
Abstract
Abstract
Background:
Helium is used as an insufflation gas to avoid the negative properties of carbon dioxide (CO2), such as CO2 accumulation, acidosis, and tachycardia, particularly in the case of insufficient respiratory function, seen also in infancy. Any laparoscopic procedure carries the risk of a gas embolism.
Materials and Methods:
Seven anesthetized piglets (weighing 9.9–12.8 kg), randomized into three groups, served as models for pre-teenage children. Three piglets received a CO2 embolism, followed by a helium embolism of 2 mL/kg, respectively. Helium was administered to three piglets, whereas both gases were repeatedly administered alternately to one piglet. The embolisms were administered for 30 seconds via a central venous line. Cardiac output was measured using the thermodilution method. The observation period for each embolism was 60 minutes in Groups 1 and 2 and 15 minutes in Group 3.
Results:
All animals survived CO2 embolisms. Four of the six piglets died after helium embolisms. Following helium embolisms there was a prompt initial decrease in the end-tidal CO2 pressure and an initial increase in the pulmonary arterial pressure. A further decrease in arterial blood pressure was prevented by a compensatory increase in the heart rate and appeared just before death. After only 5 minutes cardiac output showed a 25% decline from the initial value. Helium embolisms led to a severe increase in the pulmonary dead space.
Conclusions:
Embolisms with the smallest amounts of helium administered via direct venous puncture have an immediate lethal impact. Extended perioperative monitoring and trocar placement under vision should be performed.
Introduction
Previous research groups have described the lower potential risk of CO2 effects compared with helium in inter-individual comparisons for direct embolism only in adult animals.19,20 Comparisons of intra-individual administration of CO2 and helium in the same animal are restricted to measurements of the outcome. 21 A further study involving intra-individual administration compared CO2 and oxygen (O2) embolism. 22
The aim of this study was to directly compare helium and CO2 embolism upon direct vessel injury intra-individually.
Materials and Methods
Study design
The study was approved by the local ethics committee. Care and handling of the animals were in accordance with animal research guidelines.
Seven male German Landrace piglets (weighing 9.9–12.8 kg; mean, 11.4 kg) were investigated and served as a model for pre-teenage children. They were grouped randomly into three groups (Table 1). The defined gas volumes of bolus embolisms were injected via the central venous line and detected in the right atrium using ultrasonography. In Group 1 a single helium bolus embolism was manually administered (2 mL/kg/30 seconds), followed by a 60-minute observation period. In Group 2, instead of helium, CO2 was used. In order to achieve an intra-individual comparison between the impact of CO2 and helium bolus embolisms the animals of Group 2 furthermore received a helium embolism 60 minutes later (2 mL/kg/30 seconds). In Group 3 a single animal was used in order to achieve values for repetitive embolisms with different volumes of CO2 and helium (9 mL of CO2, 3 mL of He, 9 mL of CO2, 9 mL of He, and 9 mL of CO2). Repetitive injections were performed at 15-minute intervals.
Group 1, helium embolism; Group 2, carbon dioxide (CO2) embolism followed by helium (He) embolism after 1 hour; Group 3, alternating repetitive administrations of CO2 and helium in 15 minutes.
Anesthesia and preparation
After intramuscular sedation (10 mg/kg ketamine and 2 mg midazolam) with the piglet in a supine position an intravenous line was placed. Anesthesia was induced with midazolam (5 mg), fentanyl (0.05 mg), and pancuronium bromide (2 mg) and was maintained with continuous infusion of sodium pentobarbital (4 mg/kg/hour) and fentanyl (6 μg/kg/hour). Muscle relaxation was maintained with pancuronium bromide (0.3 mg/kg/hour). After endotracheal intubation, pressure-controlled ventilation with the Servo 900C ventilator (Siemens-Elema, Solina, Sweden) was adjusted to normocarbia (PCO2 in the carotid artery [PCO2, a carot]=35–45 mm Hg). Total fluid replacement was approximately 10 mL/kg/hour. Cutdowns were performed to place a pulmonary artery catheter, a central venous line, and an arterial line in the carotid artery. After all cannulizations had been performed the piglets were allowed to stabilize for 30 minutes. A warming blanket and a red light heater were used to prevent hypothermia. At the conclusion the animals were sacrificed, and the positions of the endotracheal tube and the central lines were verified by autopsy.
