
Abstract
Abstract
Introduction:
Severe pectus excavatum (PE) is a deep chest wall deformity that generates both a cosmetic damage and a cardiac/respiratory function impairment. Excluding the scarce reports on Marfan's syndrome (MFS) and Ehlers-Danlos's syndrome (EDS), few studies have examined the relation between severe PE and connective tissue disorders. The aim of this study is to verify the clinical significance of such correlation.
Subjects and Methods:
Ninety-two consecutive patients, of whom 79 were males, between 6 and 34 years old, classified as having severe PE, were seen at our institution from June 2005 to September 2010. All patients underwent clinical, ophthalmological, cardiac, and radiological (chest and spine magnetic resonance imaging) screening. The following features were observed: skin stretch marks, scoliosis, joint hypermobility, echocardiographic signs, spinal defects, and myopia.
Results:
Classical connectivopathies such as MFS or EDS were present in only 5 patients (approximately 5%), whereas a single deformity was present in 4. The largest group (approximately 71%) was represented by phenotypical alterations such as mitral valve prolapse, aortic root enlargement, and skeletal and skin alterations (MASS). Among those patients, the most frequent clinical manifestations were the skeletal ones, followed by skin marks and mitral valve prolapse.
Conclusions:
PE showed an evident association with an array of features that we describe as MASS. Although not one of this subgroup of patients has been described with increased aortic root diameter when screened (a feature widely present in MFS patients), they probably would require a thorough and longer follow-up than those affected by isolated PE because of the potential occurrence of severe cardiovascular complications such as aneurysms and dissection, which are major causes of morbidity and mortality in MFS.
Introduction
PE etiology is uncertain, but a familial tendency has been noted, and although a direct genetic link has not been identified, still approximately 40% of patients with PE have relatives with various deformities.1,13,14 PE is known to be frequently associated with hereditary connective tissue disorders, such as the mitral valve prolapse, aortic root enlargement, and skeletal and skin alterations (MASS) phenotype and Marfan's (MFS), Ehlers-Danlos's (EDS), Poland's, and mitral valve prolapse syndromes.15–19
MFS is a systemic autosomal dominant connective tissue disorder caused by several mutations in the gene encoding the glycoprotein fibrillin-1 (FBN1) situated on chromosome 15q21. MFS has an incidence of 2–3 cases in 10,000,15,16,20 and PE is present in two-thirds of patients with MFS.15,20–22 The clinical manifestations of MFS vary in range and severity and may involve several organs; the most frequent anomalies are found in the cardiovascular, respiratory, ocular, and skeletal systems.16,23 Cardiovascular diseases (aortic dilatation and dissection) are the major cause of morbidity and mortality.24–26 Although molecular testing for mutations in the FBN1 gene is widely available today, the diagnosis of MFS cannot be reliably established by a simple demonstration of a gene mutation,24,27 and it is more likely dependent on a combination of major and minor signs as defined in the Ghent criteria.24,28,29 For an instance, severe PE that requires a surgical repair is one of the major skeletal criteria for MFS diagnosis.15,17,27
MASS is an acronym described at first in 1989 by Glesby and Pyeritz 30 that defines an array of clinical features such as mitral valve prolapse, nonprogressive aortic enlargement, and skeletal and skin alterations. It is described as an autosomal dominant disease that results from mutations in the FBN1 gene and belongs to the group of connective tissue disorders characterized by a slight, generalized laxity of the connective tissue, with low aortic risk.18,29,31,32 In patients with MASS phenotype, aortic root diameter may be at the upper limits of normal for body size, but there is no documented progression to aneurysm or predisposition to dissection and a scarce understanding of its clinical value.18,29,30,33 Mutations in the FBN1 gene have been associated with variable clinical phenotypes, ranging from MASS phenotype to classic MFS, isolated ectopia lentis, and isolated ascending aortic aneurysm and dissection. 34 To date, apart from limited reports on MFS and EDS, few studies have described correlations between PE and connectivopathies spectrum.
In our patients, MASS phenotype was frequently associated with PE deformity. Starting from this assumption, the aim of this study was to verify the correlation between MASS features and PE severity. Moreover, we investigated, whenever present, the clinical significance of such correlation that in the end may have an impact on the outcome of surgical repair.
