
Abstract
Abstract
Objective:
To evaluate the routine use of the vacuum bell for elevating the sternum during minimally invasive repair of pectus excavatum (MIRPE) (the Nuss procedure).
Subjects and Methods:
This was a retrospective evaluation of a prospective database including all patients who underwent MIRPE at our institution between 2005 and 2010. Data included the patient's demographic characteristics, age at surgery, gender, Haller index, duration of surgery, and intraoperative complications.
Results:
Fifty patients from 9 to 28 years old (average, 14.95 years) were observed, including 39 males and 11 females. The preoperative Haller index was between 3.25 and 7.4 (average, 5.05). Mean duration of surgery was 58 minutes (range, 45–92 minutes). The use of the vacuum bell led to a clear elevation of the sternum as confirmed by thoracoscopy. Advancement of the pectus introducer and placement of the pectus bar were safe, successful, and uneventful in all patients. No cardial and/or pericardial lesion was noted as well as no lesion of the mammary vessels.
Conclusions:
The intraoperative use of the vacuum bell during the MIRPE is safe and effective as it facilitates the retrosternal dissection and the insertion of the pectus bar. If available, we recommend the routine use of this device for MIRPE.
Introduction
The procedure of applying a vacuum to elevate the sternum was first used more than 100 years ago. 14 Despite the risks and unsatisfactory results after operative therapy for some patients, there has been little progress in the therapeutic use of vacuum therapy during the last few decades. In 2003, we commenced conservative treatment of pectus excavatum using the vacuum bell. Our preliminary experience on a group of 34 patients demonstrated encouraging results using the vacuum bell for conservative treatment of pectus excavatum in selected patients. 15 Additionally, Schier et al. 16 as well as we 15 reported for the first time on the off-label intraoperative use of the vacuum bell to elevate the sternum during the MIRPE procedure. After informed consent of the parents and approval by the institutional review board, we started to use the vacuum bell during MIRPE routinely.
Subjects and Methods
The technique and use of the vacuum bell for conservative treatment of pectus excavatum are described elsewhere.15–17 Our preliminary experience encouraged us to use the device intraoperatively to facilitate the dissection of the transmediastinal tunnel and the advancement of the pectus introducer, the riskiest step of the procedure. When creating the vacuum, the elevation of the sternum is obvious, as demonstrated first by Schier et al., 16 and persists for a distinct period of time. Therefore, we considered that the vacuum cup may also be useful in reducing the risk of injury to the heart and the mammary vessels during the MIRPE procedure, as described first by Schier et al. 16 The device might also be applied for placement of the pectus bar. Because the manufacturer of the device does not have a license for sterilization of the vacuum bell, this additional use had to be considered as “off-label.” In agreement with our hospital hygienist and bearing in mind the nature of the material, we used gas sterilization for preparation of the device for intraoperative use. Three different sizes of the vacuum bell exist, as described previously.15,17 The diameter is 16 cm for the small model, 19 cm for the medium-size model, and 26 cm for the large model. The medium-size model is available in a supplemental version with a reinforced silicon wall (e.g., for adult patients with a small deep pectus). The appropriate type and model of the device were determined according to the individual patients' chest wall size.
Results
The surgical technique that we used is described in detail elsewhere.1,18 Surgery was indicated if the patient had a severe pectus excavatum based on clinical examination as well as Haller index greater than 3.2. From 2005 to 2010, 50 patients from 9 to 28 years old (average, 14.95 years; 39 males and 11 females) were operated on for pectus excavatum. Thirty-eight patients underwent primary surgery. Twelve patients (11 male, 1 female) used the vacuum bell for a period of 4–36 months (average, 19.9 months) before surgery and discontinued the application because of decreasing motivation and/or insufficient success. The preoperative Haller index was between 3.25 and 7.4 (average, 5.05). The duration of surgery averaged 58 minutes (range, 45–92 minutes). The vacuum bell was applied for retrosternal dissection and advancement of the pectus introducer (Fig. 1) as well as placement and flipping of the pectus bar. The use of the vacuum bell led to a clear elevation of the sternum, and this was confirmed by thoracoscopy (Fig. 2). Advancement of the pectus introducer and placement of the pectus bar were safe, successful, and without adverse events in all patients. No evidence of cardiac and/or pericardiac lesions or lesions of the mammary vessels was noted intraoperatively by using right-sided thoracoscopy. Additionally, no midline incision to elevate the sternum with a hook was necessary.