Measurements
Measurements of end-tidal PCO2 (PCO2, et), mean arterial pressure (Pa carot, mean), heart rate (fc), and mean pulmonary arterial pressure (Pa pulm, mean) were obtained in Group 1 and Group 2 every minute for the first 10 minutes and at 5-minute intervals for the next 20 minutes. The data were measured by an E-PRESTIN module (i4 iMM F-CU8) and displayed on an iMM anesthesia monitor (GE Healthcare, Datex Ohmeda GmbH, Freiburg, Germany). Cardiac output was measured via a 5 French pulmonary artery catheter (reference number 132F5; Edwards Lifesciences, Unterschleissheim, Germany) by thermodilution. Arterial PCO2 (PCO2, a carot) and arterial O2 saturation (SO2, a carot) were measured by blood gas analysis with the Rapidlap 248 (Bayer AG, Leverkusen, Germany). The PCO2, a–et difference (ΔPCO2, a-et) was calculated from these data for each piglet. Cardiac output, PCO2, a carot, and SO2, a carot were measured at 5-minute intervals. PCO2, et and Pa pulm were recorded continuously for Group 3 during the repeated embolisms and are presented as a combined image of our monitor. Data are presented as absolute values. Graphs were generated using GraphPad (La Jolla, CA) software (Prism 4).
Results
Basic data for the animals are presented in Table 1. Concentrations of hemoglobin, electrolytes, and glucose and body temperature were in normal age- and species-specific ranges throughout the whole examination. At the beginning of the embolism hemodynamic parameters were also within standard range.
In Group 1 (Fig. 1) two piglets died within 15 minutes after embolism. The surviving animal reached baseline values again within 1 hour, showing a continuous decrease in cardiac output with a very low value (<0.2 L/minute) at 20 minutes. Cardiac output of the other animals declined rapidly within 10 minutes. Heart rate stayed above 50 bpm in all animals for 10 minutes. The deceased animals showed an initial rapid decline of Pa carot, mean. Although piglet 2 showed a brief incline after 4 minutes, the values dropped to 0 after 15 minutes. This short increase is also detectable at about 4 minutes in fc, Pa pulm, mean, and PCO2, et. The surviving animal showed a constant decline of Pa carot, mean until 20 minutes. SO2, a carot stayed constant and showed a sudden drop after 10 minutes. The surviving animal had a constantly high SO2, a carot. The piglets showed an initial increase in Pa pulm, mean and decrease in PCO2, et. PCO2, a–et, indicating pulmonary dead space, increased about 11.3–21.6 mm Hg (Table 2).
