
Abstract
Abstract
Background:
Live case demonstrations (LCDs) represent a common educational method throughout most surgical specialties. Concern has been raised about ethics and patient safety. The surgeon's elevated stress level, the need to comply with the meetings' time schedules, unfamiliar surgical equipment, and questionable indications resulted in prohibition of LCD in some surgical societies. We aimed to investigate the opinion of International Pediatric Endosurgery Group (IPEG) members on LCD.
Materials and Methods:
An online-based survey in 2010–2011 requested all IPEG members to complete a questionnaire including data on personal background and statements on LCD. Participants had to indicate agreement with statements on a scale from 1 (do not agree) to 5 (fully agree).
Results:
Sixty-one surgeons and 148 attendees completed the questionnaire. Eighty-three percent of surgeons indicated elevated stress levels during LCD. Surgeons (3±1.2) and attendees (3±1.4) agreed that LCD may be harmful. Surgeons (2±1.2) and attendees (2±1.3) disagreed that LCD may be beneficial for patients. However, LCD was rated as educationally essential by surgeons (3±1.3) and attendees (3±1.3). Surgeons agreed (3±1.2) that educational benefits of LCD outweigh disadvantages for patients; attendees did not agree (2±1.3). Surgeons (4±1.4) and attendees (3±1.4) agreed that LCD should continue. Nevertheless, 36% of surgeons and 52% of attendees would not consent for LCD in their own child.
Conclusions:
LCD is regarded an essential part of surgical education by IPEG members. However, it represents a controversial topic. The majority of IPEG members appear willing to continue LCD. If IPEG decides to go on with LCD, attention has to be drawn to patient safety and ethical considerations.
Introduction
Little is known about the experience of performing surgeons during LCD and the perspective of attendees of LCD procedures during surgical meetings. The aim of this study was to investigate the experience and opinion of the members of the International Pediatric Endosurgery Group (IPEG) with regard to LCD.
Materials and Methods
An Internet-based survey on LCD was designed and conducted on behalf of the IPEG Research Committee. The Webpage http://livesurgery.survey-center.com was launched on December 7, 2010 and closed on January 31, 2011. All IPEG members were invited to participate in the survey by e-mail, using the recent general mailing list of the IPEG office. Based on the assumption that IPEG faculty members were more likely to be involved in LCD as performing surgeons, all faculty members were separately invited to participate by personal e-mail. IPEG members willing to participate clicked on an embedded link in their e-mail to connect to the survey. Three reminder messages were sent during the 7-week period using the same mailing lists.
The survey consisted of two different branches: one for the performing surgeons during LCD and one for attendees of LCD. A switch was integrated into the survey to ensure adequate questions for both groups. No unique personal identifiers were collected from participants to encourage respondents to be candid in their responses.
The first part of the survey comprised six questions to ascertain professional background of the respondent. The second part of the survey consisted of questions and statements to delineate the respondent's opinion about LCD during surgical meetings and the ethical issues arising.
Surgeons were asked to indicate their subjective stress level during LCD and to name any examples of harmful events for the patient during LCD from their own experience. For the remaining nine statements on LCD, the agreement or disagreement had to be indicated on the following scale: 1 (I fully disagree), 2 (I do not agree), 3 (I agree), 4 (I strongly agree), and 5 (I fully agree).
Attendees were also asked to indicate any examples of harmful events for the patient during LCD from their own experience and give their agreement or disagreement with 10 statements on LCD on the aforementioned scale.
Software for data analysis was provided by the company in charge of the survey's Website (MeineUmfrage.com, Heidelberg, Germany). Only complete datasets were included in the study. Incompletely answered datasets or datasets sent from the same Internet protocol address were excluded from further analysis. Data are quoted as median scores and standard deviation on the agreement scale. A median score of ≥3 was considered as agreement, and a median score of <3 was considered as disagreement with the statement.
Results
Two hundred nine datasets were completed and included in our study: 61 respondents completed the dataset for performing surgeons during LCD, and 148 respondents completed the dataset for attendees during LCD. The data on the professional background of respondents are summarized in Table 1 for performing surgeons and Table 2 for attendees.
