procedure (21 ± 5 versus 27 ± 12 minutes, p = 0.030) and EBL was lower (1.3 ± 0.5 versus 1.7 ± 0.6, p = 0.015). There were two mucosal perforations and conversions to triangulated 3-access-site laparoscopy in the standard, but none in the Cross-technique group (p = 0.191). Patients who underwent cross-technique pyloromyotomy weighed slightly less (3.6 ± 0.6 versus 4.0 ± 0.5 kg, p = 0.012), but there was otherwise no statistical difference in age, gender ratio, conversion rate or length of stay between the groups. There was one postoperative wound infection in the cross-technique group, but none in the standard group. None of the patients required reoperation. All participating surgeons felt that the cross-technique was more ergonomic and easier to perform than the standard SIPES technique.
Conclusions: The Cross-technique appears superior to standard SIPES pyloromyotomy and should be preferentially used for single-incision endosurgical pyloromyotomy for hypertrophic pyloric stenosis.
Background: Laparoendoscopic single site appendectomy (LESS) is now being used at many centers for the management of acute appendicitis. Younger the child more is the technical challenge for laparoscopic surgery. The parallel alignment of the laparoscopic instruments and its close configuration along with the restricted workspace in smaller children creates an unique challenge for minimally invasive surgeons. Question is whether it is possible to do Laparoendoscopic single site appendectomy (LESS) in children less than 8 years?
We looked at our experience so far with LESS in children less than 8 years.
Methods: We retrospectively reviewed records of children who underwent LESS for acute appendicitis at our institution. Period of the study was from March 2009 to August 2010. All patients were followed 3–4 weeks post surgery in the clinic. The variables analyzed were gender, age, operative time, complications, length of stay and cosmetic results.
Results: A total of 57 LESS appendectomies for acute appendicitis were performed between May 2009 and August 2010. There were 10 (14%) children with acute appendicitis who were less than 8 years old. The average operative time for LESS appendectomy in young children was 49.75 minutes (Range 42–66 minutes). 4 (40%) children had a perforated appendicitis while 6 (60%) had non-perforated or early appendicitis. The length of stays varied from 1 to 6 days. The average of length of stay was one day for non-perforated appendicitis versus 4 days for patients with perforated appendicitis. No cases were converted to open surgery or conventional laparoscopic surgery. There were no complications. Patients and parents were extremely satisfied with the cosmetic results.
Conclusion: Our limited data suggest that LESS appendectomy is a safe and acceptable approach for children less than 8 years. This procedure can be performed in comparable operative time with good outcomes and excellent cosmetic results.
Substitution of Conventional Laparoscopic Surgery with Single-Incision Laparoscopic Surgery for Performing Appendectomy: A Single Institution Review
Background: Recent reports suggest that single-incision laparoscopic surgery (SILS) is technically feasible. Acute appendicitis is one of the most common surgical problems in clinical practice. The popularity of SILS has recently increased, and several techniques for single-incision laparoscopic appendectomy (SILA) have been described. We describe our initial experiences of performing SILS for appendicitis by using conventional instruments and also the methodological changes in laparoscopic appendectomy (LA) in the single institution.
Patients and Methods: This review included all patients with appendicitis who were treated laparoscopically in our institution between January 2008 and September 2010. The preoperative, intraoperative, and postoperative data were collected and reviewed retrospectively.
Results: A total of 144 patients were reviewed. Among these, 65 patients underwent the conventional technique of three-port laparoscopic appendectomy by using pre-tied knot suture (LAPA-P) (range, 2–15 years old; median, 11 years old), 75 patients underwent laparoscopic appendectomy by using extracorporeal knotting (LAPA-E) to reduce costs (range, 3–15 years old; median, 10 years old), and 4 recently admitted patients underwent SILA (age, 6–14 years old; median, 10 years old). SILA was completed intracorporeally by using conventional instruments—one 3-mm and two 5-mm ports. Complicated appendicitis with or without perforation was noted in 47 (33%) patients. The mean operative times in patients, excluding those with complicated appendicitis, who underwent LAPA-P, LAPA-E, and SILA were 51.7 min (range, 35–80 min), 54.1 min (range, 30–80 min), and 68.7 min (range, 55–80 min), respectively. None of the cases were converted to open appendectomy. There was no significant difference in the complication rates and the incidences of each complication between the 3 procedures.
Conclusion: The substitution of the conventional approaches with SILS for performing acute appendicitis was successfully achieved. The duration of SILA was slightly longer than that of conventional LA, but this can be reduced with experience. Larger studies and further technical refinements are required, but SILA using conventional, rather than special, instruments can be feasible and be acceptable to pediatric endoscopic surgeons.
Single Incision Laparoscopic Surgery (SILS) for Adnexal Pathology in Adolescent Girls
Introduction: Single incision laparoscopic surgery (SILS) is a comparatively new technique and its validity and advantages in pediatric surgical practice is still the topic for discussion. The aim of our study was to analyze our initial experience with SILS in adolescent girls with adnexal pathology.
Materials and Methods: The total number of 35 SILS operations were performed during the last two years (2009–2010). There were 2 cholecystectomies; 2 splenectomies; 2 nephrectomies. 29 SILS procedures were performed for ovarian and paraovarian lesions in adolescent patients aged from 12 to 17 years: teratomas (14), cystadenomas (5), paraovarian cysts (8), androgen-producting tumours–suspected androblastomas (2). The size of the mass varied from 6 to 20 cm in diameter. In 4 cases urgent SILS procedures were performed for adnexal torsion and “acute abdomen” syndrome.
Single umbilical SILS port with three trocars, raticulating and ordinary laparoscopic instruments were used in all cases. “Ligasure,” “Harmonic” devices, entrapment endobags including large “Endocatch II” could be used through the SILS port when it was necessary.
The character of the principal procedure was–adnexectomy (4), ovariectomy (2), ovary sparing cyst enucleation (23).
Results: There were no conversions to multi-port laparoscopy or open surgery. Mean operative time was about 55 minutes (from 35 to 130 min.).
No intraoperative and postoperative complications occurred. Cosmetic results were good in all cases.
Laparoscopic examination revealed concomitant surgical pathology in 14 patients and SILS technology made it possible to perform simultaneous procedures in these cases–patent processus vaginalis closure (5); benign adnexal lesions that were not diagnosed preoperatively (12–small teratomas, paraovarian cysts, hydatids of Morgagni); omentum and contralateral ovary biopsies (2 patients with suspected androblastomas); appendectomy (2).
Conclusion: Single incision laparoscopic surgeries are feasible in pediatric patients with gynecological pathology, including emergency situations; SILS technology allows performing all necessary surgical manipulations including ovary sparing procedures, various simultaneous surgical manipulations for diagnosed concomitant pathology.
In our opinion, large adnexal masses in adolescent girls is the best indication for SILS technologies in pediatrics; and it is the only group of pediatric patients where SILS can be real alternative to conventional multipuncture microlaparoscopic surgery;
Greater numbers of cases and a comparative study is necessary to assess the true benefit of this technology (if there is any).
Experience with Modified Transumbilical Laparoscopic Surgery in Children
Background: Single incision transumbilical laparoscopic surgery requires one multi-channel trocar and special roticulating instruments. The disadvantages of this technique are large umbilical incision, more postoperative pain, a higher risk for developing hernias or surgical site infections. The modification of this method may be utilizing two or three small incisions for multiply trocar placement in umbilical area. We present our initial experience with multi-trocar transumbilical laparoscopic surgery in children.
Methods: A retrospective review of all the patients that underwent multi-trocar transumbilical laparoscopic surgery was conducted between January 2009 and September 2010. All procedures were performed with the same technique. An infra-umbilical 10 mm skin incision is made before Veres needle insertion. After insufflation, 10 mm trocar and endoscope with 6 mm working channel is placed. Once laparoscopy is performed one or two additional 3 mm or 5 mm trocars are inserted through small incisions around umbilical ring without connection of fascia incisions. This technique permits the use of two or three instruments in the abdominal cavity without opening the fascia over a long segment.
Results: There were 122 operative procedures: 108 appendectomies, 8 cholecystectomies, 3 inguinal herniorrhaphies and 3 ovarian cyst excisions. Aged ranged between 9 months and 16 years. Mean operative time for appendectomies was 30 minutes, 35 minutes for cholecystectomies, 30 minutes for herniorrhaphies and 35 minutes for cyst excisions. There were no intra-operative complications. There were two conversions to conventional laparoscopic surgery in the cases of diffuse peritonitis. No post-operative complications were seen.
Conclusions: Multi-trocar transumbilical laparoscopic surgery appears to be feasible, safe and effective. This technique is performed in a comparable operative time with good outcomes and great cosmetic result. Such approach may be alternative to single incision multi-channel trocar surgery particularly in infants and small children.
Laparoscopic Single Port Cholecystectomy in Children: A Single Centre Experience
Background: Laparoscopy is the standard approach for cholecystectomy in most paediatric surgical centers. In an attempt to minimize the surgical trauma and improve cosmetic outcome new laparoscopic techniques with a single incision through the umbilicus has been proposed.
We evaluated the feasibility of laparoscopic single port cholecystectomy in children and present our first consecutive seven cases.
Material and Methods: Seven patients were operated with single port laparoscopic cholecystectomy 2009–2010 (three girls, four boys, age 5–14yrs, bodyweight 15–52 kg). The first two patients were operated with SILS®-port (Covidien) and a combination of roticulating instruments (Covidien) and conventional 5 mm laparoscopic straight instruments. Five patients were operated with TriPort® (Olympus) and similar instrumentation. A 5 mm 30° telescope (EndoEye®, Olympus) was used. Retraction of the gall bladder and liver was achieved with a monofilament stay suture passed through the abdominal wall below the right costal margin and through the fundus of the gall bladder. Dissection of the gallbladder, the cystic duct and the cystic artery was performed according to standards for laparoscopic cholecystectomy, including intraoperative flouroscopic cholangiogram.
Results: No surgical complication was registered. One operation was “converted” with one extra 5 mm port to allow better retraction of the gall bladder and liver. Operation time was longer for Single Port Laparoscopic cholecystectomy compared to conventional laparoscopic cholecystectomy, with a tendency towards shorter operating time already after a few operations. Postoperative pain and time to discharge was comparable to conventional laparoscopy. At follow-up no incision hernia was registered, and the cosmetic result was very good. The adoption to using crossing, roticulating instruments was swift. The TriPort required a smaller umbilical incision compared to the SILS-port, making it better adopted to paediatric surgery.
Discussion: Laparoscopic single port surgery is quickly spreading in general- and paediatric surgery. New instruments and ports are rapidly being introduced, making it possible to apply single port surgery also in paediatric surgery. Potential benefits except for cosmetic outcome are reduced postoperative pain, shorter hospital stay and faster return to normal physical activity. Our initial experience show that single port laparoscopic surgery in paediatric population is feasible, effective and safe.
Single Port Access (SPA) Laparoscopic Intracorporeal Appendectomy Using Conventional Laparoscopic Surgery Instruments
Background: Single port access surgery for appendectomy is now a popular choice at many institutions. The instrument clatter with the parallel placement of instruments and with the loss of triangulation during conventional laparoscopy makes it technically challenging. Various new roticulating instruments as well as telescopes have been devised to circumvent this problem. Addition of these instruments ends up increasing the cost per procedure substantially.
We report our experience with the use of conventional of laparoscopic surgery instruments for single port access intracorporeal appendectomy in children.
Methods: We retrospectively reviewed the charts of all children undergoing laparoscopic single port access appendectomy at our institute. A total of 57 SPA appendectomies were performed over a period of 1.5 years. The last 21 cases were performed using conventional instruments. Charts were reviewed for age, gender, complications, hospital stay, operative time, follow-up visit, cosmetic appearance of the scars. All patients had follow-up visit at 3–4 weeks post surgery in the clinic.
Technique: Vertical Incision was made in the scar of the umbilicus and using the modified Hassons technique an Olympus Triport was placed in to the peritoneal cavity. A conventional 5 mm 30 deg of standard length was then introduced. Using the conventional straight laparoscopic instruments the appendix was dissected and then resected using endoloopes. It was then retrieved through the cap of the Triport.
Results: A total of 57 SPA laparoscopic appendectomies for acute appendicitis were performed between May 2009 and August 2010. The last 21 cases were performed using conventional instruments. The average operative time for SPA laparoscopic appendectomy was 49.75 minutes (Range 42–66 minutes). The length of stays varied from 1 to 6 days. The average of length of stay was one day for non-perforated appendicitis versus 4 days for patients with perforated appendicitis. No cases were converted to open surgery or conventional laparoscopic surgery. There were no complications. Patients and parents were extremely satisfied with the cosmetic results.
Conclusion: SPA laparoscopic appendectomy using conventional laparoscopic instruments is safe and acceptable technique. With our technique it is not necessary to buy the expensive reticulating instruments and thus save money for the hospital and the patients.
What is the Learning Curve with Single Incision Laparoscopic Cholecystectomies in the Pediatric Population?
Objective: The laparoscopic method has become the standard of care and preferred technique in both the adult and pediatric population for cholecystectomy. With the introduction of Single Incision Laparoscopic Surgery (SILS), the questions have been asked, is there a learning curve for this procedure and how steep is it? Based on our experience at a regional pediatric referral hospital we plan on identifying whether there is a number of cases at which the operative time for a SILS cholecystectomy plateaus and then look at how this compares to standard laparoscopic cholecystectomy (LC).
Methods: We conducted a retrospective review of all the cholecystectomies (SILS and laparoscopic) performed at our institution by two pediatric surgeons for the period of July 2009 to March 2010 (n = 86; LC = 47, SILS = 39). We then compared operative times for the procedures looking specifically at trends for the SILS group until the times reached a steady state.
Results: Operative times were found to be mean of 60.4 minutes for LC and 62.7 minutes for SILS (p < 0.05). We also found that the learning curve for SILS procedures to come to a plateau operative time was about 12 cases or 30% of the SILS population.
Conclusions: There was no significant difference between LC and SILS in our patient population in terms of operative time. This is true, after the first 12 SILS cases because there was a statistically significant difference noted between the initial 12 cases and the subsequent 27 SILS cases performed. We feel that although this is a good starting point, a larger trial with multiple surgeons should be performed to identify how steep the learning curve is for SILS cholecystectomy.
Analgesic Requirement After Conventional Laparoscopic Versus Sils Appendectomy in Children
Objective: Single incision laparoscopic surgery (SILS) has become a standard procedure for appendectomy in children. The technique allows a virtually unscarred operation by insertion of a triple-port via a single umbilical mini-laparotomy. However, only little is known about the impact of the approach on postoperative pain. We therefore evaluated the requirement of analgesic medication after conventional laparoscopic (CL) versus SILS appendectomy in children.
Methods: A retrospective chart review was performed between January and September 2010 to collect data for children older than 4 years suffering from an acute uncomplicated appendicitis on: age and BMI at surgery, operation time, duration of hospitalization and the total amount of analgesics peri- and postoperatively, defined as quantity times applied dosage per kg body weight (mg/kg BW). Pain treatment consists of intravenous or oral administration of paracetamol or metamizole (about 15 mg/kg body weight each) regularly or on inquiry of the patient, depending on the individual postoperative course. Data are presented in mean ± standard deviation tested at a significance level of p < 0.05.
Results: 67 patients (30 female) at a mean age of 11.1 ± 3.5 years and a mean BMI of 18.8 ± 3.8 kg/m2 underwent either SILS (n = 7) or CL (n = 60) appendectomy. Mean operation time was 57.1 ± 16.6 min for SILS versus 67.2 ± 28.4 min for CL, mean hospitalization was 4.0 ± 1.4 days (SILS) versus 3.9 ± 1.5 days (CL), both not significant different. The total amount of required analgesics was similar for both groups, 96.3 ± 101.4 mg/kg BW after SILS and 111.4 ± 83.9 mg/kg BW after CL appendectomy. The total amount of required analgesics significantly correlated with the duration of surgery (p < 0.0001, R = 0.48) for all patients.
Conclusion: Postoperative analgesic requirement was significantly correlated with the operation time but remained unaltered by the performed laparoscopic technique, suggesting a comparable well-being and appropriate postoperative course in children after SILS appendectomy.
Early Experience with Single-Incision Laparoscopic Surgery (SILS) for the Placement of Laparoscopic Gastrostomy in a 10-Year-Old Girl
Access procedures for alimentation have been performed both endoscopically and surgically. In patients in whom endoscopic gastrostomy feeding tubes can not be placed, SILS gastrostomy is an alternative approach. This minimally invasive approach is a new technique through a single umbilical incision, without the need for additional laparoscopic ports.
In this article we present our first experience with SILS by placing a gastrostomy in a 10-year-old girl who was not candidate for PEG-tube due to varices in the oesophagus and hepatosplenomegaly. She had an advanced stage of mucoviscidosis with livercirrhosis. She also had an umbilical hernia which we would repair during the same procedure through the same incision. Access and pneumoperitoneum were obtained through the umbilicus with the SILS port. The selected place for the feeding tube in the stomach was exteriorized through this incision and the feeding tube was placed. The stomach was returned into the abdomen. The fascial defect, and thus also the hernia, was repaired and the 2-cm umbilical incision was closed with endocutaneous sutures. The operation time was 25 minutes. Intraoperative and postoperative course was uneventfull. We were able to use the feeding tube on the first postoperative day with good bowel function. The patient and her parents were very pleased with the cosmetic outcome.
SILS procedure seems to be a less invasive alternative to open placement of gastrostomy. This approach has the possible advantages of reduced postoperative pain, faster return to normal function, reduced port site complication, improved cosmesis (a virtually invisible scar in the umbilicus) and better patient satisfaction.
Single-Port Appendectomy in Paediatric Surgery: A Retrospective Single Centre Study
Introduction: The advantage of laparoscopic appendectomy which has been used since 1980 has always been controversially discussed. Since then, laparoscopic appendectomy has been refined in order to increase the benefits. In 1992 Pelosis proposed the single-port appendectomy. The aim of the present article is to report our technique and results of single-port appendectomy in children.