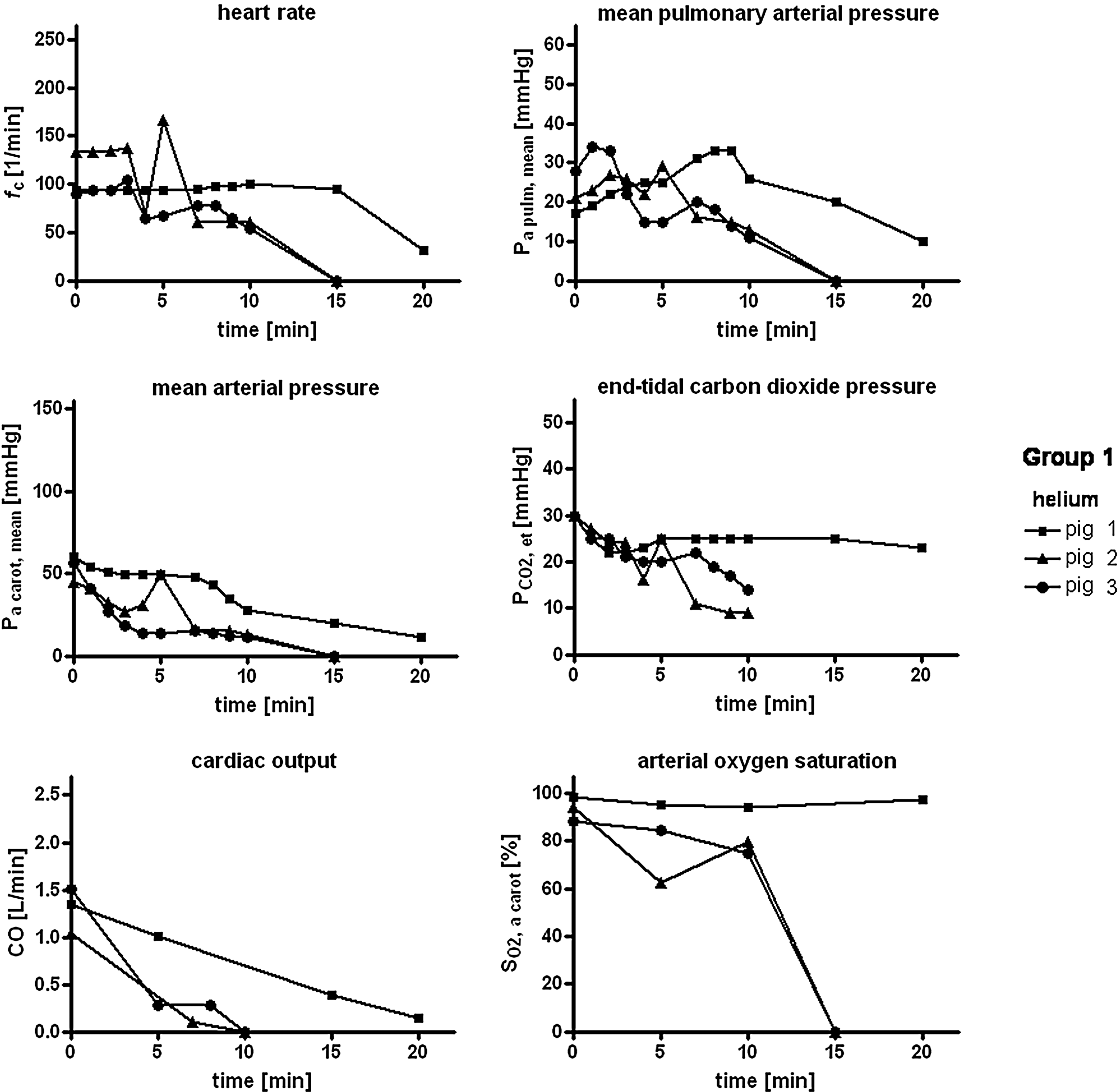
Parameters of Group 1. Presentation of the first 20 minutes after helium embolism. CO2, carbon dioxide; O2, oxygen.
Recompensation after embolism: asurviving piglet, PCO2, a–et=5.4 mm Hg at 40 minutes; bsurviving piglet, PCO2, a–et<6 mm Hg at 30 minutes; cmaximum PCO2, a–et=10 mm Hg at 10 minutes, PCO2, a-et<6 mm Hg at 40 minutes.
CO2, carbon dioxide; He, helium; PCO2, a–et, arterial to end-tidal CO2 pressure.