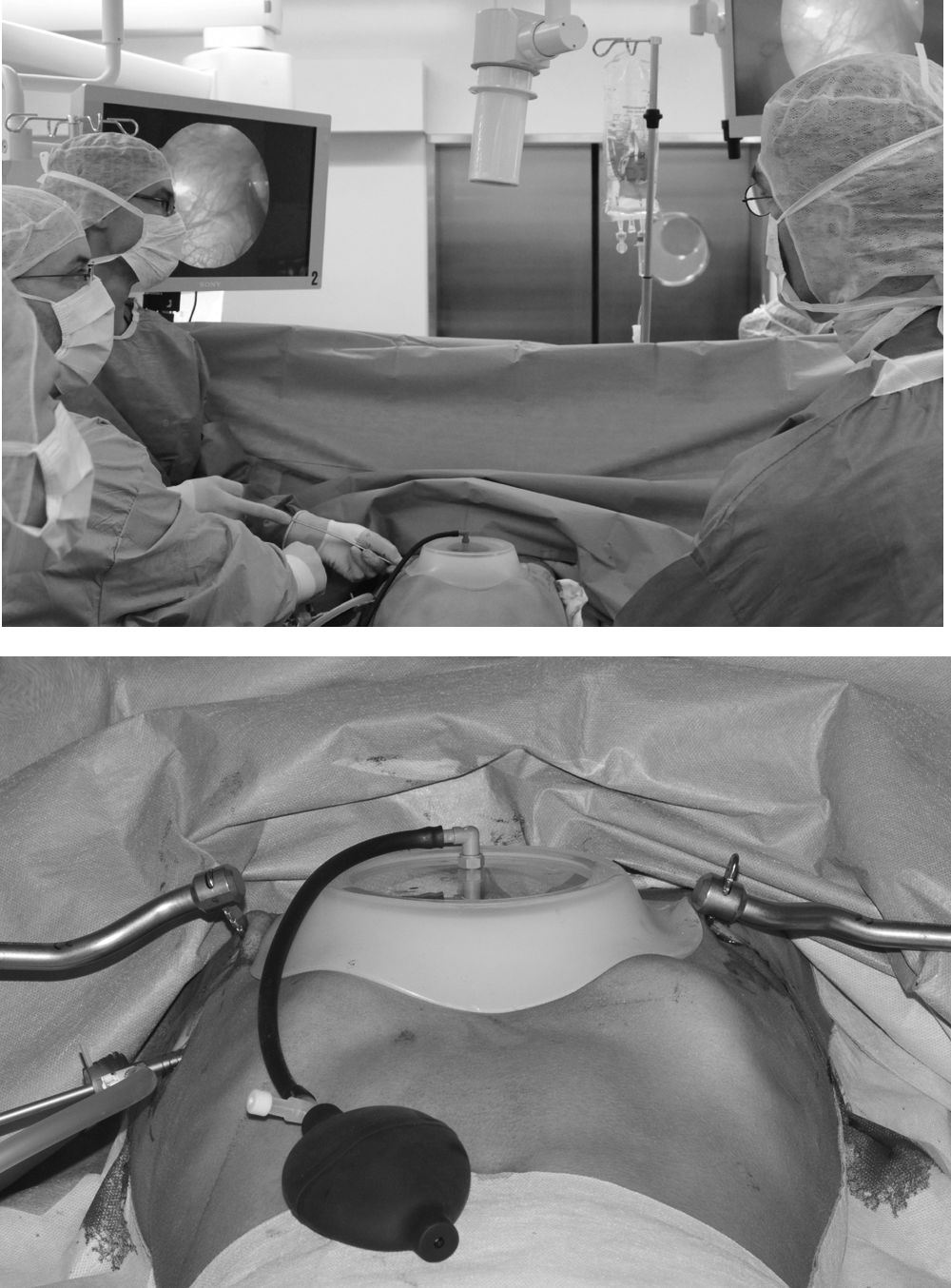
Intraoperative application of the vacuum bell.