Materials and Methods: This is a single centre retrospective study from the Children's hospital of Cologne. Between November 2005 and January 2010 we performed 242 single-port appendectomies. Single-port appendectomy was performed in all patients presenting with a preoperative diagnosis of acute appendicitis or in rare cases of recurrent pain in the right lower quadrant. Patients with preoperative diagnosis of perityphlitic abscess were treated conservatively or operated with an open technique. Operative technique: The access to the peritoneal cavity is performed through a semicircular umbilical laparotomy. A 10 mm trocar is inserted. After establishing a pneumoperitoneum, a 10 mm zero degree operating laparoscope is introduced. A 5 mm Babcock clamp is introduced through the working channel of the laparoscope and is used to localize and mobilize the appendix. The tip of the appendix is grasped. Insufflation is stopped and the appendix is externalized through the umbilicus while removing the trocar. The appendectomy is performed in a standard technique with two ligatures at the basis.
Results: We performed single-port appendectomy in 242 patients. The mean age at operation time was 10 years. All patients received preoperative antibiotic prophylaxis (single-shot Cephalosporine). The technique was successful in 219 (90%) patients. In 23 (10%) cases a conversion was necessary to manage an adhesive or retrocecal appendix. The mean operative time was 32 (7–95) minutes. There was no intraoperative complication. Postoperative complications occurred in 11 cases (4, 5%), 7 of them were wound infections.
Conclusion: Single-port appendectomy is a safe and effective technique with minimal need of equipment. Generally it can be performed in all types of appendicitis, even perforated appendicitis. However, we do not recommend this procedure when perityphlitic abscess is present. If necessary, additional trocars can be introduced at any time.
Single Port Laparoscopic Surgery: Safe Procedure in Small Babies
Background/Purpose: The use of laparoscopy as a minimal invasive procedure has gained widespread popularity in the treatment of small babies` surgical diseases due to the excellent outcomes obtained with it. The present article reviews our experience with single port laparoscopic surgery in neonates and infants weighting less than 5 kilograms.
Methods: The medical records of nine neonates and infants weighting less than 5 kilograms, who underwent single port laparoscopic surgery over a period of 6 months, were retrospectively reviewed for demographic information, procedures, operative time, complications and outcomes. Only hemodynamically stable and non septic babies were considered candidates. The operations were performed with a hybrid device, made with an Alexis retractor® and a surgical glove. Conventional laparoscopic instruments were used.
Results: Four neonates and five infants were included in this study: 5 females and 4 males. The weight ranged from 2.5 to 5.4 kg (mean, 3.5 kg). The mean age was 68 days (range, 8 day to 6 months). Procedures performed included 1 hepatic biopsy, 5 hepatic biopsies with intraoperatory cholangiography, 2 ovarian cyst resection and 1 Meckel's Diverticum resection with colonic biopsy for aganglionic total colon suspicion. The mean operative time in hepatic biopsies with cholangiography was 84 minutes, 30 minutes for ovarian cyst resection, 50 minutes for hepatic biopsy and 120 minutes for Meckel`s diverticulum resection with colonic biopsies. There were no conversions to conventional laparoscopic or open surgery. All patients tolerated the procedure very well. One neonate had postoperative evisceration. There were no mortalities.
Conclusions: The skin elasticity and the great umbilical area respect to the body surface area make possible the use of multiport device in this age group. Our experience, suggest that single port laparoscopic approach is a feasible, safe and well tolerated procedure in neonates and infants with the additional advantage of having a small unique incision.
The First Experience of Application of the Single Port Laparoscopic Surgery in Operative Treatment of the Liver Cysts in Children in Russian Federation
Aim of the study: Laparoscopic operations began to take a considerable part in surgery of liver and bilious ducts in children. And as the technics of laparoscopic operations dynamically develop, we have applied for the first time an S-portal technique, and would like to present it to the world medical society.
Methods: We used a new tight attachment X-CONE, which provides stable placing opticians in the centre and full mobility of instruments, unlike other existing one-port devices, where instruments are fixed.
Main Results: Before operation full complex investigation including computer tomography of abdominal cavity with contrast, ultrasonic research of hepatobiliary zones, serological blood tests of oncomarkers and antibodies for echinococcus and alveococcus was carried out. We used a unique tight attachment X-CONE. For the port equipment the minilaparotomy is carried out: In the field of a belly-button the cut of 25 mm long is made. The surgeon consistently enters device halves (the same way as well as a retractor) and after that bridges them by means of a tight attachment. Toolings on LEROY, CUSCHIERI, CARUS have been used. Laparoscopic echinococcectomy was carried out with preliminary introduction of 2% formalin into cyst's cavity with 7 minutes exposition.
Conclusion: by results of our centre laparoscopic operations can be considered as «the gold standard» treatments of this pathology. Port X-CONE while use together with the bent instruments provides optimum triangulation, the review of a surgery field and carrying out exact intra- and extracorporal manipulations. Use of long optics gives the space for manipulations with instruments. Single Port Laparoscopic Surgery (SPLS) is natural continuation of a traditional laparoscopy on a way of depression in operation trauma and reduction of quantity of scars.
Initial Experience with Single Incision Laparoscopic Surgery in a Pediatric Hospital in Bogota
Background: Minimally invasive surgery is the current accepted approach for abdominal surgery. However, less invasive techniques such as single insicion laparoscopic surgery (SILS) are being used more frequently and we believe it will become the standard choice for abdominal surgery. This report describes our initial experience with Single Incision Laparoscopic Surgery (SILS).
Methods: We reviewed all the patients who underwent SILS in our hospital between November 2009 and September 2010. We used a surgical glove attached to a wound retractor to yield a multi-port hybrid.
Results: We present 46 patients with a mean age of 8.6 years and mean weight of 32 kg. The youngest patient was 8 days old and the smallest patient weighed 2.5 kg. The average duration of surgery was 50.7 minutes. The average length of stay was 46.6 hours. Different procedures were performed: appendectomies for early appendicitis (50%), hepatic biopsies (17.3%), appendectomies for complicated appendicitis (3 cases), and the following isolated cases: cholecystectomy, Meckel's diverticulum resection, oophorectomy, salpingo-oophorectomy, ovarian cystectomy, bowel biopsy, and a resection of an accessory spleen torsion. SILS was successfully completed in 44 cases, and 2 cases were converted to standard laparoscopy. There were no intraoperative surgical complications. Postoperative complications presented in 5 cases: a superficial incisional site infection, two residual abdominal abscesses, one bowel obstruction and one evisceration. The last two cases subsequently resulted in reoperation and occurred early in our learning curve.
Conclusions: SILS is a reproducible and viable technique that may be used successfully in pediatric surgery. It may be used safely in different procedures and age groups, even in neonates. Time of surgery decreased with our learning curve. Additionally, excellent cosmetic results were obtained as evidenced by imperceptible umbilical scarring.
Laparoscopic Single Incision Approach to Neuroblastoma: Early Experience of a Single Center
Laparoscopic approach to adrenal gland was introduced in 1992. Few papers have shown that it is feasible and safe approach to adrenalectomy in pediatric population. We present three cases of neuroblastoma patients treated with SILS approach. Between 12.2009 and 07.2010 we performed SILS adrenalectomy in two children and SILS liver metastasis biopsy in one patient. First case was an 11-month-old boy with disseminated neuroblastoma localized in both adrenals. Metastasis to liver and lungs were observed. Primary adrenal tumors were 4 cm in diameter. Open liver biopsy confirmed neuroblastoma. The child received 6 courses of chemotherapy. Adrenal tumor shrank to <2 cm with stabilization of pulmonary and liver metastases. The patient underwent modified SILS laparoscopy. In supine position 2.5 cm longitudinal umbilical incision was made. Covidien SILS Port was introduced. Additional 3 mm instrument was introduced at the xiphoid process to elevate the right lobe of the liver. Right adrenal gland was dissected with monopolar hook and Ligasure. Right adrenal vessels were clipped and cut, followed by complete removal of the adrenal gland en-bloc with the tumor. Splenic flexure was mobilized. Due to problems with tumor visualization mobilization spleen was mobilized, which required to introduce another 3 mm instrument to retract the stomach. 1 cm tumor localized in the peripheral part of left adrenal gland was removed with Ligasure preserving remaining adrenal gland. No hepatic metastases were seen. Tumors were removed in Endo-catch sac through the umbilical incision. Neuroblastoma was confirmed pathologically. Resection margins were clear. Operating time was 220 min. There were no postoperative complications, except a minor umbilical infection. Child continued chemotherapy and is free of disease at 9 months follow-up. Second case was a 15-year-old girl with left adrenal tumor. Ultrasound examination and abdominal CT showed 4 cm adrenal mass. The child underwent left SILS adrenalectomy in right lateral position. Covidien SILS Port was introduced in left epigastrium. Splenic flexure and spleen with caudal part of pancreas were mobilized with Ligasure. Adrenal vessels were clipped and cut, than left adrenalectomy was performed. Specimen was removed in Endo-catch sac. Operating time was 135 minutes. No postoperative complications were observed. Pathological examination revealed ganglioneuroma. Follow-up is 6 months without signs of local recurrence. The third case was a 1-year-old girl with a primary neuroblastoma localized in the posterior mediastinum and multiple liver metastases (stage 4). The child underwent initial open liver biopsy followed by induction chemotherapy, after which simultaneous thoracoscopy with removal of the residual scar tissue at the site of primary lesion and SILS liver biopsy were performed. Laparoscopy revealed several metastatic hepatic lesions. Both procedures were uncomplicated and child currently undergoes further chemotherapy and awaits bone marrow transplantation. The role of laparoscopic adrenalectomy in malignant adrenal tumors still remains controversial; however, there are some reports of using this approach in pediatrics. All SILS procedures in neuroblastoma were feasible and safe; however, there might be some limitations of this approach. Additional percutaneous insertion of 3 mm instruments may help. Further studies are required to investigate potential benefits of this approach.
Feasibility of Single Site Pyeloplasty in Piglets of Different Sizes
Background: Single site laparoscopic techniques are commonly applied for ablative procedures in the adult population and more recently have also been introduced in children. Furthermore some authors reported successful single site reconstructive procedures in adult patients. However, there is no experience regarding the feasibility of single site techniques for reconstructive operations in children. The aim of our study was to assess the feasibility and optimal techniques for pyeloplasty in piglets of different sizes.
Material and Methods: Four female piglets (weight ranging from 11 to 12 and 27 to 28 kg) underwent bilateral transabdominal dismembered pyeloplasty with one subumbilical SILSTM port.
The piglets were placed in a lateral position. After mobilization of the colon of the affected side, the hilar vessels and the pelviureteric junction was identified by use of a straight 5 mm monopolar hook and a bent 5 mm grasping instrument (Roticulator, Fa. Covedian). After resection of the pelviureteric junction and spatulation of the proximal ureter, the pelviureteric anastomosis was performed by a combined use of a straight 5 mm needle holder and a bent 5 mm grasping instrument, which allowed nearly normal triangulation for intracorporal suturing and knotting. The anastomosis was performed with 5.0 Vicryl© interrupted single sutures. Unburdening of the anastomosis was undertaken by endoluminal placement of a 4 Charr. stent in 4 of 8 pyeloplasties. After scarifying the piglets, determination of intact and impermeable pelviureteric anastomosis was veryfied.
Results: All SILS pyeloplasties were successfully performed with negligable blood loss. The feasibility of the procedure was not affected by the weight of the piglets. Operation duration of 4 cases with pelvi-ureteric stenting did not differ from 4 non-stented cases. There was a short learning curve for intracorporal knotting with acceptable mean total operation duration of 132 min (range: 55–190). However, we observed a significant learning curve regarding complications: Leakage 2 of 8 (1 stented, 1 unstented anastomosis) and stenosis in 1 unstented case occurred only in the first two animals.
Conclusion: A dismembered pyeloplasty with intracorporally performed pelviureteric anastomosis can be safely achieved in piglets indicating an anticipated feasibility for small infants. Best triangulation is guaranteed in SILS pyeloplasty in piglets, if one straight and one bent working instruments are used for suturing in case of demanding procedures and small working space. To avoid leakage and stenosis, stenting of the pelviureteric anastomosis is required.
Thorax
Thoracoscopic Repair of Congenital Diaphragmatic Hernia of Bochdalek While on Ecmo
Introduction: The minimally invasive approach to the repair of congenital diaphragmatic hernias (CDH) has become an accepted modality for these critical patients. Multiple studies have compared open to thoracoscopic repair, and nearly all of these studies have deemed extracorporeal membrane oxygenation (ECMO) an absolute contraindication to thoracoscopic repair of CDH. Concerns include transport to the OR while on ECMO, patient positioning with cervical cannulas in place, thoracic insufflation causing mediastinal shift, and bleeding complications which may be more difficult to control using minimally invasive techniques. We theorized that by using a previously developed protocol at our institution for the safe transport of infants on ECMO, meticulous positioning and monitoring, and careful surgical technique, the thoracoscopic method of repair may actually be a safe alternative as a result of smaller incisions, less dissection, and potentially decreased bleeding risk. We present a case of a successful thoracoscopic repair of CDH while on ECMO.
Case Report: The patient is a 36 week gestation male who was noted to have grunting, retractions and cyanosis shortly after birth. Chest x-ray demonstrated evidence of a left-sided CDH. The patient was intubated and transferred to our institution for further management. He was subsequently placed on venoarterial ECMO via right neck cannulation due to deteriorating cardiorespiratory status. On DOL 18 and weighing 2.2 kg, the patient was transported to the operating room using our transport protocol for a thoracoscopic repair of the CDH. The patient was carefully placed in a left lateral decubitus position which he tolerated without difficulty. Three ports (two 5 mm and one 3 mm) were used, and after reduction of the herniated bowel into the abdomen, the defect was closed primarily. Operative time was 86 minutes. Blood loss was minimal. The patient tolerated the procedure well and remained hemodynamically stable throughout. Fresh frozen plasma, platelets and amicar were available but were not given during surgery. Postoperatively, the patient was decannulated from ECMO seven days after CDH repair, slowly weaned from the ventilator, and was discharged home on DOL 81. Currently the patient is seven months old, on room air, and has no evidence of a recurrent hernia.
Conclusion: Thoracoscopic repair of CDH while on ECMO may be a reasonable surgical option in select patients. It may be especially beneficial in balancing the anticoagulation of the ECMO circuit and preventing patient and circuit complications following surgery performed while on ECMO. Further investigation is warranted to determine appropriate guidelines for patient selection.
Nuss Procedure: Decrease in Bar Related Complications with Primary Placement of Two Bars
Background: The Nuss Procedure, first reported in 1998 is currently the treatment of choice for pectus excavatum. The most significant bar related complication documented is bar movement, requiring reoperation in 3.4–27% of reports. Our experience compares the initial placement of one Nuss bar vs. two.
Methods: An IRB approved, retrospective chart review was performed of all Nuss procedures from November 2000 through February 2010. Since 2006, all initial Nuss procedures were started with the intent of placing two bars. Haller index, patient demographics, duration of surgery, length of stay, bar-related complications including broken wires, loose retention plates, and bar movement requiring re-operation were collected and compared for the one-bar vs. two-bar patient populations.
Results: A total of 97 Nuss Procedures on 85 patients (58 with one bar and 27 with two bar primary Nuss procedures and 12 revisions) were analyzed. Two attending pediatric surgeons performed all the procedures. Re-operation when one bar was placed occurred in 13 (22%) patients; 9 (15.5%) for bar movement, 3 (5.2%) for loose retention plates, and 2 (3.4%) for broken stabilization wires. No patients with initial placement of 2 bars had any of these complications or re-operations (22% vs. 0%, p = .007).
Conclusion: Our data demonstrates improved bar stability with no re-operative interventions when pectus excavatum is initially repaired with two Nuss bars. We support this change in all patients when feasible.
Haller Index During End-Inspiration Underestimates Surgical Indication in Patients with Pectus Excavatum
Background: The Haller index (HI) provides an accurate reference of the degree of chest wall compression in patients with pectus excavatum (PE). In these patients, an HI ≥3.25 indicates surgical correction. It is customary to assess HI by non-contrast computed tomography (CT) at end-inspiration (E-I), yet imaging during end-expiration (E-E) may better mimic PE severity observed at the operating table. The aim of our study was to evaluate variability of chest wall and cardiac compression parameters with breathing and whether such changes may impact surgical indication in PE patients.
Methods: We included twenty four PE patients referred for surgical consultation who underwent chest CT evaluation at both E-I and E-E (Brilliance 64; Philips Medical Systems, Eindoven, The Netherlands). HI was obtained by dividing the transverse diameter of the chest by the anteroposterior diameter, while cardiac compression index (CCI) was calculated dividing the transverse by the paramedian cardiac diameter transverse/paramedian). Paired T test was used to calculate the degree of change in HI and CCI with breathing. Pearson correlation was utilized to evaluate relationship among variables.
Results: Median patient age was 18 years old (25–75% interquartiles 14–28). HI and CCI values were significantly higher during E-E (Table). Eight out of ten (80%) patients without surgical indication during E-I (Haller index < 3.25) were considered surgical candidates when evaluated at E-E. There was a direct relationship between HI and CCI at both E-I (r = 0.83, p < 0.001) and E-E (r = 0.65, p < 0.001). Absolute and percentage change in HI did not correlate with change in CCI. Age had a direct relationship with CCI and HI at both respiratory phases but did not correlate with the change in HI or CCI.
p<0.05 vs. Expiration. Values are depicted as median (25–75% Interquartiles)
Conclusion: There is substantial variability in HI assessment with breathing which significantly alters candidacy for surgical correction. CT evaluation during E-I in patients with PE considerably underestimates disease severity.
Background: Pectus carinatum treatment is mostly performed with an open cartilage excision surgery. Different minimally invasive alternatives have been proposed in the last few years. Recently, a novel surgical technique has been proposed for the treatment of unilateral pectus carinatum, consisting of a thoracoscopic approach and multiple cartilage incisions. The purpose of this work is to present our modification to this aproach.
Methods: In 4 patients with unilateral pectus carinatum, we have modified the technique introducing a complete cartilage resection of the malformed cartlages, preserving the perichondrium through thoracoscopic aproach. Three ports were used. Cartilage is removed using a rongeur.