In Group 2 in order to compare the parameters intra-individually after embolism with CO2 and helium, the shown 20-minute measuring period commencing from embolism was depicted one above the other (Fig. 2). All three animals survived CO2 embolism, whereas two animals died after the following helium embolism after 6 and 15 minutes, respectively. After 60 minutes the surviving animal reached baseline values again. Following CO2 embolism the animals reached baseline values again even after 10 minutes with the exception of one animal that required 40 minutes. Heart rate, Pa carot, mean, cardiac output, and SO2, a carot showed no relevant changes upon CO2 embolism. In contrast, with one exception, fc and Pa carot, mean decreased rapidly after helium embolism. A further decline in arterial blood pressure was compensated for by a slight increase in fc, until there was a sudden decline in fc and Pa carot, mean shortly before death (Fig. 2). Cardiac output and SO2, a carot only showed a distinct decrease after helium embolism (Fig. 2). CO2 led to a rapid increase in Pa pulm, mean in all animals. The following helium embolism showed the same effect in two animals. The animal that died 6 minutes after helium application did not show such an increase. Every embolism was also followed by a rapid decline in PCO2, et. Initial values in two piglets for Pa pulm, mean and PCO2, et after CO2 embolism were reached again after 20 minutes (Fig. 2) and in one piglet after 40 minutes. One piglet survived helium embolism (Fig. 2). The surviving animal reached baseline parameters again within 1 hour. PCO2, a–et increased about 10.5–13.9 mm Hg after CO2 embolism and about 20.8–51.0 mm Hg after the following helium bolus (Table 2).

Parameters of Group 2. Presentation of the first 20 minutes after each embolism. Values after carbon dioxide (CO2) embolism are shown in open gray symbols followed by helium (He) embolism shown in solid black symbols.
In Group 3 the effects of alternating CO2 and helium embolisms at 15-minute intervals on Pa pulm, mean and PCO2, et are demonstrated in one single piglet (Fig. 3). Before each embolism the parameters were within the standard range. Administration of 3 mL of helium was followed by a notably greater decrease in PCO2, et than after each administration of 9 mL of CO2. Similarly, Pa pulm, mean showed a more rapid and stronger increase after 3 mL of helium than after the initial CO2 embolism. Subsequent CO2 embolisms of 9 mL led to a distinctly weaker increase in Pa pulm, mean each time. A 9-mL helium embolism resulted in the most pronounced reaction. After the final embolism of 9 mL of CO2 there was hardly any reaction in PCO2, et and Pa pulm, mean.
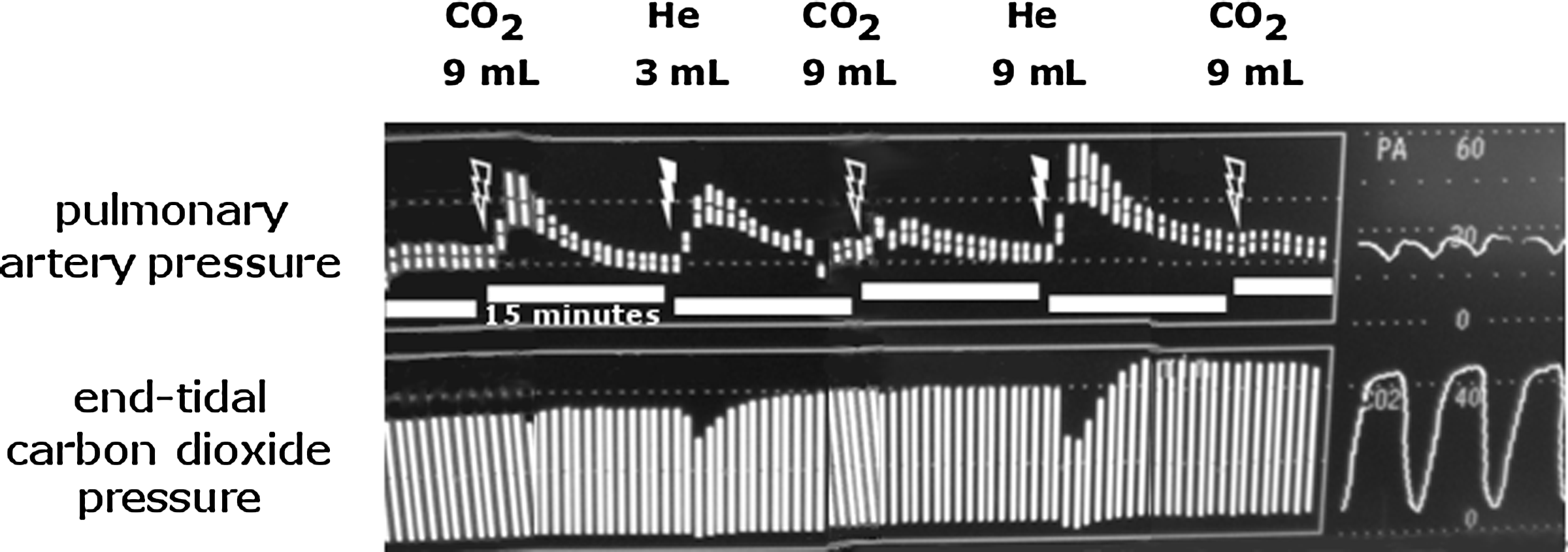
Combined monitor image of Piglet 7. Repetitive embolisms of carbon dioxide (CO2) and helium (He) are alternated in 15-minute intervals. Flashes mark the starting points of the administrations of the embolisms.