Eighty-three percent of performing surgeons stated they had elevated mental stress levels during operating in LCD compared with the usual setting in the work environment of their home department (61% moderately, 18% highly, and 5% extremely elevated compared with their usual setting). Twenty-five percent of respondents in both groups were aware of events during LCD that were harmful for the patient. Many comments in the free-text option indicated a suspected potential connection of the adverse events with LCD. Some respondents referred to the same events they experienced during one particular demonstration (Table 3).
LCD, live case demonstration.
In the two different branches of the survey, performing surgeons and attendees were asked to indicate their agreement to given statements on LCD. LCD was rated as absolutely essential for educational purposes in pediatric surgery by both surgeons (3±1.3) and attendees (3±1.3). Surgeons agreed with the statement that no other educational method can replace LCD for minimally invasive pediatric surgery (3±1.4). Attendees did not agree with this statement (2±1.4). However, LCD was strongly regarded as having a high impact on their surgical skills and everyday work by attendees (4±1.2).
Both groups disagreed with the statement that LCD is beneficial for the individual patient who is operated on (surgeons, 2±1.2; attendees, 2±1.3). Both surgeons and attendees agreed with the statement that LCD may be harmful for the patient (surgeons, 3±1.2; attendees, 3±1.4). Surgeons agreed with the statement that the benefits of LCD in surgical education outweigh the possible disadvantage for the patient (3±1.2). Attendees did not agree with this statement (2±1.3) (Fig. 1).

Agreement with given statements on LCD on a scale from 1 (I fully disagree) to 5 (I fully agree). Performing surgeons, n=61; attendees, n=148.
Both surgeons (4±1.4) and attendees (3±1.4) agreed that LCD should continue to be part of surgical meetings. And, both groups disagreed with the statements that LCD should generally be discontinued (surgeons, 2±1.3; attendees, 2±1.4) and that LCD is ethically wrong (both groups, 2±1.2). Only performing surgeons agreed with the statement, “If my child required an operation, I would consent to have Live Surgery done in my child” (3±1.4). Attendees did not agree with this statement in median (2±1.7). In detail, 36% of surgeons and 52% of attendees would not agree to consent for LCD in their own child (Fig. 2).
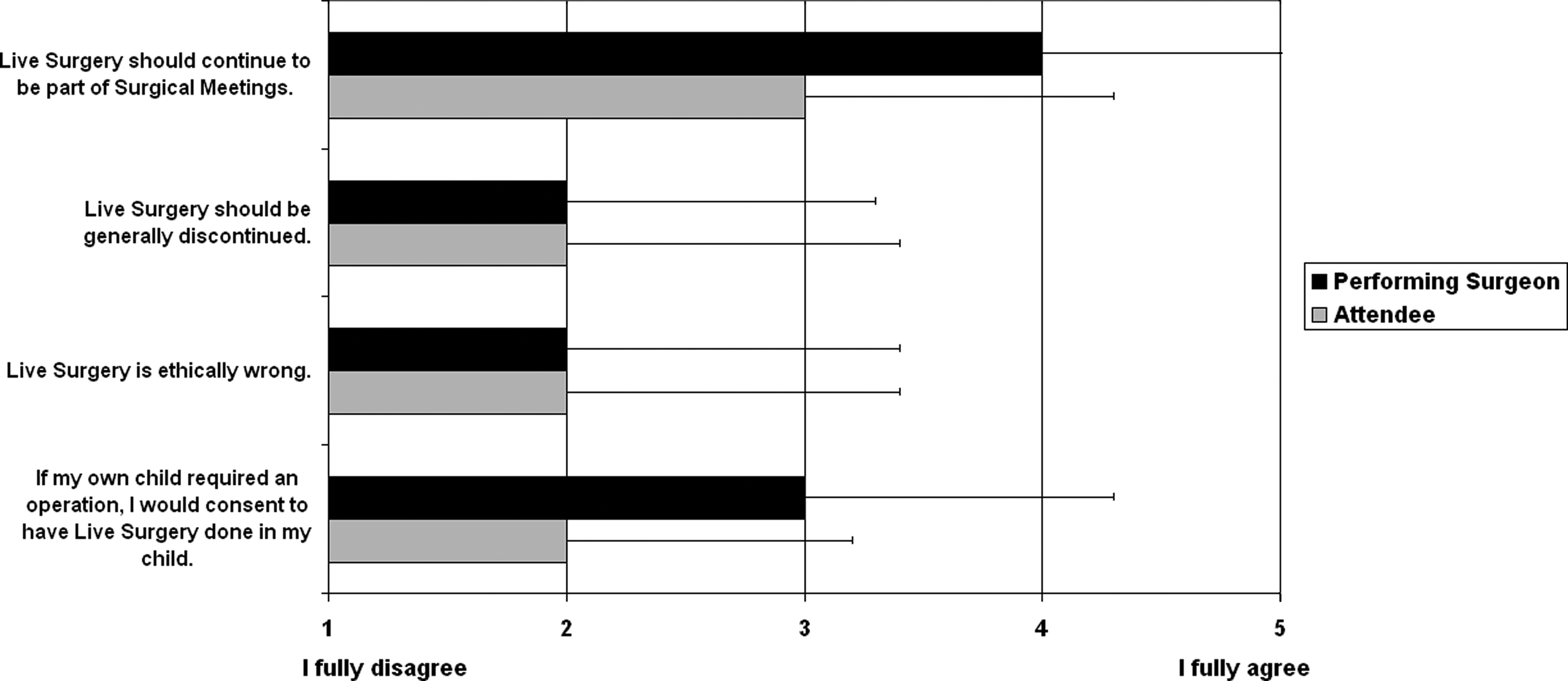
Agreement with given statements on LCD on a scale from 1 (I fully disagree) to 5 (I fully agree). Performing surgeons, n=61; attendees, n=148.
Discussion