Results: we have performed this thoracoscopic tecnique in 4 patients during a period of one year. Ages were 13, 14, 14, and 15 years old. Follow-up ranged from 8 to 16 months. No intraoperative complications were observed. The results were excelent in 2 patients, good in one and fair in the first patient of our clinical serie, who was reoperated using a classical open aproach.
Conclusion: Thoracoscopic cartilage resection with perichondrium preservation can be considered as feasible alternative for the treatment of unilateral pectus carinatum chest wall deformity.
Laparoscopic Gastric Pull-Up and Thoracoscopic Esophagoesophagostomy Combined with Intrathoracic Fundoplication for Long Gap Pure Esophageal Atresia
The management of long-gap pure esophageal atresia (LGEA) remains controversial. Recently laparoscopy-assisted gastric transposition has been reported from a few institutes; however, a cervical esophagogastrostomy through mediastinal tunnel (Spitz technique) is performed. Our standard procedure for these infants has been gastric pull-up and esophagoesophagostomy in the right thorax combined with intrathoracic fundoplication. All of the patients with this procedure are doing well for the last decade. As minimally invasive techniques, we have performed the same procedure using combined laparoscopy and thoracoscopy without any assisted laparotomy and thoracotomy in an eight-month-old girl with LGEA.
Surgical Techniques: The patient was positioned supine. The first port for camera was inserted through the umbilicus and a couple of 5-mm ports were placed in the standard locations for laparoscopic Nissen fundoplication. The gastrostomy was taken down and closed using 4–0 absorbable sutures, and an additional 5-mm port was inserted at gastrostomy site. Laparoscopic gastric mobilization was performed; the short gastric and left gastric vessels were divided using harmonic shears and the whole stomach and distal esophageal stump maintained their vascular supply via the right gastric and gastroepiploic arteries. The distal esophageal stump received a triple 3–0 traction suture to allow the pull-up later. The hiatus was enlarged by radial incisions at both cruras and mobilized whole stomach and distal esophageal stump were pushed up into the right thorax through hiatus. The patient was positioned left decubitus and three 5-mm ports were inserted into right thorax. Pneumothorax with CO2 at a 4 mmHg pressure sustained a mild collapse of the lungs. Thoracoscopically upper esophageal pouch was dissected bluntly and then distal esophageal stump with whole stomach were pulled-up into the right thoracic space. The end of the distal esophageal stump with insufficient blood supply was divided using scissors and sufficient bleeding on the cutting edge was observed. Esophagoesophagostomy was performed interrupted 4–0 absorbable sutures and wrapped by 360-degree gastric fundoplication. The patient was positioned supine again and attention was turned back to the abdomen. The pulled-up stomach was found to be appropriately positioned and fixed to the thoracic inlet. Heinecke-Mikulicz pyloroplasty was also performed with interrupted 4–0 sutures. Operation time including changes of patient's positioning and dressing was approximately 6 hours.
Conclusions: The patient had mild anastomotic stenosis requires balloon dilatations; however, she is eating baby food well with neither vomiting nor respiratory distress. Postoperative intrathoracic gastrofiberscopy showed well-maintained fundoplication and her parents are also satisfied with 7 small wounds cosmetically. Our laparoscopic gastric pull-up and thoracoscopic esophagoesophagostomy with intrathoracic fundoplication is feasible and is an excellent option in selected patients with LGEA.
How Choose the Approach to Repaired the Eventration of Diaphragm in Children by Thoracoscopic or Laparoscopic Surgery?
Purpose: To introduce the approach and method to repair the eventration of diaphragm in children under endoscopy.
Methods: From May 2007 to Feb. 2010, ten children with eventration of diaphragm were treated in Shanghai Xinhua Hospital by thoracoscopic or laparoscopic surgery. Seven were Right-sided eventration and three were left. 6 are male and 4 are femaie. The age of the patients was ranged from 3 months to 2 years old.
Result: All cases were finished the operation of diaphragm plication to repair the eventration under laparoscopic or thoracoscopic procedure.. 7 right-sided eventration were repaired by thoracoscopic surgery, 3 left-sided eventration were treated by laparoscopic surgery. Ten patients recovered very well. All of them grow well during the 2 months to 2 years after operation. Compared with the preoperative, the level of the top of diaphragm was depressed one to three ribs at eventration side. No complications presented during operation or postoperation. The cosmetic effect was obvious on the operative chest well compared with open surgery.
Conclusion: The diaphragm plication can be finished under endoscopic. Thoracoscopic procedure is recommended to repair the right-sided eventration diaphragm. Laparoscopic is recommended for left-sided eventration to avoid damaged the bowel under the left diaphragm.
A Novel Shape-Ready Metal Bar for Minimally Invasive Repair of Pectus Excavatum: A Preliminary Report
Introduction: Minimally invasive repair of pectus excavatum, first described by Nuss in 1998, has been soon adopted through out the world during the past decade. Due to a lack of understanding on morphologies and repair techniques, this patient-specific approach has undergone a serious learning curve. Therefore, a novel shape-ready metal bar with its predigested technique had been designed and adopted to our patients. We aim to evaluate the initial post-operative results regarding on factors related to postoperative complications and to examine the acceptability of this new approach by the patients.
Patients and Methods: Twenty-four patients (21 male and 3 female) were operated on between June 2009 and August 2010 at the Department of Pediatric Surgery, Xinhua Hospital, Shanghai Jiaotong University School of Medicine. Standard Nuss procedure had been adapted to the first 8 patients in these cases (median age, 8 years; range, 3 to 12 years) during the first six months before the shape-ready bar were introduced into clinics. The left 16 patients (median age, 10 years; range, 3 to 17 years) had been operated on using the shape-ready bar during the next 8 months. While the novel metal bar was designed with a removable introducer, the operation could be predigested into one step instead of passing through with a introducer and pulling back with the metal bar in the standard Nuss procedure.
Results: There was no significant difference in haller index between patients who undergone Nuss procedure and who undergone the new technique (Nuss, 5.18 ± 0.38; shape-ready bar, 4.96 ± 0.62; P > 0.05). Duration of the surgery was longer with the Nuss (Nuss, 60.38 ± 12.92; shape-ready bar, 42.88 ± 6.75; P < 0.01). No postoperative pneumothorax and hemothorax were found in the patients with shape-ready bar, while 1 case of pneumothorax was recorded in the Nuss patients.
Conclusions: The Nuss procedure for repair of pectus excavatm has been accepted worldwide because of its minimal invasiveness and excellent cosmetic results. We designed a novel shape-ready metal bar, combining a removable introducer, which can be inserted under the sternum in one step. This predigested technique, based on the Nuss procedure, which requires neither metal bar curving before operation nor metal bar turning over during the operation, is effective. Since the tunnel for inserting the bar is shorter than that of the standard Nuss procedure, injuries during inserting and removing the metal bar could be less. Further evaluation requires long-term follow-up.
Total Laparoscopic Single-Stage Duhamel-Martin Pull-Through for Hirschsprung Disease Performed in the Neonatal Period
Background/Aims: Whilst minimally invasive approaches to the management of Hirschsprung Disease (HD) are becoming increasingly popular, the Duhamel pull-through is being performed less frequently. We report our initial experience of total laparoscopic single-stage primary Duhamel-Martin pull-through performed for HD in the neonatal period.
Methods: Single institution retrospective casenote review. The procedure was performed using a 5 mm right-upper quadrant port and 2 additional ports (3 mm & 5 mm). Laparoscopic levelling seromuscular biopsies were taken and the colonic mobilisation and retrorectal dissection also performed laparoscopically. The aganglionic colon was isolated with ligatures and removed per rectum via the retrorectal tunnel. Following completion of the colo-anal anastomosis, the spur was divided in its entirety per-rectum under laparoscopic vision using multiple firings of a linear stapler. Finally, the anterior proximal end of the native rectum was anastomosed laparoscopically to the stapled/cut edge of pulled-through colon with interrupted intracorporeal sutures. A covering stoma was not used.
Results: The procedure was successfully completed in 2 infants (1 male) diagnosed with HD in the neonatal period. Gestational age at birth was 37 and 40 weeks, age at presentation was 2 and 3 days, diagnosis of HD was made at 13 and 12 days, and surgery was performed at 21 and 17 days of age. Weight at surgery was 3.1 and 2.8 kg. Feeds were commenced on the second post-operative day in both cases; infants passed stool on post-operative days 2 and 1 and were discharged home on post-operative days 5 and 4 at an age of 26 and 21 days. Procedural time was 360 and 315 minutes. There were no peri-operative or post-operative complications. Follow-up is 27 and 14 days.
Conclusions: The Martin modification of the Duhamel pull-through allowing complete obliteration of the rectal spur using a total laparoscopic approach without eversion of the bowel per rectum as a single-stage procedure in the neonatal period is feasible. Immediate post-operative recovery is rapid and cosmesis excellent. We intend to further evaluate the long-term outcomes of this technique as we favour the modified Duhamel pull-through for our patients with HD.
Pectus Excavatum Repair According to Nuss: Is it Safe to Place a Retrosternal Bar Under Thoracoscopic Vision?
Introduction: The minimally invasive repair of pectus excavatum (MIRPE) has been popularized by Donald Nuss all over the world since 1998. Compared with the Ravitch procedure, MIRPE “requires neither cartilage incision nor resection.” Nevertheless, patient satisfaction is the same for both procedures. The indication is most of the time for a cosmetic result. Thus, incidence of cardiac or pericardium injuries during retrosternal dissection or at the time of bar removal is low but remains the main topic of preoccupation.
Case Report: A 18 years-old boy had a moderate deformity of his thoracic cage (Haller Index: 3.5) but the psychological consequences of this pectus excavatum seemed to less and less tolerated during a 15 month period when the surgeon was consulted three times. A Ct scan did not reveal any other malformation. Preoperative investigations revealed normal complete pulmonary function. The echocardiogram and the electrocardiogram were normal. Under a right thoracoscopic control, the introducer reached the left pleura beginning the dissection of the anterior mediastinum in a cranial position and sliding down slowly behind the sternum to reach the good level for correction. As the introducer was going outside through the left intercostals space, arrhythmia was noticed by the anaesthesiologist without bradycardia or hypotension. The electrocardiogram could be modified by the presence of the introducer. One umbilical tape replaced the introducer and was left in place. Bradycardia and hypotension occurred and a pericardial effusion could be observed by the right thoracoscopy. Through a left thoracoscopy nothing abdormal was seen. An echocardiography could confirm a cardiac tamponade. A sternotomy was immediately performed. Two wounds in the heart were sutured, one in the right atrium and one in the right ventricule. A massive transfusion was required but no cardiac massage. A transoesophageal echocardiography revealed no damage of the tricuspide valve. The patient recovered quickly. The hospital stay was 7 days. He is asymptomatic and still has a pectus excavatum.
Discussion: Indications for pectus excavatum repair must be seriously discussed with patients and parents. They must be informed about other treatment and procedures and all complications that can occur. Numerous issues must be explained including cardiac injuries: pneumothorax, hemothorax, bar displacement, allergy, infections, incomfort and pain, difficulties encountered in case of need for cardiac resuscitation. Many recent papers propose to modify the original Nuss procedure to minimize the occurrence of severe complications. Retrosternal dissection with an introducer assisted by a right thoracoscopy, dissection with two thoracoscopic instruments, enven bilateral thoracoscopy, cannot avoid cardiac injuries. The extrapleural way can be a good alternative with or without thoracoscopy. Relaxing or lifting the sternum can help to the placement of the bar and direct subxiphoid dissection too. Comparison of the Nuss and Ravitch and other cosmetic procedures must be discussed.
Modifications of Nuss Procedure for Treatment of Chest Wall Malformations in Children: Our 10-Years Experience
Pectus excavatum is the most common chest wall deformity in children. The Nuss procedure for repair of pectus excavatum has been accepted worldwide because of minimal invasiveness and excellent cosmetic results. Since 1961 we have performed more than 2500 surgical procedures in children with chest wall malformations. As soon we have found some results of Paltia procedure unsatisfied we started to use our modification of Nuss thoracoplasty as procedure of choice. Our modifications of Nuss procedure include: T-shaped wide bar of our own design, the creation of chest tunnel from left to right with the introducer of our own design, the fixation of the bar to ribs, the removing of the bar after 4–6 years.
Since 2001, 290 Nuss procedures were performed for pectus excavatum in children. Mean operation time–38 ± 7 min. We used the single bar in all cases, except for one. The thoracoscopy was performed in 8 children: after failed Paltia procedures (4), after sternotomy for heart surgery (3) and after pulmunoectomy (1). In 4 cases we performed simultaneous operations: Nuss procedure with thoracoscopic ductus arteriosis closure (2) and Nuss procedure with thoracoscopic pulmonary operation (2). We also used Nuss procedure for the treatment of combined wall deformity (6 children), such as Poland syndrome, etc.
Children were allowed to be active on 3–7 day after operation.
The age of our group ranged from 3 to 21 years. Mean age 11.8 ± 3, years. More than 65% of our patients had pectus excavatum Grade 3. 52 children had associated genetic anomalies.

Complications: 2 hemothorax, 2 pneumothorax, and 1 bar displacement occurred in early postoperative period. In long-time period 1 bar rejection and 1 hypercorrection were found.
In 92 children bar was successfully removed after 2.4–6 years. In more than 95% children we have excellent cosmetic results. In 6 children moderate remained deformity of chest wall was observed. These patients underwent Nuss re-operation with good efffect.
Conclusion: We consider Nuss operation to be the perfect choice for correction of pectus excavatum. Our modifications were aimed on increasing of effectiveness of Nuss procedure and enabled the prevention of severe complications and bar displacement.
Thoracoscopic Anatomic Lobectomy and Segmentectomy for Benign Lung Lesions
Abstract Withdrawn
Thoracic/Lumbar T2, T3, T4 and L3 Superselective Endoscopic Sympathetic Block (ESB), for Disabling, Palmar, Facial, Axillary and Plantar Hyperhidrosis and Erythrodermia of Childhood and Adolescence
Abstract Withdrawn
Early Elective Video-Assisted Thoracoscopy (VATS) for Pleural Empyema in Children and Adolescents
Aims: The treatment algorithm of postpneumonic pleural empyema is a matter of continuous debate. After initial antibiotic treatment, the selection and optimal timing of invasive treatment were evaluated. The principal question was when to perform VATS in the course of treatment, whether in the early phase of fibrinous exudate formation or in the late phase of constrictive fibrous plaque formation.
Patients: During a 4 year period, 13 patients were treated for pleural empyema at the Department of Paediatric Surgery, Regensburg. 6 of these were treated by early VATS (`E-VATS`), 4 had late surgical intervention (`L-VATS`) and 3 were treated by primary thoracotomy.
Results: In the E-VATS group, no conversions were necessary, whereas in one of the L-VATS patients a conversion to open thoracotomy and lobectomy was found necessary. All the patients undergoing early VATS had an uneventful post-op recovery with complete resolution of the pleural thickening whereas in the late VATS group persistent fever, prolonged ventilation, respiratory insufficiency and atelectasis were common post-op complications.
The duration of ICU-treatment and hospitalization in the late VATS group was significantly higher. The operations were less extensive and faster in the early VATS group as we will demonstrate with several cases.
Discussion: Our experience suggests that VATS should be considered at as soon as there is echogenic pleural fluid or there is pleural thickening failing to resolve with antibiotic treatment. Given that pleural drainage in children is generally carried out under general anaesthesia, VATS can easily be combined with this to provide further diagnostic information and guided therapy. Thoracoscopy reduces the risk of lung puncture and allows more precise drainage placement. If fibrinolytic therapy is considered, prior VATS is recommended for inspection and to eliminate adhesions.
Thracoscopic Resection of Long Tubular Esophageal Duplication Extending to the Almost Entire Length of the Esophagus
Introduction: Esophageal duplications are unusual congenital anomaly in gastrointestinal duplications, furthermore long tubular duplications of esophagus are very rare. We report a case of 23-months-old male with tubular esophageal duplication, extending from the neck to the esophagogastric junction, treated thoracoscopically.
Case Report: He was admitted to our institution for stridor and vomiting after birth, and poor body weight gain at 11 months old. Upper gastrointestinal contrast study showed the esophageal duplication in parallel at left side of native esophagus, and the duplication was communicated with native esophagus at the esophagogastric junction. Proximal site of the duplication was not communicated with native esophagus, and gastroesophageal reflux was recognized. Endoscopy showed severe reflux esophagitis (Los Angels classification grade C) and the duplication had common wall between duplication and native esophagus in endoscopic ultrasonography He underwent the thracoscopic resection of the duplication 12 months later after diagnosis. In right lateral decubitus position, parietal pleura incised on lower esophagus, and then esophagus and duplication picked up together. We incised duplication, confirmed the communicated lesion, and closed. We incised the border with duplication and native esophagus longitudinally and left the muscle layer of the common wall. Residual mucosa of duplication was coagulated by electrical coagulator. We successfully completed tubular esophageal duplication thracoscopically. He had minor leakage from the closure site, but the leakage was healed conservatively. Gastroesophageal reflux disappeared and doing well after this procedure.
Conclusions: Thracoscopic resections for long tubular esophageal duplication are feasible, safe and efficient procedure. Surgeon had a better visualization of the duplication from the upper mediastinum to lower mediastinum above diaphragm. Resection can be as complete as in open procedure without complicating the technique. It avoids cosmetic and functionnal disorders due to thoracotomy.
Thoracoscopic Thymectomy for Myasthenia Gravis in Children
Minimally invasive surgery (MIS) has been proved to be a good approach to different thoracic surgeries in the pediatric population. Myasthenia gravis (MG) is an autoimmune disorder in which antibodies against the acetylcholine receptor are produced, resulting in progressive muscle weakness. When medical treatment is not sufficient to control the symptoms, complete thymectomy is indicated. Thoracoscopic thymectomy has been described before showing equal results compared to open surgery, adding the benefits of MIS. The aim of this report is to describe our experience in video-assisted thymectomy for MG.