Subjects and Methods
A retrospective analysis was performed on a series of 92 consecutive patients affected by PE who were seen at our Paediatric Surgical Centre from June 2005 to September 2010. As a part of the clinical or preoperative assessment, these patients underwent a thorough clinical, ophthalmological, cardiac, and radiological (chest and spine magnetic resonance imaging) evaluation. We collected demographic data, PE gravity, and the Haller Index, which is defined as the ratio between the horizontal distance of the inside of the ribcage and the shortest distance between the vertebrae and sternum extrapolated from magnetic resonance imaging scans.6,35–37 Moreover, at the outpatient preoperative evaluation, the following clinical features were observed: skin stretch marks, skeletal features, echocardiographic signs, lumbosacral dural ectasia, and myopia. According to the clinical features and instrumental results, patients were classified as only PE deformity, MFS, EDS, MASS phenotype (MASS), slight laxity of the connective (SLC), or SLC with an extensive involvement of the skeletal system (SLC*).
For the MASS subset we calculated a grade, proposed as the MASS score, 27 which ranged from 1 to 4, based on the presence/absence of clinical features related to connectivopathy such as mitral valve prolapse, myopia, and skeletal and skin alterations. We defined MASS score 1 as those patients who presented with only skeletal alterations as in “sole” PE deformity, SLC, and SLC*. Conversely, MASS phenotype and EDS and MFS patients ranged in from MASS score 2 to 4 according to their clinical features.
In addition, because all of our patients were affected by a skeletal deformity such as PE, two other scores were proposed (1996 Ghent criteria). The first, termed the Skeletal score (S score), was purely based on the number of major skeletal features as previously described (Table 1).24,28 The latter, termed the Total Skeletal score (TS score), was based instead on every skeletal alteration comprising both major and minor features (Table 1).
In order to estimate an association between clinical features and defect gravity, we looked for a correlation between the aforementioned scores with the Haller Index.
Statistical analyses were performed using Stata version 10 SE Data Analysis and Statistical Software for Windows. Continuous normally distributed data are presented as mean±standard deviation values, whereas continuous non-normally distributed data are presented as median (range) values. A correlation index and a linear regression analysis were estimated between scores and the Haller Index. A value of P<.05 was considered statistically significant.
Results