Discussion
The porcine model was chosen because of its comparability in cardiovascular reactivity with respect to humans. We used 5–6-week-old pigs as a model for pre-teenage children. According to Rendas et al., 23 such a comparative definition is given because of the known timespan that it takes for pigs to develop a mature cardiopulmonary system. The comparison is, for example, based on the alveolar number that reaches maturity in pigs within 12 weeks compared with humans with 8 years. The definition is furthermore based on the development of the pulmonary vasculature and the left-ventricular predominance seen in pigs. 23
What are the characteristics of helium as an insufflation gas? It can be used in laparoscopy in order to avoid local peritoneal acidosis 24 with a subsequent higher rate of metastasis seen with a capnoperitoneum. Furthermore, it can prevent CO2 accumulation in respiratory diseases during anesthesia.1,2,6 In addition to metabolic CO2 production, a capnoperitoneum causes an intra-abdominal pressure-dependent CO2 load due to peritoneal resorption. Helium is well established in other medical branches. 10 It is the most inert gas. The Oswald solubility coefficient of helium in plasma at 37°C is given as 0.0086 mL of helium/mL of plasma. 9 For CO2 it is 0.5195 mL of CO2/mL of plasma, which is a 60-fold difference. 8 Laparoscopy with helium also offers the advantages of a pneumoperitoneum without the inherent metabolic disadvantages of CO2. Meta-analysis for different insufflation gases revealed only small changes in cardiopulmonary functions.4,5 Argon caused a decrease in the cardiac output and an increase in the systemic vascular resistance of up to 30%, 25 whereas helium, nitrogen, and air showed even less changes in this respect.4,5 Nitrous oxide (N2O), a soluble gas with an additional analgesic effect, is inappropriate when using electric cautery because of its high explosiveness. 26 Therefore, the difference between various insufflation gases consists mainly of the potential effects of an intravascular gas embolism.
There was a prompt reaction (i.e. a decrease in PCO2, et and an increase in Pa pulm) after direct embolism with CO2 and helium (Fig. 2). However, the reactions after helium embolism were more pronounced (Figs. 1 and 2). Pa pulm decreased suddenly because of cardiopulmonary decompensation immediately after the embolism in piglet 6 (Fig. 2). The difference between CO2 and helium embolism was most noticeable in the decrease in cardiac output (Fig. 2). There was almost no change in cardiac output after CO2 embolism. However, it decreased drastically after helium embolism (Figs. 1 and 2), and only one animal was able to recompensate (Fig. 2, piglet 4).
The mean arterial pressure also showed a rapid decline after helium embolism, whereas Pa carot, mean decreased moderately after CO2 embolism followed by recompensation. The heart rate remained almost unchanged, in contrast to bradycardia appearing after helium embolism (Figs. 1 and 2). Only one animal initially decreased slightly in Pa carot, mean with a constant fc (Fig. 2). Oxygenation also changed slightly after CO2 embolism but decreased markedly after helium embolism (Figs. 1 and 2). The chronological order of changes in the parameters matches the results of Jersenius et al. 27
Both gases led to simultaneous changes in PCO2, et and Pa pulm (Fig. 2). However, the impact of CO2 embolism was clearly attenuated because of rapid CO2 utilization from the site of administration to the pulmonary vascular bed. This is confirmed by multiple repetitive applications of the two gases in piglet 7 (Fig. 3). The decrease in PCO2, et after helium embolism was more pronounced than after CO2 embolism despite a threefold increase in gas volume. A less distinct PCO2, et and Pa pulm reaction after repetitive CO2 embolisms was noticeable in all cases (Fig. 3).