From June 2002 to September 2010, we performed a total of fourteen thymectomies, 3 male and 11 female, mean age was 10 years (2 to 14 years). Ten patients had thymic hyperplasia, 1 thymic involution and 3 were normal thymus, none was associated to thymoma.
The first three procedures in this series were completed by a right approach; one patient suffered an unnoticed contralateral phrenic nerve injury, developing left diaphragmatic palsy in the postoperative period. Decision was made to perform the following cases through a left thoracoscopic approach.
Complete thymectomy was achieved in all cases with no conversions to open surgery. No other intraoperative complications were present. There was no surgical mortality. One patient developed a myasthenic crisis in the early postoperative period associated with the administration of azythromycin.
Clinical improvement was observed in all patients during follow-up (1 to 99 month), 6 are currently asymptomatic, 7 patients improved their clinical symptoms dramatically, decreasing dose in their medical treatment. One patient who showed improvement of symptoms, died for a non related reason.
We believe that complete thymectomy can be achieved by this approach, is technically feasible, with a low rate of complications, associated with minimal pain after surgery and good cosmetic results. We conclude that MIS should be considered as the first technical option for thymectomy in MG patients.
Congenital Stenosis of the Esophagus: Laparoscopic Resolution
Aims: the esophageal stenosis due to extrinsic cause is a non-common disease that usually presents vomits and growth failure. It is defined as an intrinsic stenosis of the esophagus present, but not necessarily symptomatic, since birth; caused by a congenital malformation of the architecture of the esophageal wall. Thirty percent (30%) is associated to other anomalies. The initial treatment usually consists of intraluminal dilatation, and surgery is reserved only for those with no response.
Material and Methods: female patient of 1 and a half-year-old reports background-preceding-precedent of SOB and narrowness of aortic valve. She presents persistent vomiting with progressive dysphagia and a halt-stagnating in weight raise. At admission she was 7.600 kg (pc–3) with a deficit of the 30% (dnt moderate) TEGD: esophagus at the site of third half with lower third present narrowing of 4 mm long with stasis of medium of contrast; esophagus supra and sub stenotic with acceptable diameter which suggests esophageal stenosis. A fibroesophagoscopy was made, entering fibroscope 18 cm from ads where, a stop is made due to persistent narrowness with no sign of esophagitis so that the esophagoscopy can not continue to the stomach. An esophageal monometry was not done, neither a pHmetry. dilation with catheter balloon for l urethral dilation of 7 fr was performed twice without succeeding in cleaning the narrowed area. A surgical repair is then performed with removal of the stenotic area by right thoracoscopic. A complete esophagectomy was performed and then anastomosis end to end performed at separated stiches of pds 5.0 with extracorporeal knots.
Results: Operating time was 150 minutes. There was no significant intrasurgical bleeding. Feeding started after the third day trought transanastomotic probe by gavage. Seven days after surgery a new transit with good passage of contrast to stomach with a small leakage at anastomotic level. After 13 days of fistula persistence, with low debit through pleural probe, parenteral feeding started. Due to poor weight gain, at day 23 laparoscopic gastrostomy was performed with placing of transpyloric catheter for constant feeding. After four days, medical discharge was indicated. On day 30 after surgery a new oesophagogram was repeated and a complete closure of the fistula with small narrowness of 4 mm in length could be seen in the area of surgical anastomosis, with moderate prestenotic dilation. Good stomach passage without gastroesophageal reflux. Three months after surgery a new endoscopy was performed with good passage through the anastomosis and with no obstructions or difficulties. The gastronomy probe was retreat.
Conclusions: The E.C.E diagnosis is frequently problematic and the therapeutic approach is controversial. Even when the traditional treatment of this pathology is dilation via buginage or balloon under fluoroscopic guidance, it needs multiple sessions with possibility of complications (esophageal perforation, post dilatation scars, restenosis) in some specific cases, the possibility of a surgery may be consider, being laparoscopic approach a safe and feasible technique.
Single Incision Video-Assisted Thoracic Surgery (SIVATS) for Parapneumonic Thoracic Empyema
Introduction: In this series of parapneumonic thoracic empyema we emphasize the interest of combining single incision with endobronchial blocker and gasless VATS.
Materials and Methods: A retrospective single center study of 50 consecutive cases between January 2003 and August 2010 was performed. Indication, medical history, preoperative imaging, laboratory findings, operative technique and results were recorded.
Results: All 50 patients were admitted at our pediatric intensive care unit (PICU), 39 of them (78%) were transferred from other hospitals. Mean age was 60 months (range 8–180), mean WBC count was 18.500/microliter; mean CRP was 28 mg/dl. General anesthesia with endobronchial blocking device (Arndt Pediatric Endobronchial Blocker, Cook® or Fogarty 4F, Edwards Lifesciences®) was used in all except one case. A single incision of 2 cm was made on the mid-axillar line just below the inferior angle of the scapula, and gasless VATS was performed. Camera and instruments were introduced directly through the incision (no port). There were no per-operative complications; there was no conversion to thoracotomy. Most patients (48/50) were extubated in the operating room. Mean PICU stay was 7 days (range 4–21). We noticed one recurrence which was treated by redo (SIVATS). Long-term results are excellent.
Conclusion: SIVATS with endobronchial blocker and without carbon dioxide insufflation is a safe and effective method for treatment of parapneumonic empyema. We propose an algorithm for the management of this pathology based on our experience and on literature review.
Thoracoscopic Central Venous Access Placement in Azygos Vein in Children with Intestinal Failure and Multiple Venous Thrombosis
Background: Patients with intestinal failure (IF) depend on patency of vascular access for parenteral nutrition (TPN). Multiple thrombosis of venous trunks may be a significant challenge in children with IF. We report the minimally invasive approach of the azygos vein in 2 patients with IF.
Material and Methods: Patients with IF and signs of vascular thrombosis were evaluated through MDCT scan for vascular patency. When superior vena cava (SVC) and inferior vena cava (IVC) were found nonpatent, alternative non conventional sites for line placement were used, like hepatic vein access. In 2 patients, a thoracoscopic azygos central line placement was performed in 3 ocasions.
Surgical Technique: Position: prono-lateral left decubitus. Five mm trocar placed in 4th intercostal (IC) space for camera; 3 mm aditional port for suction and lung retraction. Controlled neumothorax at 5 mmHg pressure. Surgeon at the back of the patient and assistant at the front. This approach can be done transpleurally or extrapleurally. Percutaneous puncture is made through 5th or 6th IC space, close to the spine. In the transpleural approach the pleural cavity is entered, and under direct vision the azygos vein is punctured in cephalic direction. A guide wire is then passed through the right atrium, under fluoroscopic control. Using Seldinger technique, a Hickmann 7 french catheter (BARD®) is tunelled from the anterior chest wall and passed centrally. For the extrapleural access, the thoracic cavity is entered with the needle within the extrapleural space; saline solution is instilled creating a virtual cavity; then, without entering the pleural space, the azygos vein is accessed and the catheter passed in the same way.
Results: 3 procedures were completed in 2 patients with IF caused by gastroschisis and intestinal atresia respectively. Both patients had had a STEP procedure and one of them had a failed intestinal trasplantation. Both were TPN dependent, with different amounts of enteral feedings. Case 1: 1st transpleural access was inserted at 33 months old and 2nd extrapleurally at 4 years. The line permanence was 9.4 years 3.5 months respectively. Both were retired because of catheter related infection. Case 2: An extrapleurally inserted line was placed at 16 month of life and last until now (10 months). There were no intra or postoperative complications, neither in the placement or retirement of the lines.
Conclusion: The thoracoscopic approach to the azygos vein is a useful alternative in patients with IF dependent on TPN with no other vascular access. Although the best approach should be the prevention of venous thrombosis, this is a safe option for these extremelly difficult cases.
Technical Modifications in Thoracoscopic Repair of Esophageal Atresia. Our Experience
Objective: To evaluate technical modifications in our learning curve in the thoracoscopic repair of esophageal atresia.
Material and Methods: We analize the series of patients with esophageal atresia (EA) which underwent thoracoscopic repair in our hospital during two periods, 2002–2004 and 2007–2010. During those periods we treated a total of 21 patients, 3 of which were esophageal atresia type I and the other 18 were type III. 10 of them had associated malformations of which the most frequent were cardiac malformations. In all the cases, one 5 mm and two 3 mm trocar were used, a 5 mm 30 degree telescope, and an additional clamp without trocar to compress the lung in two cases.
Results: During the first period we had to convert to open surgery 6 of 13 patients for several reasons—too much tension in the ends in two type I and one type III atresias, impossibility for compressing the lung resulting in bad visualization in another case, a right aortic arch in one more and another one due to patient instability resulting from a complex cardiopaty. We felt that there were too many technical difficulties and later complications that made us stop and think. Two years later after improve our experience in minimal invasive surgery (MIS) in several ways we returned to a thoracoscopic approach of EA. We made some changes in the type of trocars and their position, in instruments, in ways of introducing sutures and some additional tricks to reduce manipulation of the esophagus, using selective intubation, etc. That allowed us to work more confortably, with a more ergonomic position and an enhanced and more stable operating area, facilitating both dissection and suturing, reducing unnecessary movements and therefore reducing fatigue and improving technical precision, with a reduced time in surgery and less complications. In the second period we had to convert one type I case, and suspend another one after closing the fistula, caused by a severe heart disease. We had no severe complications like recurrent traqueoesophageal fistula and only two mild stenosis wich were resolved with pneumatic dilatations in two patients.
Conclusions: Thoracoscopic repair of esophageal atresia is maybe the most difficult and more technically demanding surgery in MIS. In order to improve the results we think it is important to introduce experimental animal surgery, and to look for an appropriate small model, and the kind of surgeries such as inguinal hernias where it is possible to improve suturing, as a common practice for attendants as well as medical internal residents in pediatric surgery.
Lessons Learned with Long-Term Follow-Up of Thoracoscopic Repair for Esophageal Atresia
Background: Oesophageal atresia (OA) is a group of congenital anomalies with interruption of the continuity of the oesophagus with or without a persistent communication with the trachea. Advancements in neonatal surgery have allowed pediatric surgeons to approach this procedure using minimally invasive surgery with excellents results.
Objective: To evaluate the feasibility and results of thoracoscopic repair in various types of esophageal atresia (EA), and to report some tips you can perform to obtain a much better result.
Methods: During a period of 36 months, 12 patients born with an esophageal atresia and tracheoesophageal?stula underwent thoracoscopic repair. Four of them were females, and eight males. Weights ranged from 1.9 to 3.5 kg and gestational age of birth was between 35 to 39 weeks. Nine had another congenital malformation associated.
Results: The majority of our patients had a tipe III AE. All of them underwent the same thoracoscopic procedure. 11 were completed successfully by thoracoscopy, and without any intra-operative complications. An esophageal end to end anastomosis was performed in 10 cases. One of these procedures had to be converted to open surgery, in a patient with log–gap AE. Two patients had long-gap atresias, and they underwent laparoscopic gastrostomy with proximal esophageal aspiration for 5 to 7 weeks to approximate the ends of the esophagus to two vertebrae apart. A left chest tube was installed in 10 patients. All patients had a transanastomotic tube after surgery and oral feeding was started between day 3 and 4. None of them presented suture dehiscence. 6 patients required esophageal dilatation, at least one time (1–6 times). 4 patients developed esophageal stenosis due to gastroesophageal reflux, needing Nissen Fundoplication + Gastrostomy).
Conclusion: Over the past three years we have increased our acknowledgement and we are able now to perform a successful minimally invasive procedure in these children. After this serie of AE, some tips can be useful to perform this procedure safely.
Always perform echocardiography before surgery, to determine aortic bow position Right semi prone position of the patients 1st trochar always placed under the tip of scapula The 2nd trochar in the axilla region The 3rd trochar is placed according to surgical evaluation of esophageal ends, generally at 7° intercostals space
MIS Approach to Pulmonary Hydatid Cysts
Aim and Objective: To assess the role of Minimally Invasive Surgery in the management of Pulmonary Hydatid Cysts in children.
Materials and Methods: A review of 9 patients who underwent minimal invasive surgery (MIS) for Pulmonary Hydatid Cysts in children. 6 of them were unilateral and 3 were bilateral. 3 of them also had additional liver hydatid cysts. In one child, the cyst had a bronchial communication. The age ranged from 2 years to 11 years (Mean 4.2 years). All children were pre-treated with Albendazole.
Results: In all children but one, thoracoscopy was performed, the cyst fluid was aspirated, scolicidal agent injected and then the cyst was opened and the germinal layer completely removed. Intercostal drainage was required for a few days. All the 3 children with bilateral lung hydatid were operated on both sides in the same sitting. Those who had associated liver hydatid cysts underwent laparoscopic surgery later. The child who had a bronchial communication provided us with an opportunity for bronchoscopic removal of the membrane and avoided all the potential morbidity of excising a deep seated lesion. All the children have done well.
Conclusion: Thoracoscopy offers an excellent option for surgical management of pulmonary hydatid cysts and avoids the morbidity associated with open surgical methods. Bronchoscopic removal is an attractive alternative in those with a bronchial communication.
Thoracoscopic Repair of a Chest Wall Lung Hernia
Herniation of the lung through a traumatic chest wall defect is a rare occurrence. A 10-year-old boy sustained focal blunt trauma to the chest in a bicycle accident resulting in a thoracic handlebar injury. Eight weeks after the accident he presented with a painful area in the left midclavicular, fifth intercostal space with intermittent swelling. He did not have any significant respiratory symptoms except for discomfort and the presence of an outward protrusion on the anterior chest with inspiration, cough, and valsalva. Chest radiograph was normal. Findings were consistent with a lung hernia.
We present a video illustrating the technique of thoracoscopic repair of a 6 × 3 cm intercostal chest wall hernia with placement of a Goretex patch. The procedure was accomplished using a three-trocar approach and complete resolution of the lung hernia was achieved. The patient has remained asymptomatic at one year of followup without evidence of recurrence. Handlebar lung hernias are rare, with approximately 20 reported cases in the literature, most involving children. This case illustrates the feasibility of repair using thoracoscopic and minimally invasive techniques.
Treatment of a Densely Fused Fissure During Thoracoscopic Right Middle Lobectomy
Aim: During major pulmonary resection using thoracoscopy, a Ligasure device or bipolar sealing device is commonly used for sealing the cut lung tissue and fissure surfaces. However, in cases where a fissure is fused so strongly that it cannot even be identified, there is a risk for air leakage after major pulmonary resection. We report a case with a fused fissure between the right upper and middle lobes, where a surgical stapler was thought to be better for creating a division between the right upper and middle lobes than a Ligasure device because we considered that it would not seal the lung parenchyma effectively.
Case: A 2-year-old girl with congenital cystic adenomatoid malformation (CCAM) of the right middle lobe (RML) was referred to our institution for further management after a series of infections. The patient was positioned in the lateral decubitus position and single lung ventilation was used. The first 5 mm port was placed in the fifth intercostal space in the anterior axillary line to determine the position of the fissure and evaluate the general condition of the lung parenchyma. Four additional ports were placed. A Ligasure device was used to decompress multiple cysts, causing the RML to collapse completely. Upon close examination the lung fissures were found to be fused. In particular, the minor fissure was so densely fused it could not be distinguished at all. Firstly, the vein of the RML, which drains into the superior pulmonary vein, was isolated and divided using endo-clips. Then, after exposing the bronchus, it was encircled with a thick silk tie to act as a traction suture. By applying traction and counter traction, access to the bronchus was enhanced and it could be divided using endo-clips. Finally the arteries of the RML could be identified and ligated. By doing so, a line demarking the major fissure could be identified, dissected and a stapler device used to seal the lung parenchyma and create a division between the right upper and middle lobes. In other words, the lung parenchyma did not need to be dissected to search for the fused fissure. Currently after follow-up of 16 months, she is well, with no episodes of respiratory distress or recurrence of symptoms.
Conclusion: Our technique of dividing the pulmonary vein, then the bronchus, then the pulmonary artery then the fused fissure is safer and can be applied whenever fused fissures are encountered during thoracoscopic pulmonary lobectomy.
Thoracoscopic Diaphragmatic Hernia Repair in Newborn: The Effect of the Sequence of Suture Application and Sac Excision on Surgical Working Space
Thoracoscopic repair of diaphragmatic hernia (DH) could be successfully performed with a delicate anesthesia, low CO2 insufflation flow and pressure, and even transient interruption of gas flow. To initiate the repair of DH by thoracoscopy, one of the basic aims should be to obtain a working space. This video states the importance of timing of suspension and closure suturing just before the excision of the sac.
Case Report: A thoracoscopy was performed in a 3-day-old male newborn having a diagnosis of Bochdalek type congenital diaphragmatic hernia. He was admitted with dyspnea and tachpnea following the birth. A 4 mm sub-scapular optic port and two 3 mm working port were introduced into the thorax and then abdominal organs were reduced into the abdomen. Two suspension sutures were applied just on the middle of the defect before hernia sac excision. By hanging the suspension sutures at out of thorax, the defect orifice was narrowed. The hernia sac was pulled into the thorax from a narrow gap just at the lower end of the defect. The sac was excised and pulled outside from inside of a working port. While the suspension sutures were hanged, two interrupted polypropylene 2/0 sutures onto the lower end, and two similar sutures onto the upper end of the defect were applied and then two suspension sutures were released and tied in thorax on the mid part of the defect. The patient did well postoperatively and was discharged on postoperative 11th day.
Thoracoscopic Oesophageal Atresia Repair: Is the Cosmetic Argument Just Cosmetic?
Introduction: Better cosmesis is a common justification for endosurgical alternatives to open surgery. Excellent cosmetic outcomes can, however, be achieved by minimally-invasive open surgery (MIOS) pioneered by Bianchi. We hypothesised if cosmesis is a leading reason to choose such approaches, uptake of MIOS would be at least similar and perhaps greater than endosurgical alternatives since it is older, requires less specialized resources and typically uses only a single incision.