At our Paediatric Surgical Centre, from June 2005 to September 2010, we reviewed 92 patients, of which 13 were female (14%) with a median age of 13 (6–18) years and 79 were males (86%) with a median age of 16 (8–34) years. We assigned a MASS score to each of them as reported in Table 2. Patients were then classified according to diagnosis (Table 3); 66 individuals (72%) displayed the MASS phenotype, which appeared to be the largest subgroup. Within this group 29 had a MASS score of 2 (44%), 30 had a score of 3 (45%), and 7 had a score of 4 (11%). The most frequent clinical features were the skeletal ones present in all the patients as reported in Table 4. The MASS score showed a direct correlation with the age of the patients (i.e., from 13 years old for patients with the lowest score to 19 years old for patients with the highest) (Table 5).
MASS, mitral valve prolapse, aortic root enlargement, and skeletal and skin alterations.
LLC, slight laxity of the connective; LLC*, slight laxity of the connective with an extensive involvement of the skeletal system.
A mild aortic root dilatation was present in 5 cases (5.4%): 1 was defined as MASS phenotype (MASS score 3; diameter, 32 mm), whereas the other 4 were classified as MFS (diameter, 31–38 mm).
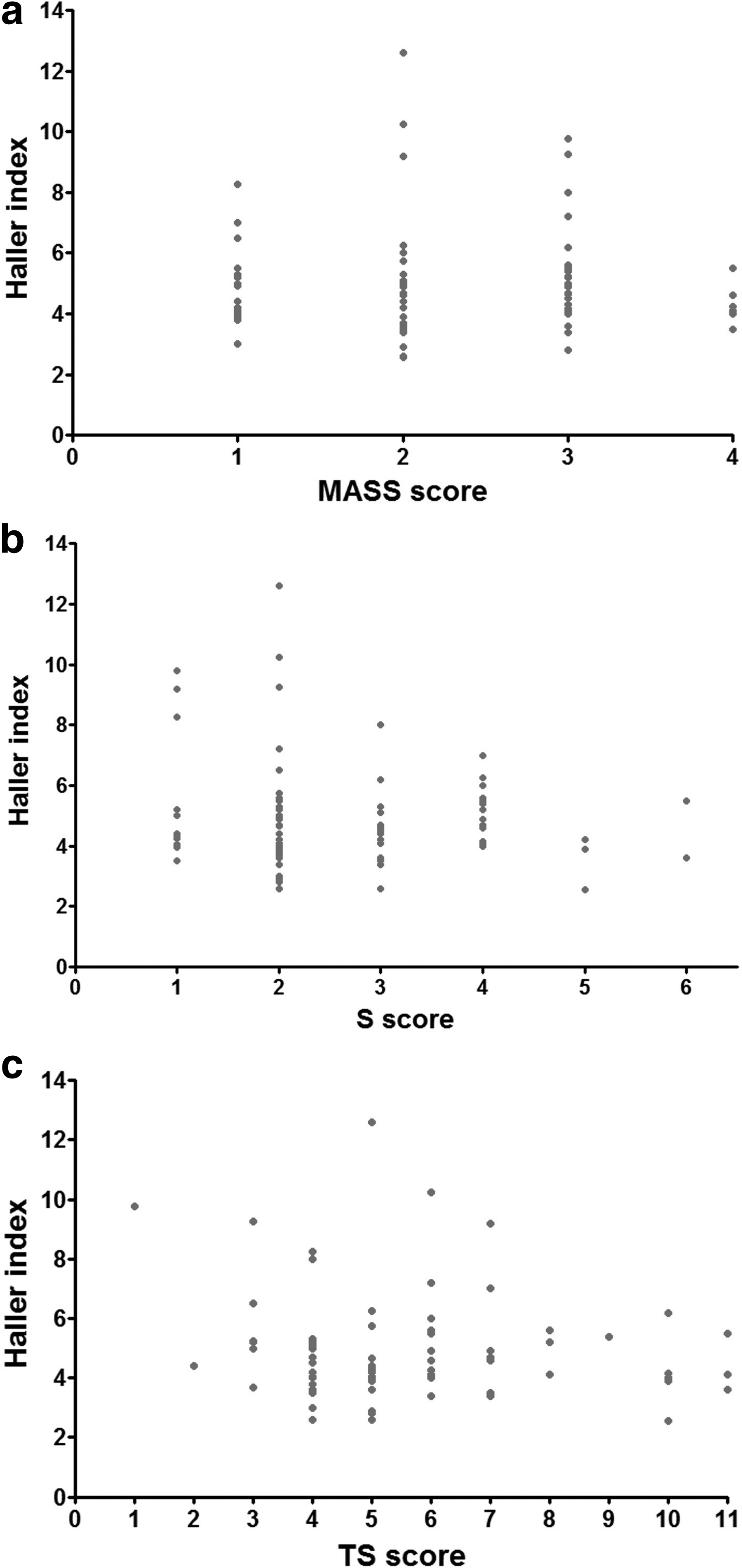
We analyzed the correlation between the MASS score, TS score, and S score with the Haller Index (Fig. 1). The calculation of the correlation index confirmed the absence of an increasing or decreasing pattern, except for the S score and the Haller Index, where there was a weak negative correlation (Table 6). Hence we calculated the regression line, which appeared to be not significant (P=.186). Three further tests of independence confirmed the independence of the MASS score, TS score, and S score with the Haller Index (P=.525, P=.802, and P=.509, respectively).
Correlation of Haller Index with
Fifty-three patients (58%) underwent MIRPE. Nuss bar dislocation happened in 2 cases only (2/52 [3.8%]), which required a second operation (one had a MASS phenotype with MASS score 3, and one had SLC with MASS score 1).
Discussion
Our study is a retrospective analysis performed on a series of 92 consecutive patients affected by PE who were seen at our institution, of which the largest subset was represented by phenotypical alterations such as mitral valve prolapse, aortic root enlargement, and skeletal and skin alterations, defined as the MASS phenotype. The aim of our study was therefore to analyze first the correlation between this phenotype and PE severity, and, when present, we wanted to elucidate the clinical significance of such correlation, which at last may have an impact on the outcome of surgical repair.