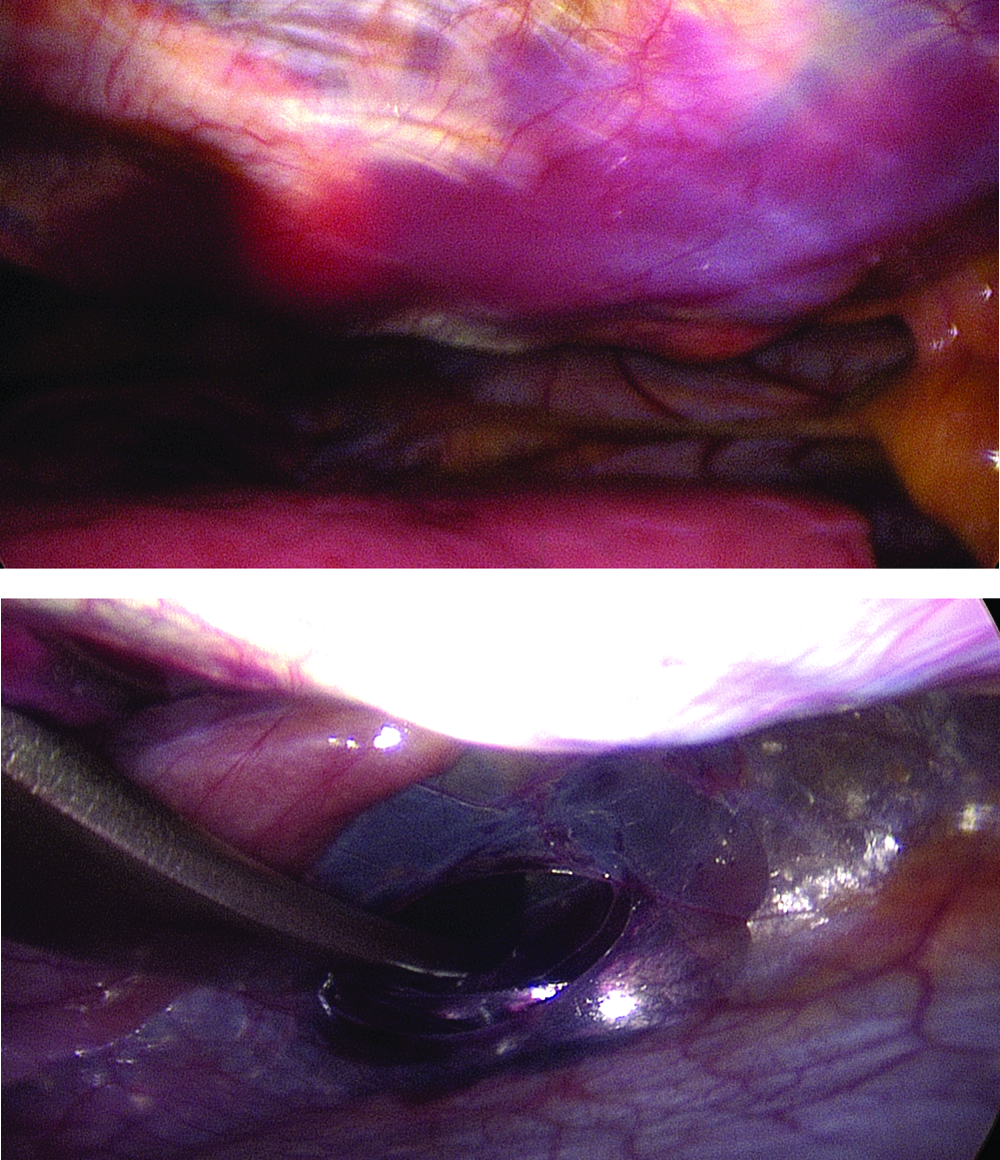
Thoracoscopy during application of the vacuum bell.
Three patients complained about chest pain within postoperative Days 1–4. The electrocardiogram and echocardiography revealed no evidence of cardiac lesion in these patients, and symptoms disappeared spontaneously. The overall duration of clinical follow-up was 12–84 months, and it was uneventful for all patients. Pectus bar removal was performed 3 years after pectus repair.
Discussion
With the introduction of the MIRPE, the number of patients presenting for surgery has increased dramatically. 18 However, with the widespread use of the MIRPE procedure the character and number of complications have increased, and there is an increasing number of near-fatal complications.2,3,5–13 During the MIRPE procedure, the riskiest step of the procedure is the retrosternal dissection and the advancement of the introducer between the heart and sternum. When the vacuum bell is used to create the vacuum, the elevation of the sternum is obvious and persists for a distinct period of time. As demonstrated in the computed tomography scan, the force of the vacuum bell is strong enough to deform the chest within minutes, even in adolescent and adult patients. 16 Therefore, the vacuum bell may also be useful in reducing the risk of injury to the heart and the mammary vessels. The use of gas sterilization prepares the device for intraoperative use, and this is in accordance with the guidelines of our hygienist.
The results of our present study show that the intraoperative use of the vacuum bell during the MIRPE procedure is safe and effective and facilitates the introduction of the pectus bar. In no case was a cardiac and/or pericardiac lesion or a lesion of the mammary vessels observed. Additionally, no midline incision to elevate the sternum with a hook was necessary. If available, we recommend the use of this device for the routine performance of the MIRPE procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.