Methods: We compared MIOS (axillary) and endosurgical (thoracoscopic) approaches to oesophageal atresia (OA). To approximate uptake of each procedure we measured the overall number of cases reported in the literature by searching Medline, SCOPUS, ScienceDirect and ISI Web of Knowledge. We also compared the number of citations accrued by each paper originally reporting the technique (from Bianchi and Rothenberg respectively). All citing articles for the index reports were identified and counted. Papers from these Tier 1 articles (those citing the index publication) were restricted to those where the original procedure was actually used, modified or substantially reviewed. Papers that cited a paper en passant were excluded, e.g., a thoracoscopic series that merely mentions the axillary approach. All articles citing the selected tier 1 articles were identified as tier 2 articles and the process continued until no further relevant citing articles were found. To provide greater information on the MIOS approach (reported principally from the originating centre), we analysed our experience with axillary OA repair to September 2009 using retrospective case-note review.
Results: More than 375 cases of the thoracoscopic approach have been reported whilst the reports of the axillary approach include <75 cases. Bibliometrics for the thoracoscopic index paper include 310 citing articles vs 32 for the axillary approach. Publications do not indicate cosmetic superiority of either. Our 11 patients had birth weights between 2070 and 3700 g. Two repairs were via left-sided axillary thoracotomy due to right-sided aortic arches with uneventful recoveries. In one patient, a delayed primary repair was performed later through a standard thoracotomy and required a colon interposition after an anastomotic leak. There were no deaths. Cosmesis of the axillary approach was informally judged excellent by parents.
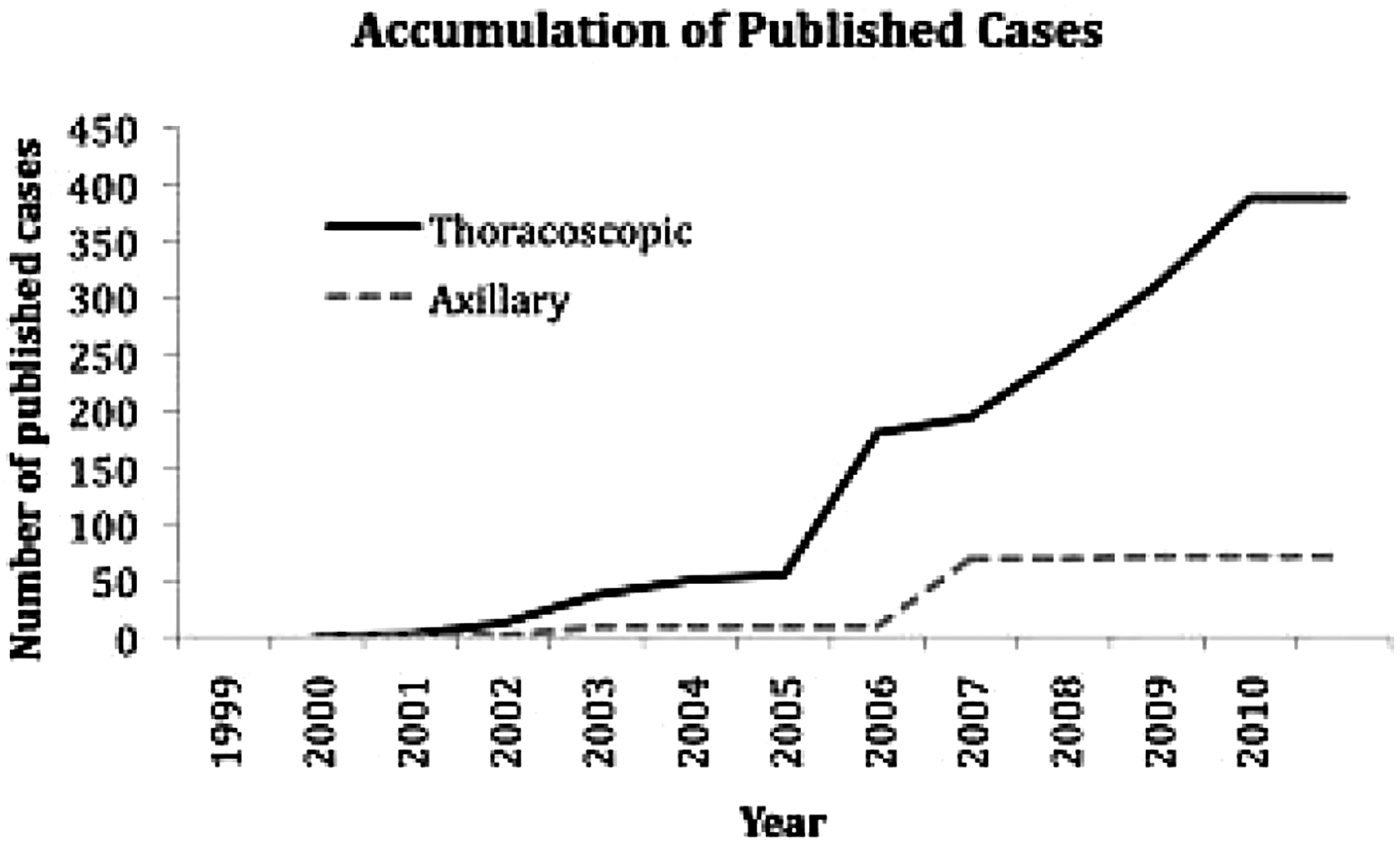
Conclusion: The axillary approach to OA repair does not appear to have been as widely or rapidly adopted as the thoracoscopic alternative. This is despite being reported earlier, having no requirement for expensive technology and there being no evidence of its cosmetic inferiority. Our series illustrates that it is a contemporary alternative to the thoracoscopic approach with the potential for cosmesis that is as good if not better (due to avoidance of multiple incisions).
Acknowledgements: The hypothesis and relevant bibliometrics have not been presented elsewhere. Clinical data was presented at BAPS2010: we acknowledge again the contributors to that study and other staff caring for these patients.
The Role of Thoracoscopy for Mediastinal Tumors in Children
Background: Mediastinal and other thoracic tumors are usually associated to moderate or severe morbidity when operated on through thoracotomy. Videothoracoscopy could bring many advantages; however, some controversies have been pointed out regarding the feasibility and oncological safety of the thoracoscopic approach, especially for malignant tumors. In adults there are many reports of thoracoscopic removal of tumors, but in children the reports are very scarce, including benign or malignant cases. The aim of the authors is to present their series of pediatric mediastinal tumors treated thoracoscopically, showing outcomes, oncological aspects, technical details and compare to previous series of open surgery in the same institutions.
Patients and Methods: From 1997–2010, 103 children (ages 2 m-18 years) with mediastinal tumors including benign and malignant cases underwent thoracoscopic treatment (group 1) in 2 institutions and had been followed up prospectively since the preoperative management. Group 2 included 72 patients operated on through thoracotomy from 1989–1996, and their data were used for comparative analysis. The diagnoses included many etiologies taking place at the anterior (AMT), medium (MMT) and posterior mediastinum (PMT), each one with individual preoperative and postoperative management. Considering thoracoscopy (group 1), the patients with AMT (n = 22) were operated on in prone position with a slight elevation of the shoulders, 3 ports. Children with MMT were operated on in lateral (n = 31) or prone position (n = 3) using 3–4 ports. Patiens with PMT (n = 47) were operated on in lateral (n = 12) or supine position (n = 35) using 3 ports. Most diagnoses were ganglioneuromas, neuroblastomas, PNET, thymus hiperplasia or timomas, different germ cell tumors, lymphangiomas and other node metastasis. Most tumors were removed through the enlarged axillary port incision. Statistics used Students, U and Wilcox tests, SPSS 17, alpha 5%.
Results: All operations except 4 could be performed thoracoscopically. The other tumors were too attached to the heart of great vessels, requiring major procedures safely done by open surgery. MMT were the more delicate and dangerous cases. Group 1 had better results than group 2 regarding ICU needs, postoperative intubation times, hospitalization time, medications, transfusion, complicated reoperation, mortality, chest wall deformity and cosmetic appearance (p < 0.0008). Only group 2 had recurrence of tumor in the incision, no implants on trocar site had been registered. Considering recurrency, group 2 had more efficacy in lymphangiomas than in group 1 (p = 0.095).
Conclusions: Thoracoscopic removal of mediastinal tumors is quite feasible and safe in children presenting most types of tumors, and seems to have less morbi-mortality than open procedures. Tumors of the medium mediastinum deserve more care to avoid conversion.
Department of Pediatric Surgery and Urology, Medical University of Wroclaw, Poland
Increasing experience in minimal access techniques and growing evidences of benefits allowed performing more complex procedures. Thoracoscopic approach seems to be a safe and effective alternative to the thoracotomy with possible avoidance of its long-term complications.
Purpose: The analysis of performed thoracoscopic repair of different types of tracheoesophageal fistula (TEF).
Material and Methods: A retrospective analysis of medical documentation and video recordings were performed. A total of fifty eight different types of TEF were closed by thoracoscopic approach during the last five years. Three 2.5–5-mm trocars were used to enter right pleural cavity with the patient lying in a prone position with the right side slightly elevated. The 5-mm 25- to 30-degree telescope was preferred. The TEF was closed by titanic clips or by ligation or both.
Results: 49 distal fistula and 2 proximal fistula were closed during esophageal atresia (EA) repair in newborns. There were 4 cases after previous EA repair where the recurrent fistula was diagnosed; however, intraoperative findings in three cases suggested rather missed proximal fistula. Only 3 cases were operated with isolated (“H” type) fistula. There were no conversion. In three cases with EA the distal fistula was closed only by ligation, all other types of fistula were closed with titanic clips, in 4 cases aided by ligation. In two cases minor tracheal air leakage from fistula site was closed with additional single suture. Previous thoracotomy in four cases didn't make any problem to achieve operative space. The postoperative course was uneventful according to TEF repair.
Conclusion: The thoracoscopic repair of TEF is effective method and based on our experience it is the procedure of choice if performed by experienced endoscopic pediatric surgeon. The previous thoracotomy is not a contraindication to thoracoscopic approach. The preoperative bronchoscopy in EA may help to identify the proximal fistula.
Lessons Learned from Endoscopic Treatment of Recurrent Tracheoesophageal Fistula
Background: Recurrent tracheo-oesophageal fistula (RTF) occurs in 5–15% of patients following oesophageal atresia repair. The repair of RTF has typically required another much more difficult surgery and with high morbidity and mortality rates. Endoscopic closure of fistula has been reported with various techniques such as tissue adhesives, electrocautery, sclerosants and laser.
Methods: A case with recurrent tracheoesophageal fistula and her challenging management is presented.
Results: An Iraqi girl with a history of an esophageal atresia repair in newbom period was admitted to our institution at 6 years of age. She had been suffering from choking while feeding and had numerous attacks of lower respiratory infections, starting from the early postoperative period. Radiological and endoscopic evaluation revealed a tiny recurrent esophageal fistula 1 cm above carina and stricture on the anastomosis line. Due to her deficient condition, balloon dilatation and endoscopic obliteration of the fistula with fibrin glue via bronchoscopy were performed. Postoperative evaluation did not show any sign of the fistula. She started feeding and had difficulty in swallowing with coughing periods. Esophageal passage was partially obstructed at the injection site on radiography and yellowish, luculent, rigid material was verified and then extirpated by esophagoscopy. Foreign body to be assumed as injection material turned up to a peanut that was eaten beyond care giyers' inormation. Further investigations showe recurrence of the formerly obligated fistula. As parents' preference, open surgery (thorcotomy and ligation of the fistula) was performed. The postoperative period and follow-up were uneventful.
Conclusions: Endoscopic obliteration of recurrent esophageal fistula may easily be applied in even patients with deficient condition. Bronchoscopy should be the way of choice for intervention to minimize risk of foreign body aspiration. Esophageal foreign bodies may cause recurrence of the fistulas in postoperative period. Further experience with appropriate technical support and large series is needed to fulfil physicians' and parents' expectations.
Troubles and Complications in MIS
Laparoscopic Surgery in Neonates: Is it Really Safe?
There have been multiple papers advocating minimally invasive surgery in neonates and infants less than 5 kg, as safe and without increased morbidity. This literature has failed to capture the three recent case reports of cardiac collapse secondary to carbon dioxide embolism (1,2,3). We present a fourth case of gas embolism in a 3.14 kg term male 3 day old neonate undergoing laparoscopy for antenatally diagnosed duodenal atresia. Under general anaesthesia, infraumbilical 6 mm Hasson and CO2 insufflation (Karl Storz Insufflator 0.5 l/min, max pressure 8 mmHg) there was immediate loss of the end tidal CO2 and pulse oximetry traces whilst the ECG demonstrated normal QRS complexes. A diagnosis of pulseless electrical activity (PEA) was made. Full cardiopulmonary resuscitation was given with 5 doses of adrenaline 10 mcg/kg and iv fluid boluses. The presumed cause of the PEA was gas embolism. Other causes of PEA were considered during the resuscitation. Spontaneous cardiac output returned after 20 minutes with normalisation of the C02 and pulse oximetry traces, and palpable peripheral pulses. The infant was successfully extubated on day 7 post event to room air with no neurological sequelae evident. A non-eventful open duodenoduodenostomy was performed with successful discharge 15 days post operatively on full feeds with no obvious neurological or cardiovascular sequelae. Four cases of cardiac collapse secondary to carbon dioxide embolism during laparoscopy in neonates are very concerning. The sequelae of clinical events in all four cases are classical and very similar. These cases highlight the possibility of this potentially lethal complication. Pathology Age Weight Entry Insufflate Return CO Kudsi Pyloric 3wks 2.5 kg VN X1 20min etal1 stenosis Taylor& Pyloric 12wks 3.6 kg Hasson X2 36min Hoffman2 stenosis Kalwani& Duodenal 1day 2.0 kg Hasson X0 20min Aliason3 atresia Our Duodenal 4days 3.12 kg Hasson X2 22min Patient atresia Table 1: Comparison of neonatal characteristics with intraoperative cardiovascular collapse during laparoscopic surgery (Age: time of surgery, Insufflate: number of insufflations prior to event, CO: cardiac output, VN: veress needle). Factors that increase the risk of gas embolism and its consequences in neonates during laparoscopic surgery include (1) Insufflation of air versus CO2 (unprimed insufflation tubing) with air having lower lethal insufflation rate/dose than CO2, (2) The smaller tolerated injected volume and pressure of CO2 introduced, (3) Foetal circulation with functionally not anatomically closed foramen ovale and ductus arteriosus, (4) Patent umbilical vein providing a direct route to the heart via the patent ductus venosus, and (5) Increased peritoneal absorption of CO2 due to greater surface area per unit weight and increased permeability. Neonatal minimally invasive surgery creates challenges requiring awareness and understanding of the unique neonatal needs. We hope to highlight these to minimize their occurrences and provide safe MIS practices.
Results
Remark: Continuous variables presented as median value.
References
Introduction: The procedure of inguinal herniorrhaphy is the most common procedure performed by pediatric surgeons today. Laparoscopy has proven to be both sensitive and specific for evaluating the contralateral inguinal region. Despite the attractiveness transinguinal laparoscopy offers and the success it has seen, we report a series of hernias after the utilization of this tool.
Methods: After IRB approval, a retrospective review of our institutions experience from 1/2002 to 6/2010 with children who underwent unilateral inguinal hernia repair with contralateral evaluation with laparoscopy was completed. Data recorded included sex, age of initial presentation, laterality of initial hernia, age at second presentation, and operative time of initial surgery.
Results: From 2002 to 2010, 1291 patients underwent unilateral inguinal hernia repair with negative laparoscopic evaluation of the opposite ring. There were 30 patients (2%) who subsequently presented with an inguinal hernia on the contralateral side. All were male. The average age of initial presentation was 41.2 months. The mean time to occurrence of the contralateral hernia was found to be 16.9 months with a median of 12.2 months. The mean operative time for the initial operation was found to be 23.9 minutes.
Conclusions: When using laparoscopy to explore the contralateral inguinal region, the surgeon should be aware that a negative exam may still be associated with a small chance of clinically developing a hernia.
Thoracoscopic Versus Open Repair of Tracheo-Esophageal Fistula: A Matched Comparison of Morbidity and Mortality
Background: Recent technical advances have allowed minimal access repairs of complex congenital malformations in neonates. Thoracoscopic repair of tracheo-esophageal fistulae (TEF) has been reported and is regarded to be superior to conventional repair via thoracotomy due to smaller incisions, thereby lowering the demand for post-operative analgesia in the short term and fewer musculoskeletal deformities in the long-term. However, there is little literature available comparing the morbidity and mortality between the two TEF-repair techniques.
Objective: To compare the morbidity and mortality associated with thoracoscopic versus open TEF repair in a matched study design.
Patients and Methods: Between July 1999 and June 2009, 166 TEF-repairs were performed at our institution, of which 12 were thoracoscopic repairs. These 12 patients were matched to 12 open repairs based on gestational age (GA) and birth weight (BW). Maximum matching discrepancy of 12% was tolerated. Descriptive statistics and paired univariate analysis (Wilcoxon Rank Sum test, McNemar test) were performed using SAS 9.2. Two-sided p-values were applied.
Results: The patients' GA ranged from 35 to 41 weeks and BW from 2240 g to 4390 g. Baseline characteristics were similar between the two groups including VACTERL-associated malformations, TEF type and age at repair (Table 1). Leaks occurred equally among the matched pairs, while post-repair esophageal strictures were more common with thoracoscopic repairs (p = 0.06). No difference between the two groups was found for time to establishment of full oral feeds, length of hospital stay and number of hospitalizations during the first five years of life. Long-term morbidities were similar between the matched pairs. There was no mortality in either group and the patients were followed for 519 days in the thoracoscopic and 942 days in the conventional repair group (p = 0.0161).
Conclusions: Thoracoscopic TEF-repair was comparable in post-operative outcomes to conventionally repaired TEF in our matched cohort study. Future, larger studies are required to determine the basis for more frequent strictures following thoracoscopic TEF-repair, which may reflect our learning curve.