A helium embolism causes a much higher increase in the ventilatory dead space with pulmonary vascular closure than a CO2 embolism of the same volume (Table 2). This study showed a less increasing PCO2, a–et after CO2 embolism compared with a helium embolism. It is furthermore noticeable that administration of a helium embolism after a CO2 embolism in spite of a preceding recompensation period led to the most pronounced increase of PCO2, a–et.
It must be borne in mind not only that CO2 is physically more solven in the plasma,8,9 but also that carbonic anhydrase converts 16.2 mmol of CO2/L of blood to hydrogen carbonate and that CO2 is stored intraerythrocytically as well as in the tissue. Such CO2 utilization after intravascular entry counteracts CO2 accumulation in the lungs. The gas bubbles shrink during their passage. 28 This results in smaller vessels being occluded within the pulmonary system than it would be the case with helium bubbles. Hence, a CO2 embolism leads to a considerably smaller increase in dead space than a helium embolism. Therefore, a helium embolism is similar to an air embolism in which the pulmonary gas thrombus is not resorbed, but is converted into a steady thromboembolism via endothelial adhesion and granulocytic aggregation. 29 Such an attempt at an explanation may be reasoned further. According to this line of thought, there is still a CO2-mediated vasoconstriction in spite of a recompensation period. Hence a helium bubble of the same diameter may occlude more arterio-alveolar units. Without such a vasoconstriction the bubble would have reached more peripheral units. In this context one also has to bear in mind that an immature extension of the pulmonary vasculature leads to even more serious increases in alveolar dead space.23,30
A single study in the literature that compares CO2 and helium embolisms intra-individually does not mention hemodynamic parameters, but reports the survival of all four dogs after 5–10 mL/kg CO2 embolism with subsequent death after helium embolism using the same dosage. 21
In addition to the gas type, the velocity of administration is important. Roberts et al. 11 administered 1.5 times the amount of gas that was used in our study to large pigs over a period of 30 minutes. The soluble gases CO2 and N2O did not alter Pa pulm and PCO2, et. Argon and helium did lead to a distinct decrease in the PCO2, et, parallel to an increase in the PCO2, art with consecutive major acidosis and tachycardia. Rudson-Brown et al. 19 administered repetitive CO2 or helium embolisms as a bolus. These pigs survived CO2 embolisms of 10 mL/kg and died after helium embolisms of 2.5–5.0 mL/kg. Similarly, their animals showed a rapid decrease in the PCO2, et and oxygenation. They did not exhibit a decrease in Pa carot, mean until higher dosages. 19
Because helium is not approved as an insufflation gas in all countries, also other inert gases such as argon are used as an alternative in special situations. 31 Sharing the same physical properties inert gases also share the same risks. 9
Especially in small individuals, a vascular puncture plays an important role, for even the smallest amounts of gas may lead to fatal consequences. After 2 seconds at an insufflation speed of 1 L/minute a gas volume of 30 mL has already been insufflated. The brevity of the time interval prevents virtually any adequate response by the surgeon. In light of these considerations, the present study involved administering an embolism of 2 mL/kg via direct venous gas injection.
Conclusions
Although there are numerous reports regarding the use of helium as an alternate insufflation gas to CO2, its use is limited to special indications such as laparoscopic tumor surgery. If helium is used, one has to keep in mind that helium embolisms of even the smallest amounts of up to 2 mL/kg have a lethal impact immediately after venous puncture. The trocar should be placed openly. Additional monitoring (e.g., via transesophageal echocardiocarphy or precordial Doppler ultrasound) as well as preoperative exclusion of a patent foramen ovale should be taken into consideration.
Footnotes
Disclosure Statement
No competing financial interests exist.