Although PE is commonly seen in patients with underlying connective tissue abnormalities, only a handful of studies have documented the outcomes of surgical repair in this population. In 1985 Golladay et al. 22 compared the characteristics of 45 children who underwent surgical repair according to the Ravitch procedure, of which 7 were affected by PE and MFS and 38 had PE without MFS. They claimed that to achieve an acceptable defect correction in PE patients with MFS, the use of a substernal strut was essential,15,22 as confirmed later also by other authors. 21 Arn et al. 38 in 1989 reviewed the records of 28 patients with MFS and 30 patients with presumed isolated PE in order to determine the surgical repair outcome of PE in MFS. They concluded that PE may suggest the presence of an underlying heritable disorder of connective tissue such as MFS; furthermore, in patients with MFS or other connective tissue disorders, surgical repair should be delayed if possible until skeletal maturity is nearly completed and should use an internal stabilization. 38 In 2002 Croitoru et al. 39 published their surgical experience with MIRPE in a population of 303 patients, which included 16 patients with a confirmed diagnosis of MFS and 49 with a suspected diagnosis of MFS (nonspecific connective tissue disease). In 2009 Olbrecht et al. 20 studied a group of patients with PE who underwent MIRPE who had connective tissue disorders (MFS, EDS, and nonspecific connective tissue disease). Finally, in 2010 Redlinger et al. 15 compared operative and postoperative characteristics of MFS patients, patients with marfanoid features, and all other patients undergoing MIRPE. They concluded that MIRPE is a safe procedure for patients with MFS or marfanoid features, showing equally good results. In any case, to date, no study had addressed yet surgical outcomes in patients with MASS phenotype undergoing PE repair. The PE–MASS phenotype association is not commonly emphasized, and our data show that it may be very frequent. We have found a high incidence of MASS phenotype among our patients, accounting for about two-thirds of the total PE population, whereas in our study, in a finding consistent with other reports, MFS represents only about 4%. 15
PE patients are known to be affected by structural abnormalities of type 2 collagen in the costal cartilage, abnormal levels of ions such as zinc, magnesium, and calcium, and a disturbance of collagen synthesis as described by biochemical studies.1,3,13 This consideration implies that nearly all of the patients affected by PE displayed a variable laxity of the connective tissue, with probable abnormalities in both the structure and collagen synthesis. Deriving from that, thanks to a thorough clinical and instrumental assessment, we were able to differentiate various phenotypes in the connectivopathy spectrum, focusing on the most prevalent one represented by MASS phenotype.
Aortic aneurysm and dissection are known as significant major causes of morbidity and mortality in MFS patients.18,32 Mutations in the FBN1 gene may have a significant causal role in descending aortic dissections in patients who have a Marfan-like syndrome. 34 To date there are no data documenting the stability of aortic diameters over time. 31 Mortensen et al. 31 observed 4 MASS patients with normal aortic diameters and 1 patient with MASS phenotype with 5 mm progression of aortic diameters. Rybczynski et al. 27 prospectively evaluated 279 patients with suspected MFS, and almost one-quarter of patients had some other hereditary disorder of connective tissue, half of which involved the cardiovascular system. When we analyzed our patients, 5 cases had a mild dilatation of the aortic root. This cardiovascular feature is rarely found among the MASS phenotype population, representing only about 1.5% of the whole MASS cohort. It is likely that these patients do not generally progress to aortic aneurysm or have a predisposition to dissection, but in clinical practice it remains difficult to identify an increased aortic risk in individuals with Marfan-like features, especially when these do not have the classic stigmata of MFS. Therefore, larger studies with comprehensive clinical and echocardiographic follow-up over years are needed to predict aortic disease progression in Marfan-like syndromes. 31
At the beginning of this study, as previously described for MFS,39,40 we postulated that the severity of the hereditary connective tissue disorder could have an important impact on the success of the surgical procedure. Nonetheless, in our series we did not find any correlation between the gravity of clinical manifestations and the surgical outcome. Fifty-three patients (58%) underwent MIRPE. Nuss bar dislocation happened in 2 cases only (2/53 [3.8%]), which required a reoperation (MASS score 3 and one MASS score 1). The presence or absence of a severe connective tissue disorder was therefore not decisive on the success of surgery, although a larger cohort may be needed in order to draw any conclusion. To estimate an association between clinical features and the defect gravity, we looked for a correlation between these arbitrary scores extrapolated from Ghent nosology24,28 such as the MASS, S, and TS scores with the Haller Index. Our results, conversely, disproved every possible association: these parameters were revealed to vary independently from the Haller Index. In particular, our data demonstrated that there was no association between the Haller Index and gravity of clinical features.
In conclusion, we have described a significant association between PE and MASS phenotype, a slowly progressive pathology, without mortality and morbidity equal to MFS. Our results showed that there is no correlation between this phenotype's gravity and the surgical outcome of corrective surgery for PE. Yet, at present, there is no information about the risk of complications or about the long-term prognosis in MASS patients; hence strategies for clinical management remain still undefined. In any case, we advocate an extended clinical and echocardiographic follow-up over time, first of all because of the possible worsening of the mitral valve prolapse that is a feature present in nearly half of the MASS population. Moreover, although this point is still debatable, some of these patients might evolve toward a rare but severe clinical manifestation that is typical of MFS such as dissecting aortic aneurysm.
Footnotes
Disclosure Statement
No competing financial interests exist.