A Particular Cholecystectomy
A 9-year-old boy suffering from sickle cell anemia and presenting gallstones, was send to our surgical department for cholecystectomy. There was no clinical history of cholecystitis. Laparoscopic cholecystectomy was performed. There were multiple adhesions between gallbladder and liver and, during the procedure, the gallbladder was perforated. Bile was aspirated, antibiotics (cephalosporins) were continued and a small drain was left in place for 48 hours. Postoperative course was uneventful and child left hospital on the fourth postoperative day. Four days later he was admitted for abdominal pain and vomiting. Lab values showed infection (CRP = 10.4 mg/dl), sonogram and CT scan were showing a small amount of ascitis and some bile around the liver hilum. Antibiotics were started but were not improving the patients condition and finally he was reoperated. Bile was found between liver and stomach, it was aspirated, abdomen was rinsed and drained. Postoperatively the patient improved rapidly, oral feeds were introduced and well tolerated but abdominal drainage increased and became yellowish. A leak on the biliary tree was suspected and confirmed on sonogram and MRI. Retrograde cholangiowirsungography was performed, showing a section of a right lateral hepatic bile duct with low implantation in the choledocus. Cystic duct was originating from this ectopic right lateral duct. Endoscopic cystoduodenostomy using a double pigtail prosthesis was performed successfully. Follow-up now is one month and child is doing well.
Conclusion: We usually perform a preoperative sonogram but no contrast study before cholecystectomy in children. There was no documented cholecystitis in this case but the chronical jaundice due to sickle cell anemia may have masked some episodes of cholecystitis. Acute or chronic cholecystitis in association with a biliary tree anomaly is at high risk of peroperative biliary tree injury. We changed our protocole: in children with a history or suspicion of acute or chronic cholecystitis we perform magnetic resonance cholangio-pancreatography (MRCP) before laparoscopic cholecystectomy.
Is Fascial Closure Necessary to Prevent Trocar-Site Hernias in Pediatric Laparoscopy? Experience of a Single Pediatric Institution in Colombia
Background: Minimal access surgery is becoming the surgical approach of choice for a variety of surgical disorders in the pediatric population. It has been recognized that although incision hernias are less common after laparoscopy vs. open surgery, there is still a risk described in a few series. The incidence reported for adults is 0.1–3% and for children and adolescents there is a 0.3% of incidence. Actually there is no consensus in children and adolescents regarding the closure of fascial defects in 5 mm trocar sites. Some authors have stated their opinion that all 5 mm ports sites might not be necessary to close, but in active manipulation during prolonged procedures, to avoid complications they should be closed. We present our experience with port site incisional hernias following laparoscopy using hybrid devices, 3, 5, and 10 mm trocars; closing fascia only in umbilical incisions and in any lateral incision for 10 mm trocars.
Methods: The medical records of all children who underwent laparoscopy at the Fundación HOMI in a 33-month period (November 1, 2007 through August 31, 2010) were reviewed. A total of 159 cases were identified, the follow-up ranged from 1 week to 30 months. Data obtained included diagnosis, procedures, demographics, number and size of port sites, type of closure, complications, and hospital stay periods.
Results: Median patient age was 11 years (range 0.06–17). Of the 335 identified port sites, 68 were 10 mm torcars, 199 were 5 mm torcars, 25 were 3 mm trocars, and 43 where hybrid ports. All of the umbilical incisions were done with the Hasson's technique and underwent fascial closure with polyglactin 910. Closure didn't include peritoneum, and air was deflated completely before port removal. Other than umbilical sites were done under laparoscopic direct vision and didn't get fascial closure.
One hernia (0.29%) was diagnosed at the fourth postoperative day in an umbilical 10 mm port site that had done fascial closure. The patient presented dehiscence of the whole abdominal wall with protrusion of omentum. We found that 5 mm port sites without fascial closure did not present incisional hernia. Also we didn't find any relationship regarding age and incisional hernia. 5 mm port sites were not closed in any of the off-umbilical insertion even in extensive manipulation and prolonged operating times.
Conclusions: The incidence of port site hernia after laparoscopy in our study was 0.29%, which is similar to that reported by the study published by Chen in 1996. The literature shows very few reports of this complication. The only case that presented hernia was a patient with risk factors for inadequate wound closure including hepathopaty and malnourishment. Further studies must be conducted regarding the relationship between the nutritional state of the individual, age and the closure of fascia with the development of hernias. Also, we considered important to determine in other studies if by not closing the fascia there is a significant change in the pain experienced, the economic costs and the surgical time spent.
Urology
Anderson-Hynes Pyeloplasty in Infants Below 20 kg: Laparoscopic or Open Surgery?
Abstract Withdrawn
Laparoscopy in Impalpable Testes: Comparison of Single-Stage Versus Two-Stage Orchidopexy
Purpose: To compare the results of the classic two-stage orchidopexy described by Fowler-Stephens with a testicular vessel-sparing single-stage approach in the management of intraabdominal testes we retrospectively analyzed our data.
Materials and Methods: From January 2005 to September 2010 53 patients (mean age 32 months, range 5–186) underwent laparoscopy for impalpable testes. In case of a viable gonad, laparoscopic orchidopexy was performed either in a two-stage procedure including ligation of the vessels as a first step or as a single-stage procedure without ligation of the testicular vessels. The results of both approaches were evaluated by assessment of testicular survival using ultrasonography.
Results: A total number of 62 testes were included in the study, of which 54 were located intra-abdominally; single-stage orchidopexy was performed in 29 testes whereas a two-stage approach was conducted in 14 testes. 11 gonads had to be removed due to atrophy and in 8 cases non testis was found at all. During a mean follow-up of 17 months (range: 1 to 48 months) none of the 29 testes treated by single-stage orchidopexy atrophied. By contrast, atrophy and reascent occurred in 1 of 14 after two-stage procedure.
Conclusion: Considering our excellent experiences with single-stage management, we conclude that the single-stage approach is a reliable, save and efficacious in the treatment modality of intraabdominal testes. We suggest that the two-stage procedure including testicular vessel ligation should be restricted to high abdominal testes with very short vessels.
Improving Outcome with Gubernacular Sparing Laparoscopic-Assisted Fowler Stephens Orchidopexy
Aim: To demonstrate the technique of successful testicular salvage in patients having a gubernacular sparing, laparoscopic-assisted, Fowler Stephen's procedure.
Methods: A prospective study over a 5 years of a single surgeon's experience within a tertiary paediatric surgical unit is reported. All cases of impalpable testes subjected to laparoscopy were recorded in a standard computer spreadsheet. Patient demographic details, operative findings, details of intervention and outcome were documented.
Results: Thirty four cases of impalpable testes of median age (at initial intervention) of 1.49 years, range 0.81–9 years, were managed over the period of study. Nineteen testes were absent/vanishing (7 left, 9 right, 3 unstated) and the rest were intra-abdominal. Of the latter group of 15 cases, two were bilateral, resulting in a total of 17 orchidopexies. One of these cases had both testes located above the pelvic brim. The rest of the testes were well proximal to the internal ring and subjected to staged Fowler Stephens ochidopexy.
Apart from a single patient who suffered small bowel injury and who was kept overnight all other patients were managed as day cases for all of the admissions.
All patients (15) had successful surgery with testes (17) palpable within the scrotum at post operative assessment at 3 and 6 months. Mean follow-up was 601 days, (SD 476).
A single case of an intra-abdominal left testes with absent ipsilateral vas and kidney underwent successful staged procedure notwithstanding division of the spermatic vessels.
One patient with Rubinstein Taybi Syndrome who underwent a previous fundoplication and PEG placement suffered small bowel injury which was repaired instantly.
Conclusion: The initial results from a staged Fowler Stephen's procedure with laparoscopic assistance of second stage are encouraging. Despite being more invasive than a total laparoscopic approach, preservation of the gubernacular supply without acute angulation ensures comprehensive success.
The Impact of the New Hemostatic Devices in Pediatric Patients Underwent Total or Partial Retroperitoneoscopic Nephrectomy
Background: Scanty reports exist in literature regarding the use of new hemostatic devices to perform renal ablative surgery in pediatric population. The aim of our study is to review a series of total and partial nephrectomies performed in the last 5 years in our Institutions.
Materials and Methods: Patients with benign lesions who underwent retroperitoneoscopic nephrectomy and partial nephrectomy at our institution in the period 2005–2010 were retrospectively analyzed in the study. Twenty-two procedures were performed, 20 patients underwent nephrectomy (12 girls; 8 boys) and 2 other girls that presented a duplex system with a non functioning upper pole underwent a retroperiotoneoscopic nephro-ureterectomy. To easily analyze the data of the 20 patients underwent nephrectomy, they were divided in 2 groups: group 1 (G 1) pts-1–10, in who we performed the procedure using monopolar coagulation and group 2 (G 2) pts 11–20 in who we used new hemostatic devices (starion®, ligasure®, ultracision®). The results of the 2 partial nephrectomies were analyzed separately.
Results: No conversions were reported in our series. We mainly analyze 6 parameters to compare the results: Operative time (OT), estimated blood loss (EBL), need of transfusion (NT), complications, time to oral intake (TOI), and hospital Stay (HS). OT in G1 was variable between 50–130 minutes (median 85 minutes) in G2 45–100 minutes (median 65 minutes); EBL was about 15 ml for G1 and about 5 ml for G2, NT was not necessary in both groups, in G1 we had 2 complications due to a small bleeding during dissection only 1 complication in G2 due to an instrument failure; TOI was day 1 for both groups; median HS was 3 days for both groups. As for heminephrectomy OT was 120 and 140 min, EBL about 30 ml in both, NT not necessary, TOI was 1 day and HS 4 and 5 days, respectively. For heminephrectomy no complications were recorded.
Conclusions: Our study confirmed the feasibility and safety of nephrectomy and partial nephrectomy in pediatric patients using retroperitoneoscopy. The use of new hemostatic devices reduces signifincantly OT and EBL. These devices seem to be essential to perform partial nephrectomy via retroperitoneoscopy.
However, a randomised controlled study on larger series of partial nephrectomy is strongly suggested to confirm our preliminary experience.
Retroperitoneal Laparoscopic Pyeloplasty with Uretropelvic Junction Obstruction in Children: Technique and Initial Outcomes
Aims: We present the technique of retroperitoneal laparoscopic pyeloplasty with ureteropelvic junction obstruction (UPJO) and the inital results.
Methods: Form 1/2009 to 6/2010, a total of 36 patients was left hydronephrosis due to ureteropelvic junction obstruction who underwent retroperitoneal laparoscopic pyeloplasty. There were 29 males, 7 females and mean age was 3.5 years old (range 3months to 14 years old).
Outcome measures consisted of operative time, hospitalization stay, complications. All the patients were followed up with ultrasonography and intravenous pyelography 3 months and then every 6 months after procedure.
Results: Average operative time was 65 mins (range 45 min to 135 min) and mean hospital stay was 2.5 days (range 2 to 4 days). No complication was noted neither intraoperation nor postperation. Perirenal drainage was removed 2 days after surgery and the stent JJ was removed 3 weeks after surgery. All patients were evaluated 3 months postoperatively for an ultrasonography and intravenous pyelography, which revealed no evidence of obstruction in any of the patients.
Conclusion: The study suggests that retroperitoneal laparoscopic pyeloplasty is feasible, effective in children with good results.
A Retrospective Review of the Outcome of Laparoscopic 2-Stage Fowler-Stephens Procedures Over a 6 Year Period
Introduction: A total of 164 laparoscopies for the investigation and treatment of 139 impalpable testes were performed in our unit over a six year period.
Methods: Patients were identified through our operating register, and then a retrospective review of the patient journals of those who had undergone a Fowler Stephens two stage orchidopexy was performed.
Nineteen patients had bilateral impalpable testes. Twenty-three testes had confirmed vanishing testes, where the vas and vessels ended blindly. Thirty-two testicular remnants were removed from the inguinal canal or scrotum during groin exploration. Open orchidopexy was performed in forty-two testes and a two-stage procedure with division of the vessels was performed (Fowler-Stephens) in forty-one testes if the testis could not be drawn over to the contralateral inguinal ring during laparoscopy.
Results: Thirty-six patients underwent a two-stage Fowler-Stephen's procedure of whom 5 underwent a bilateral laparoscopic procedure. Follow-up was a minimum of 6 months. One patient has been lost to follow-up and one testis was removed at the second procedure as the vas was too short to reach the scrotum. Overall survival of the testis was 82% (32 of 39 testes). 2 of the 3 testes in patients 10 years and older did not survive.
Of those who underwent open orchidopexy, one testicle had atrophied, 7 were small but within the scrotum and 23 were of normal size and within the scrotum. 2 were electively left in the groin and 5 have been lost to follow-up.
Conclusions: Testis survival after a two-stage Fowler-Stephens procedure is acceptable. Testicular survival when the boy reaches the age of 10 is much lower in our group. Education of colleagues about early referral of this group of boys is clearly important.
Seminal Vesicle Cyst with Ipsilateral Renal Agenesis: Laparoscopic Approach—2 Cases
Seminal vesicle cyst with ipsilateral renal agenesis is a rare malformation. We report 2 cases: the first one was diagnosed antenatally and operated at one year of age;the second case became symptomatic and was operated at puberty;the preoperative work-up included ulrasonography, MRI, CT scan. The transperitonael access allowed a good exposure of the entire malformation, an easy dissection deep in the pelvis with preservation of the controlateral spermatic tract. The surgical technique will be illustrated by a video. These 2 cases underlines that embryology may explain the prevalence of ipsilateral genital abnormalities in patients with a single funtional kidney.
Transperitoneal Laparoscopic Dismembered Pyeloplasty in Infants
Background: In the last fifteen years since laparoscopic pyeloplasty was first described, there has been an increase in minimally invasive pyeloplasty for treatment of PUJ obstruction. Many advocate the retroperitoneoscopic approach, which can provide an easier dissection, but due to lack of space this is very difficult in smaller children. By contrast, the transperitoneal laparoscopic approach, while providing increased operating space, carries a potential risk of intra-abdominal injury or ileus. For the past year we have been performing Transperitoneal Laparoscopic Dismembered Pyeloplasty in infants weighing less than 10 kg.
Methods: A retrospective review was carried out of all patients undergoing Transperitoneal Laparoscopic Dismembered Pyeloplasty at a single centre between August 2009 and August 2010. Data was collected from locally held electronic databases. Only patients weighing 10 kg or less at time of surgery were included.
Results: 7 cases were identified. 5 (71.4%) had antenatally diagnosed hydronephrosis. 4 (57.1%) had a left sided procedure. At time of surgery median age (IQR) was 9 months (5.5–10.5) and mean weight (SD) was 8.53 kg (1.78). Median (IQR) operative time was 145 mins (135–147.5) and median (IQR) post-operative stay was 2 days (2–3). Mean (SD) pre-operative renal pelvic dilatation on ultrasound scan was 23 mm (5.6) and mean (SD) pre-operative function on MAG3 renogram was 45.1% (13.2) and drainage curves were all obstructed. Post-operative renal tract ultrasound scan performed at a median (IQR) of 4 months (4–4.25) post-op revealed an improvement in renal pelvic dilatation of a mean (SD) of 54.4% (23.6). At present, complete follow-up is available for 3 (42.9%) cases, all of whom have had improved drainage demonstrated with MAG3 renogram performed at 7 months following surgery.
Conclusions: Transperitoneal Laparoscopic Dismembered Pyeloplasty seems to be a safe and effective operation in infants weighing less than 10 kg, resulting in improved renal pelvic dilatation and drainage.
Laparoscopy for Treatment of Nephroblastoma
Aim: To assess the effectiveness of laparascopic nephrureterectomy in the combined treatment of Wilms' tumor in children up to 1 year old.
Methods: in 2008 23 laparoscopic procedures for kidney diseases were performed in gthe Russian Research Institute for Children Oncology and Gematology. We analysed 17 minimally invasive procedures in children up to 1 year old with nephroblastoma. All the surgical procedures were performed with patients placed in a lateral position. We used balanced multicomponent endotracheal anaesthesia combined with epidural analgesia. Average duration of the procedure was 62 minutes (maximum, 130 minutes; minimum, 40 minutes). The blood loss on average was not more than 30 ml. Most of the procedure (mobilization of the colon, vessel separation, lymphadenectomy and kidney removal) was performed by the harmonic scalpel ultracision. The incision to evacuate the deleted kidney was made in the iliac area in the same place where the port had been installed and did not exceed 5 sm. All the children were extubated on the surgical table. Post-operational anesthesia was secured by constant epidural infusion of 1% ledocain during 1 day. No complications revealed in the post-operational period. All the patients stayed in the resuscitation department not more than one day. When needed, the polichemotherapy started not later than on the 8th day. In all the cases the post-operational period lasted without complications, the drainage tube was removed on the 1st day after the procedure.
Conclusion: an early age of a child is not a limitation for the laparoscopic nephrureterectomy given that the size of the tumor is? comparable with the size of a child. Minimally invasive procedures for malignant tumors in kidneys are possible in children from the first months of their life with all the oncological principles respected. The application of laparoscopic techniques leads to the reduction of the recovery period and has good cosmetic effect.
Is it Necessary to Close the Deep Inguinal Ring During Laparoscopic Orchidopexy?
Abstract: During laparoscopic orchidopexy (LO) closing the peritoneum over the area of the deep inguinal ring (DIR) is a routine step of the procedure for many authors. However, we do LO with a modification of not closing the DIR. We postulated that this step is not necessary. We report our experience and focus on this technique.
Material and Methods: This is a retrospective chart review, including hospital charts and office records, for patients who underwent laparoscopy for impalpable testes between May 2004 and May 2010.
Results: Four hundreds and forty-two boys had laparoscopy for 570 impalpable testes during the study period. Sixty-two (14%) were on the right side, 252 (57%) on the left and 128 (29%) were bilateral. During laparoscopy; the testis was “vanishing” or “atrophic” in 182 (32%), “peeping” in 74 (13%), within 3 cm from the DIR in 251 (44%) and more than 3 cm from the DIR in 63 (11%). The testes passed through the anatomical DIR in 198 (51%), and through a new deep ring in 190 (49%); medial to the inferior epigastric vessels (lateral umbilical fold) in 148 (78%) and medial to the medial umbilical fold (Prentiss maneuver) in 42 (22%). The peritoneum over the DIR was closed in 178 (46%) and left without closure in 210 (54%). Only one case developed groin hernia in the 1st postoperative day and on surgery, the defect was medial to; but not thorough, the DIR (Port-site hernia). On the follow-up (range 3–34 months) no hernia developed in any of the cases.
Conclusion: Closing the peritoneum over the area of the DIR is unnecessary during LO. However, a prospective controlled study is still needed.
Laparoscopic Varix Ligation in Children: How to Avoid Complications
Introduction: Complications usually associated with laparoscopic varicocelectomy techniques include varicocele persistence or recurrence (especially characteristic for artery-saving methods), hydrocele formation (typical for Palomo-type simple ligation of the whole vascular bundle) and bleeding.
The overall experience of about 2500 different laparoscopic procedures performed for varicocele in children during the 17 years period helped us to work out the method that provides the possibility to avoid these problems.
Materials and Methods: More than 1500 pediatric patients aged from 6 to 17 years underwent standard laparoscopic procedure during the period from 1996 to 2010.
The important pearls of our method are the following:
Modified open approach with initial insertion of the 5 mm blunt trocar eliminates the possibility of puncture complications; two additional 2–3 mm trocars used for dissection, ligation and suturing make the operation really minimally invasive and cosmetic; Thorough examination of the inguinal region with visualization of all retroperitoneal vascular structures passing through the internal ring. In order to prevent persistence and recurrence all these vessels have to be ligated (main vascular cord) or coagulated (additional thin veins). We do not dissect separately every vein branch that we intend to transect, because in this situation one can easily miss thin vein in this region and leave it not ligated. We prefer to ligate the whole vascular bundle with the exception of the isolated structures that we want to preserve; We do not preserve the artery because artery-saving methods have proved to show major recurrence and persistence rate. At the same time postoperative Doppler examination revealed no significant difference in testis blood circulation in artery-saving and other groups of the patients. Thorough dissection and preservation of 4–8 lymphatic vessels is obligatory to prevent hydrocele formation. Using of the traction ligature facilitates all stages of dissection and inspection, especially lymphatic vessels isolation. Double ligation of the vascular cord without transecting is a safe and reliable method excluding even the possibility of postoperative bleeding.
Results: The suggested technical modification of the procedure used in the large group of 1500 pediatric patients had proved to be safe, easy, universal and effective:
No cases of conversion; No cases of persistence or relapse of varicocele; No cases of hydrocele formation; No cases of postoperative bleeding; No cases of testicular atrophy.
Conclusion: Nowadays we do not know exactly which pediatric patient with varicocele have to be operated on;
If we decide to operate, the described laparoscopic surgical method provides excellent functional and cosmetic results eliminating the very possibility of the most common postoperative complications.
Laparoscopic Management of Intraabdominal Testis: Is a Two-Stage Procedure Really Necessary?
Aims: The role of laparoscopy in the management of intraabdominal testis (IAT) is well established. Orchidopexy usually involves a 2-stage Fowler Stephens procedure, with division of the testicular vessels in the first stage. We describe our experience of managing IAT, using a single-stage laparoscopic orchidopexy where the vessels are not divided, preserving the normal testicular vasculature.
Methods: We reviewed patients who had laparoscopy for impalpable testis under the care of a single surgeon between 1997 and 2009. 21 patients with a diagnosis of IAT were identified. Their case notes were reviewed for clinical data, type of procedure, complications, outcome and follow-up.
Results: Age ranged from 1 to 12 years (median 3 years). In 2 patients IAT was bilateral, so a total of 23 testes were operated on. In 17, the testis lay sufficiently close to the inguinal ring to allow a single-stage procedure to be performed. This involved dividing the gubernaculum, then mobilizing the testis by dissecting it from its peritoneal covering. The testicular vessels were preserved in 14 cases by opening the peritoneum laterally to the vessels and dissecting in a retroperitoneal plane. The vessels were divided in the remaining three. Following mobilization, the testis was brought down into the scrotum via the inguinal canal and fixed with sutures in a Dartos pouch (created via a scrotal incision). The deep inguinal ring was closed with a purse string suture. Five IAT were considered unsuitable for single-stage orchidopexy following laparoscopic assessment as the testis lay too far from the inguinal ring. They underwent a two-stage Fowler-Stephens orchidopexy. One orchidectomy was performed: the testis was fused to the liver, so orchidopexy was not feasible. No post operative complications occurred. At follow-up, atrophy rate in the single-stage group was 1 in 17 (5.8%). One patient in the two-stage group was lost to follow-up. Of the remaining four, there was one case of testicular atrophy.
Conclusions: IAT can be managed safely with a single stage laparoscopic procedure, avoiding the division of the testicular vessels. Clearly there are benefits to the patient as they do not require a second procedure. We postulate that retaining the normal vascular supply may improve the long-term spermatic and hormonal function of the testis. The position of the IAT must be taken into account, as those which lie a significant distance from the internal ring cannot be mobilized sufficiently to bring it into the scrotum. However, in appropriately selected cases, the outcome is good and the atrophy rate is low.
Diagnosis and Management of Urinary Bladder Stones in Children Under 5 Years in Rural Setting
Methods and Materials: Bladder stones were diagnosed in 4 children under 5 years at Jahun And Kazaure General Hospitals, Jigawa State, Nigeria, from 2006 to 2010. There ages were 23, 35, 46 and 52 months, respectively. The mean age was 39 months. The bladder stones were revealed following convectional plain abdominal radiography in the 4 cases. Bladder stones were removed via transvesical approach.
Results. One child presented with signs and symptoms of upper tract urinary infection (UTI). The remaining 3 were admitted with urinary retention, two among them were circumcised. In 3 patients the radiologic features of the stones were not specific. Intravenous urography was done to detect a residual stone in one case and this led to second surgery to clear the stone. There was operative wound breakage in two cases resulting from urethral catheter blockage. Hospital stay ranges from 7–14 days.
Conclusion. Convectional plain abdominal radiology was enough for prompt diagnosis of bladder stones and treatment.
Endoscopic Treatment of Pediatic Urolithiasis—Own Experience
Children in Europe and in USA represent about 1–3% of all patients with urolithiasis. Treatment is aimed at achieving high cure rates with minimally invasive approaches and no stone material left behind. At an increasing number of centers URS is being performed in cases that previously would have been treated with SWL or PCNL [3]. We report our experience with treatment of urolithiasis in pediatric population.
A retrospective evaluation of a prospectively maintained database of pediatric patients with urolithiasis was reviewed at Warsaw Hospital for Children between February 1, 2006 and July 31, 2010 with renal or ureteral calculi. Patient charts were reviewed for sex, age, prior history of stone disease, stone size and location. An ultrasound examination of the urinary tract was performed in all patients and in selected case X-ray, intravenous urography (IVU), retrograde pyelography. Operative reports were reviewed to determine type of surgery procedure and intra-operative complications.
During this 4.5-year period time 80 patients with urolithiasis required surgical procedure. 87 ureteroscpies were performed. 66 patients were qualified for URSL as a first line treatment or after extracorporeal shock wave lithotripsy. Ho:YAG pulsed laser, ultrasonic and pneumatic lithotripters with rigid and flexible ureteroscopes 4.5/6Ch and 6.5/8 Ch were used, under general anaesthesia, in operating theatre conditions. We did not use balloon dilatation or presenting. In our practice hydrodilatation appeared as an effective method. Leaving a stent in ureter is not a standard procedure and it was done only if there was a suspicion of injury. URSL was performed on 60 children out of 66 qualified. In one patient with arthrogriposis entering ureter was impossible because of anatomical malformations. Retrograde access could not be obtained in 5 of the children. Despite dilating ureter orifice ureteroscope cannot easily be advanced, so these children were qualified for operative treatment. A very good result was obtained in 53 patients (88.3%). The stones were removed completely or crushed into small pieces so that self-evacuation could take place, which was later on confirmed by the USG examination. In 8 cases (13.3%) second URSL procedure was required. In two cases complications occurred: ureter perforation and stricture of the ureter. Extraction of the stone during laparoscopic pyeloplasty was performed in 12 patients with staghorn calculi. In 9 cases to avoid nephrolithotomy ureteroscope with ultrasonic lithotryptor was used. Calculi was crushed by ultrasonic lithotryptor and rinsed from the calyx. No intraoperative or delayed postoperative complications were observed. 100% of mentioned patients were stone free. One patient underwent open surgery because of ureteropelvic junction obstruction and in remaining 2 patients no lithotryptors were used. We also performed one PCNL and two cystolithotripsy procedures because of big bladder calculi.
Our experience shows that URSL can be efficiently and safely employed in pediatric ureterolithiasis treatment. This method enables to cure a patient faster as well as reduce the pain. What is more endoscopic equipment can be also efficiently used in open surgery procedure for patients with staghorn calculi to avoid nephrolithotomy and to make this procedure save and effective.
Endoscopic Intraureteric Positive Charged Dextranomer Sephadex Copolymer Injection to Treat High Grade VUR in Ectopic Ureters
Purpose: The treatment of high grade VUR using endoscopic injection with biocompatible and biodegradable microparticles has given various success rates. We conducted a study to determine the efficacy of an recently marketing positive charged bulking agent (Positive charged Dextranomer/HA sephadex–Urodex) for the endoscopic treatment of high grade reflux in ectopic ureters.
Material and Methods: From December 2004 to October 2006, 12 children (13 ectopic ureters) were treated for high grade reflux endoscopically; 13 ureters with grade IV and V reflux received a single intraureteric injection with Urodex. The mean (range) age was 30 (9–121) months. The procedure was performed on an out-patient basis. The follow-up assessment consisted of a voiding cysto-urethrogram at 3.9 and 18 months after the injection.
Results: At 3-months follow-up 8 of 13 refluxing ureters (61.5%) were cured using Urodex whereas one year after injection success rates slightly decreased to 46.1%. This decrease may be attributed to re-reflux in two grade V cases. Also in 3 cases reflux downgraded while in 2 cases no changes in reflux grading.
Conclusions: Single intraureteric endoscopic injection with Urodex was found effective to prevent reflux into the ectopic systems. This finding may be attributed to the positive charged particles in Dx/HA. But long-term results and larger series are necessary to conclude overall success.
Abstract Author Index
Abrantes, Jessica I, P012
Adams, Steven, P127
Adayanthaya, Kishore, P014
Adibe, Obina O, S018
Aguayo, Pablo, S018
Aidlen, Jeremy T, P010, P044
Al Adhm, Khalid, P066
Albertal, Mariano, P094
Alessandra, Farina, P128, S045
Alessandro, Settimi, P128, S045
Alhasov, Abdumanap, P101, S022
Alieva, Elmira I, S072
Almström, Markus, P022, P042, P081
Alzahem, Abdulrahman, S059
Annamaria, Staiano, S045
Anselmo, Dean M, S040, S048, S054, V014, V015
Antczak, Anna, P118
Antonella, Centonze, P128
Antonio, Savanelli, P128, S045
Aoki, Tatsuya, P096
Arda, Surhan, P069, P115
Ariturk, Ender, P023
Arnold, Marion, P005
Arthur, L. Greer, P035
Arthur, L. Grier, S043
Ashraf, Junaid, P127
Atabek, Cuneyt, P119, P139
Ates, Ufuk, P030, P031
Attia, Mohamed A, P056
Avery, Nicole, P120
Azam, Sarwar, P006
Babayigit-Akpinar, Halise, P030
Babu, Narendra, P065, P112
Baerg, Joanne, S058
Baez, Julio J, P107
Baglaj, Maciej, P118
Bahadir, Berktug, P031
Bahador, Ali, P019
Bailez, M, S014, V007
Banani, S. Abbas, P019
Barker, Gillian, P130
Bataineh, Ziad, P091
Bax, N, P039
Becmeur, François, P100, S023
Bellia, Gaston, P094, S046
Beltran, Jorge R, P087, P089, P124
Benchimol, D, P001
Bernay, Ferit, P023
Betalli, Pietro, S070
Bezuidenhout, Lorraine, P004
Bhatia, Amina, S051
Bi, Yunli, S028, S032
Bicakci, Unal, P023
Bignon, Horacio, S046, S058
Blanco, Angel, P049, P106
Blatnik, Jeffrey A, S008
Boemers, T., P086
Böhm, Roland, P084, S056
Bortagaray, Juan Ignacio I, V008
Bouzidi, M., P086
Bradnock, TJ, S021, S066, P047
Branström, Gustav, P130
Breaud, Jean, P001, P029, P131
Broadis, E, P047, S021
Broto, J, P038
Brownlee, EM, P132
Buadze, Merab, P045
Buela, Enrique, S046
Bühligen, Ulf, P084, S056
Burek, Carol, V008
Burgos, Carmen Mesas, P081
Burnand, K, P136
Buyukunal, Cenk, S025, S030
Cabral, S, S014, V007
Calcagno-Silva, Marcelo, S074
Caliskan, Bahadir, P119, P139
Calkins, Casey M, S058
Calvo, Andres I, P107
Camby, C, P009
Campbell, Brendan T, P012
Cañon, Isabel C, P087, P089, P124
Caponcelli, Enrica, P062, S050
Carneiro, Siderley S, P050
Carr, Stephen R, S057
Carretero, Sara Fuentes, P110
Carvajal-Figueroa, Lourdes, S044
Carvalho, Lercion A, P117
Casadiego, Giovanny, P122
Castañeda, Sergio D, P124
Castle, Shannon L, S040
Chagas, Celio C, S074
Chagelishvili, Zaza, P045
Chalmers, David, S029
Chamond, Olivier, P033, P036
Chan, Ivy, P073
Chan, Kwong-leung, P073
Chandler, Nicole M, S039, V005
Chandrasoma, Parakrama T, P051
Chang, Yu-Tang, P020, P063
Chen, Wei-bing, P024
Chevallier, D, P001
Chiesa, P Lelli, P043
Chitnis, Milind, S061
Chiu, Priscilla P.L., P122
Chiu, Wen-Chun, P063
Cho, Min Jeng, P057
Chong, Albert, P076
Christison-Lagay, Emily R, S024
Chua, J, P070
Ciftci, Mehmet, P115
Cifuentes, Luis E, P064, S052
Cina, Robert, P113
Ciro, Esposito, P128, S045
Ciullo, Sean, P044
Clarke, Simon, P048
Clifton, Matthew, S051
Cohen, C, P001
Concetta, De luca, S045
Cone, Lois, P068
Corbetta, Juan P, V008
Corouge, P., P108
Correia-Pinto, Jorge, P060, S036
Courel, Jose, P107
Cueva-Carrillo, Judith, S044, V011
Cui, Qingbo, P032
Curbelo, M, P038
Curry, Joe, P059
Czauderna, Piotr, P090
D'Alessio, David, S063
Danielson, Paul D, S039, V005
Dassonville, M., P123
Davenport, Katherine P, S034
Davis, C, S066
De Armas, Ismael Salas, P017
de Armas, Ismael Salas, S049
de Barros Carvalho, Carlos Leite, S046
De Napoli, S, P009
De Vogelaere, Kristel, P085
DeBakey, Michael E., P008
DeFoor, William R, P068
Demirbag, Suzi, P119, P139
Dereli, Dilsad Demet, P069
Desantis, Marie Angela, P131
Devière, J., P123
Dharia, Bela, S024
Dharni, Herjyot, P048
Dhayagude, Snehalata, P014
Diao, Mei, S011
Diaz, David, P087, P089, P124
Diaz, Maria Lopez, P110
Diaz-Cristerna, Agustin, S044
Dick, A, S021
Diefenbach, Karen A, P016
Dingemann, Jens, S013
DiSomma, Nerina, P093
Dokumcu, Zafer, P119
Dolan, Lawrence, S063
Dominguez, Guillermo, S046
Donskoy, Dmitriy, P080
Dorobisz-Zaleska, Urszula, P118
Downey, Earl C, V001
Duersch, Markus, P104, S009
Duke, Duane S, P035
Duncan, Charles, P016
Dung, Le Anh, P129, S010
Duran, Victor, V008
Duthie, G, S066
Dyakov, Valentin, P002
Effat, AM, P053
El Attar, Ashraf A, P056
El-Debeiky, Mohamed S, P046
Elias, Eugenia, S046
Elicevik, Mehmet, S025, S030
Elkholi, Nour, P134
Elmo, Gaston, P109
Elsen, Mie, S061
El-Shafei, Hossam, P046
El-Shafei, Ihab A, P046
Emami, Claudia, S040, S048, S054
Emir, Haluk, S025, S030
Engelmann, Carsten, S013
England, Richard J, P004
Erasmo, Miele, S045
Erazo, Ricardo, P106
Esteves, Edward, P018, P050, P117, S074
Fasching, Günter, P037
Faubion, William, S038
Fedorova, Elena V, P135, S047
Fedorova, Lyudmila, P002
Felekouras, Evaggelos, S005
Ferreira, Aníbal, S036
Ferreira, Cindy Gomes, P100, S023
Ferro, Marcelo Martinez, S058
Fierro, Fernando, P087, P089, P124
Figueroa, Lourdes Carvajal, V011
Fishman, Julia, P048
Flavio, Perricone, P128, S045
Flores, P, V007
Foo, Eric, P067
Foroutan, HamidReza, P019
Fraga, Jose Carlos, S017
Fraile, Andres Gomez, P110
Fraire, C, S014
Francesca, Alicchio, P128, S045
Fujino, Junko, P078
Gaitonde, Krishnanth, P068
Gamba, PG, S070
Gandhi, Rajinder R, P051
Garcia-Hernandez, Carlos, S044, V011
Garey, Carrisa, P121
Garrett, Deiadra, S040, S048, S054, V015
Geiger, James, S071
Geodakyan, Oganes, P101
Georgeson, Keith E, P076, S053
Geyer, Christian, P084, S056
Gfroerer, Stefan, P028
Giné, C, P038
Giuliani, Stefano, S070
Giuseppe, Ascione, S045
Glybina, Tatiana M, P079, S060
Godoy, Jorge, P049, P106
Golebiewski, Andrzej, P090
Gonzalez, Gloria, P049, P106
Gordo, Maria Isabel Benavent, P110
Gorecki, Wojciech J, P052
Gorodnicheva, Julia M, P135
Grant, H, P021
Gray, Brian W, S071
Graziano, Kathleen, S058
Guelfand, Miguel, P111
Gusev, Alexey A, P088
Gutierrez, Roberto Suarez, V011
Guven, Ahmet, P139
Haddad, Munther, P048
Halibieke, Abudebieke, S007
Hall, Nigel J, P099
Hamitaga, Flurim, P015
Hannan, Jafrul, P006
Hansen, Erik N, P026, S041
Hao, Wei, P073
Haque, Ashraf-Ul, P006
Harmon, Carroll M, P076, S041, S053
Harth, Karem C, S008
Hasan, Abdullah-Al, P006
Hashizume, Makoto, P003
Hassan, AlHassan M, P056
Hatanaka, Masahiro, P078
Hattori, Kengo, P075
Hay, Sameh A, P046
Hebra, Andre, P113
Hegazy, Nedal, P046
Henriques, Steven, P093
Henry, Steyaert, P029
Herbst, Katherine, S029
Hien, Pham Duy, S010, S012
Hill, Sarah J, S016, S051, S058
Hinojosa, Marcelo W, V014
Hirschl, Ronald, S071
Hisley, Kenneth, P067
Hoan, Vu Manh, S010, S012
Hofmann, Alejandro D, P091
Holbrook, C, P136
Holcomb III, George W, S018, S058, P121
Hollands, Celeste, P071
Hoque, Mozammel, P006
Hoseini, S. Mohammad Vahid, P019
Hou, Wenying, P027
Hsin, Yu-Mei, P063
Ida, Giurin, P128, S045
Ieiri, Satoshi, P003
Igarashi, Akihiro, P078
Ikeda, Hitoshi, P078
Ilhan, Huseyin, P069, P115
Inge, Thomas, S063, V002
Ishimaru, Tetsuya, P072
Ishimaru, Yuki, P078
Islam, Saidul, P127
Islam, Saleem, V016
Iwanaka, Tadashi, P072, P096
Jacobsen, AS, P070
Jaeschke, U, S006
Jaimes, Paula J, P124
Jawaheer, G, S021
Jawaid, Wajid, P116
Jenkins, Todd, S063
Jesudason, Edwin C, P116
Jiang, Dapeng, P032
Jie, Zhu, S001
Jolley, Jennifer A, V014
Joseph, Jacob R, P008
Juang, David, P121, S018
Juarez, Sergio Landa, V011
Juhnke, Bethany, P067
Jung, Soo-Min, S068
Juri, Ignacio Ruiz, P107
Jurkiewicz, Beata, P138
Kadaba, Srimurthy, P065, P112
Kane, Timothy D, S034
Kanters, Arielle E, P058
Kato, Yoshifumi, S007
Katz, Michael S, P092, S043
Kavatzas, Nikolaos, S005
Kawashima, Hiroshi, P072, P096
Kazancev, Anatoly, P133
Kazantchev, Anatoliy, S062
Keijzer, Richard, S041
Kelly, Katherine B, S008
Kennedy, Alfred P, P083
Kerimov, Polad, P034, S015, S062
Khairi, Ahmed, P134
Khalifa, OM, P053
Khalil, T., P108
Khurana, Sanjeev, P120
Kiely, Edward, S017
Kim, Christina, S029
Kim, Dae Yeon, P057
Kim, In Koo, P057
Kim, Peter C, S024, P122
Kim, Seong Chul, P057
Kim, Tae Hoon, P057
Kimura, Takuya, S069
Kirgizov, Igor V, P088
Kitagawa, Norihiko, P105
Kleinsteuber, Karin, P106
Kodaka, Tetsuro, P072
Koga, Hiroyuki, P114
Kononenko, Marina, P007, S042
Koontz, Curt S, S016
Kose, Coskun, P030
Kostakis, Alkiviadis, S005
Kosumi, Takuya, S069
Kozlov, Mikhail Y, S060, S072
Kozlov, Yury, P007, S042
Krafka, Karel, P037
Krasnov, Pavel, P007, S042
Kremer, Nathalie, S053
Kronfli, R, S066
Krpata, David M, S008
Krysta, Miroslaw M, P052
Kubiak, R, P021
Kucuk, Gonul, P030, P031
Kuebler, Joachim F, P091, S013
Kulikova, Nadezhda, S022
Kutubidze, Ramaz, P045
Lacher, Martin, S053
Lacreuse, Isabelle, P100
Laer, Van, P108
Lagausie, Pascal DE, S023
Laing, Rob, P120
Laje, Pablo, S058
Lal, Dave, V004
Lam, JPH, P132
Lane, Geoffrey J, P114, S007
Langer, Jacob C., P122
Langness, Simone, S016
Lauron, Jerome, P029
Lazarus, Colin, S061
Leclair, MD, P009
Ledbetter, Daniel, V013
Lee, Alex C, P059
Lee, Jui-Ying, P020, P063
Lee, Suk-Koo, S068
Lee, Timothy, V002
Leeper, William R, V012
Lempe, M, S006
Lerminiaux, C., P123
Leuthardt, Rudolf, P015
Leys, Charles M, S058
Li, Bing, P024
Li, Goqing, P098
Li, Long, P024, P027, S011
Li, Suolin, P040, P041, S004, S035
Li, Yingchao, P040
Li, Zhaozhu, P032
Liang, Kaicheng, S037
Liberto, Daniel, P109
Liem, Nguyen Thanh, P129, S010, S012, S073
Light, Edward D, S037
Linacre, Virginia, P106
Linder, Verena, S061
Lino, Mauricio Urquizo, P109
Lisi, G, P043
Liu, Shu-li, P024, S011
Liu, Xuelai, P073
Lobe, Thom, P067
Lobos, Pablo, P109
Lombardo, Michele L, P010, P044, S057
Lopez, Juan C, V008
Lopez, Manuel, S023, S065
Losin, Marcin, P090
Lu, Liangsheng, S028, S032
Lu, Yiqun, S032
Luks, Francois I, P010, P044, S057
Lv, Zhi-bao, S064
Lydon, Eileen M, P016
MacKinlay, GA, S021, S066, P047, P132
Maestri, Luciano, S050
Mahomed, Anies, P127
Mammadov, Emil, S025, S030
Mancini, Matt, P083
Marhuenda, C, P038
Marianna, Iaquinto, P128, S045
Marino, N, P043
Marsaud, Alexandre, P131
Martinez-Escobar, Marisol, P067
Martinez-Ferro, Marcelo, P094, S046
Martinez-Ibanez, V, P038
Marven, Sean, P061
Mascianica, Katarzyna, S020
Massimi, Tareq, P010
Mattei, Peter, S058
Mayer, Steffi, P084, S056
McHoney, MC, P047
McKee, Milissa A, P016
Meehan, John J, V009, V013
Meeussen, C, P039
Mei, Diao, P027
Mei, Hong, S026, S033
Mendelson, Kim G, P092
Mendoza-Sagaon, Mario, P015
Mergan, F., P108
Meroni, Milena, S050
Merritt, Neil H, V012
Metzelder, Martin L, P091
Micheal, Kontos, S005
Midrio, Paola, S070
Millan, Carolina, P094, S046
Miranda, Alice, S036
Mitupov, Zoricto, P101, S022
Miura, John, V004
Miyahara, Katsumi, S007
Miyano, Go, S007
Miyauchi, Yuya, P075
Modesto, Bernardina B, P117
Moir, Christopher R, S038
Molina, Ivan D, P087, P089, P124
Mollen, Kevin P, S034
Moon, Suk-Bae, S068
Moreira, Agner A, S074
Moreira-Pinto, João, P060, S036
Morishita, Yuji, S055
Moront, Matthew L, P092, S043
Mortellaro, Vincent E, S018
Muensterer, Oliver J, P026, P076, S041, S053
Muensterer, Oliver, S058
Muise, Eleanor D, P035
Mungan-Akin, Ilke, P031
Munro, FD, S021, S066, P047
Muratore, Christopher S, S057
Nagarsheth, Khanjan, P083
Nagy, Brittany K, S043
Najafi, Soltan, P019
Nakano, Rejane, P117
Narasimhan, KL, P070
Narciso, Alessandra, S070
Neissner, Claudia, P126
Nguyen, Nam, S040, S048, S054, V014, V015
Nogami, Takashi, S055
Noh, Paul H, P068
Noomaan, A, P053
Nordenskjöld, Agneta, P042
Nour, FM, P053
Novillo, Indalecio Cano, P110
Novogilov, Vladimir, P007, S042
Numanoglu, Alp, P004
Oberbach, Andreas, S002
O'Brien, Barbara M, S057
Ohhama, Youkatsu, P105
Okazaki, Tadaharu, P114, S007
Okulov, Alexei B, S060
Okulu, Emel, P031
Oliveira, Carol, P122
Olsen, Melanie, P120
Ong, CP, P070
Ong, LY, P070
Ostlie, Daniel J, P121, S018
Otte, F., P108
Ozcan, Rahsan, S025
Padshah, Waisullah, P119, P139
Paiva, Kelly C, S074
Pan, Weihua, P097, P098
Pandya, Samir, S051, V006
Papachristos, Dimitrios, S005
Papadopoulos, J., P108
Papalois, Apostolos, S005
Pappalepore, N, P043
Pardy, Caroline, P048
Patkowski, Dariusz, P118, S020
Pavlopoulos, Dionisis, S005
Paz, Enrique, V008
Pearl, Richard H, P093
Peiro, JL, P038
Perger, Lena, S041
Periklis, Tomos, S005
Persico, A, P043
Pessoa-Sousa, Calebe, P018, P050
Petersen, Claus, S013
Petit, Thierry, P033, P036
Philippe, Paul, S023
Pierro, Agostino, S017
Pimpalwar, Ashwin, P008, P017, P074, P077, P082, S049
Poddoubnyi, Igor V, P079, P135, S047, S060, S072
Podevin, G, P009
Podevin, Guillaume, S023
Podkamenev, Alexey, P007, S042
Pogorzelski, Andrzej, P118
Polleichtner, S, S006
Ponsky, Todd A, S008, P058
Potter, D D, S038
Potts, S R, S021
Poupalou, Anna, S005
Prasad, Rajeev, P035, P092, S043
Prodan, Silvana, P109
Prudnikova, Tatyana A, P088
Pu, Jiarui, S026, S033
Qiangqiang, Cui, P025
Qinglin, Sun, S001
Questa, H, S014
Quynh, Tran Anh, S073
Rachkov, Victor, P002, P101, S022
Rai, R, P070
Ramadan, Marwa, P066
Ramadan, Moustafa, P066
Ramadwar, Ravindra, P014, S027
Rasputin, Andrey, P007, S042
Ravasse, Philippe, P033, P036
Rawat, David, P048
Razumovskiy, Alexander, P101
Razumovsky, Alexander, P002, S022
Reddy, Pramod P, P068
Reddy, Trisha P, P068
Reingruber, B., P104, S009
Ribeiro de Castro, João Luís, P060
Riccipetitoni, Giovanna, P062, S050
Rizalar, Riza, P023
Rod, Julien, P033, P036
Rodesch, G., P123
Rodriguez, Monica, P124
Roesch, Wolfgang H., P126
Rohleder, St, P011, P013
Roig-Francoli, Jennifer, P068
Rolanda, Carla, S036
Rolle, Udo, P028
Romero, P., S009
Rothenberg, Steven, S017, S019, S034, V003, V010
Ruan, Shuangsui, S028, S032
Rubenwolf, Peter, P126
Rutqvist, Jan O, P022
Rybakova, Diana, P034, P133, S015, S062
Rybansky, Mihail, P133, S062
Rybov, Andrey, P034, P133, S015, S062
Sabharwal, A J, S066
Sager, Cristian, V008
Said, Hanan, P066
Sakarya, Turgay, P119, P139
Salas de Armas, Ismael, P074, P077
Salas De Armas, Ismael, P082
Saldaña, Lily J, P064, S052
Salomon, Anahi, P109
Samotyjek, Joanna, P138
Sanchez, Raquel Tejedor, P110
Santhanakrishnan, Ramesh, P065, P112
Sarhan, Mohammad, P051
Sato, Masahito, P075
Sawai, Toshio, S069
Schaarschmidt, Klaus, S006
Schier, F, P011, P013
Schlesinger, F, S006
Schmosich, Steve J, S008
Schneider, Anne, P100
Schukfeh, Nagoud, S013
Schulz-Menger, J, S006
Schwartz, Marshall Z, P092, S043
Selvaggio, Giorgio, P062
Seo, Jeong-Meen, S068
Shah, Ami, V016
Shehata, Sameh, P134
Shehata, Sherif M, P053, P056
Shin, Hyun-Baek, S068
Shinkai, Masato, P105
Shipman, Kristin, V010
Sidler, Daniel, P005
Silva, João Guilherme, P060
Simango, Itayi, S061
Sirkin, Nicolay, P007, S042
Sivan, Bezalel, P068
Skerritt, C, P021
Sloots, CEJ, P039
Smirnova, Svetlana, P002, S022
Smith, Stephen W, S037
Snyder, Charles L, P121
Sokolov, Yuriy, P080
Solecki, Krzysztof A, P052
Solovjev, Alexey, P007, S042
Son, Tran Ngoc, S010
Sousa-Filho, Humberto B, P018, S074
Soylet, Yunus, S025, S030
St. Peter, Shawn D, P121, S018, S058
Stanfill, Amy B, P093
Stanton, Michael P, P099
Steinbrecher, Henrik A, P099
Stephenson, Jacob, V009, V013
Steyaert, H, P001, P131
Streck, Chris, P113
Struijs, MC, P039
Suarez, Carlos S, P107
Suarez-Gutierrez, Roberto, S044
Suda, Sonia, S037
Sun, Chi, S035
Surer, Ilhami, P119, P139
Suzuki, Kan, P072
Suzuki, Kenji, P114
Suzuki, Makoto, P078
Svensson, Jan F, P022, P042
Swiatek, Katarzyna, P118
Switzer, Diane, P093
Taguchi, Tomoaki, P003
Tahara, Kazunori, P078
Takahashi, Masaki, P072
Take, Hiroshi, P105
Tam, Paul, P073
Tanabe, Yoshihide, P096
Tander, Burak, P023
Tang, Shao-tao, S067
Tanoue, Kazuo, P003
Temeltas, Esra, P030
Terawaki, Kan, P072
Tibboel, D, P039
Till, Holger, P084, S002, S056
Timmapuri, Shaheen J, P092, S043
Tokar, Baran, P069, P115
Tolstov, Kirill N, P079, P135, S047, S072
Tomikawa, Morimasa, P003
Tong, Qiangsong, S026, S033
Torre, Michelle, P095
Torres, Manuel B, S040, S054, V015
Toselli, Luzia, P109
Troncoso, Bernardita, P111
Trubitsyn, Alexei, P080
Tsai, Feng-ji, P020
Tsang, T, P136
Tumanyan, Grachik, P080
Tung, Jeanne, S038
Turial, S, P011, P013
Udaquiola, Julia, P109
Udatsu, Yuko, S055
Uemura, Munenori, P003
Ure, Benno M, P091, S013
Vagni, Roberto, P109
Vajsar, Jiri, S024
Valamiel, Roneyara R, S074
Valla, Jean-Stephane, P001, P029, P131
Vallejos, Javier, P094
Valusek, Patricia A, S058
Valverde, Rocio Morante, P110
Van de Ven, CP, P039
Van De Winkel, Nele, P085
Van Der Veken, E., P108, P123
Van Hoorde, E., P108
van Niekerk, Martin L, P054
Van Obbergh, L., P108
van Rensburg, Carla, S061
Vanderlinden, Kim, P085
Varela, Patricio, P095
Varlet, Francois, S065
Vazquez, Araceli Garcia, P110
Vegunta, Ravindra K, P093
Vella, Claudio, P062, S050
Victor, A, P009
Viet, Nguyen Duy, P129
Vieten, Gertrud, P091
Viglio, Camilla, P062
Vilesov, Alexei, P080
Villalona, Gustavo A, P051
Vintila, Alina I, P061
Volobuev, Andrey, P034, P133, S015, S062
von Allmen, Daniel, S037
von Bergen, Martin, S002
von Delft, Dirk, S061
Wachowiak, Robin, P084, S056
Walker, G M, S066
Wallace, Lizabeth J, P093
Wang, Guo-bin, S067
Wang, Jaw-Yuan, P020
Wang, Jian, S003
Wang, Jun, P097
Wang, Shou-qing, P024
Wang, Xiang, S032
Warren, Sara L, P004
Watson-Smith, Debra, S057
Weber, Irina, P007, S042
Weber-Eibel, Jutta, P037
Weller, Santiago, V008
Werner, Antje, P084, S056
Wester, Tomas, P022
Wijnen, R, P039
Wijtenburg, E, P108
Wilson-Storey, D, S066
Winer, Eliot, P067
Wojciechowski, Piotr K, P052
Wong, Kenneth, P073
Wu, Yeming, P097, P098
Wulkan, Mark L, S016, S051, S058, V006
Xi, Hongwei, P025
Xiao, Xian-min, S064
Yagi, Makoto, S055
Yagmurlu, Aydin, P030, P031
Yagoubi, Fatima, S005
Yakubu, Abdulkadir, P137
Yamataka, Atsuyuki, P114, S007
Yamauchi, Katuji, S069
Yan, Zhilong, P097
Yang, Chunlei, S026, S033
Yang, Yang, S004
Yang, Ying, S067
Yap, TL, P070
Yee, Low, P070
Yoder, Suzanne, V003
Yonekura, Takeo, S069
Yoshida, Hideki, S055
Yu, Zengwen, P040, P041, S004, S035
Zagrosek, A, S006
Zaki, Ahmed M, P046
Zaparackaite, Indre, P127
Zegarra, Cecilia Moreno, P110
Zhang, Huanyu, S026, S033
Zheng, Shan, S064
Zhong, Zhiyong, P041
Zhou, Yi-ming, S064
Footnotes
*
Toki A, et al. Ultrasonographic diagnosis for potential contralateral inguinal hernia in children. J Pediatr Surg 2003;38:224–226.