Surgical education is based on an apprenticeship structure, and the fact that surgical procedures are performed under the observation of trainees is probably as old as surgery itself. Compared with the regular setting of a few trainees present, listening and discussing in a quiet operation theater, LCDs during surgical meetings obviously flows differently. The performing surgeon during LCD is wired with communication devices, watched by a huge audience that may want to discuss the case from the comfort of their seats. The surgeon might be faced with an unfamiliar environment, equipment, theater, and anesthetic staff and the expectation to stay on a time schedule. The potential risk that these unique circumstances might expose the patient to higher likelihood for complications has brought up an ongoing discussion about the ethics of LCD.
It has been shown for live demonstrations of endoscopic retrograde cholangiopancreatography that treatment during LCD is different from the treatment of a non-LCD control group. 5 The study included 168 patients undergoing live endoscopic retrograde cholangiopancreatography. The treatment of the LCD group was significantly delayed because of the timing of the LCD conference, the use of general anesthesia for the procedure was significantly higher, and the interventionalists' tendency toward taking shortcuts to limit procedural duration was observed. 5 Another recent study on live endoscopic retrograde cholangiopancreatography including 406 live cases clearly showed significantly lower success rates of the procedure compared with controls. 6 Even though complication rates of LCD groups were not different compared with controls in both studies,5,6 these data suggest that the quality of treatment in LCD is degraded rather than enhanced.
Objective data on surgical LCD are scarce. However, even the potential risk of not providing the best possible treatment to a patient undergoing LCD may not be acceptable. Dr. William J. Mayo, founder of the Mayo Clinic, said, “the best interest of the patient is the only interest to be considered.” In keeping with these values, different authors have suggested prohibiting LCD completely.3,4,7 This opinion has been adopted by various surgical associations such as the American College of Obstetricians and Gynecologists, the American College of Surgeons, the American Association for Thoracic Surgery, and the Society of Thoracic Surgeons, which have banned LCD from some or all of their meetings. 4 Various other interventional societies chose to recommend adherence to a recently published code of conduct, strictly regulating LCD with regard to ethical considerations. 8 Particularly in the light of advancing simulation technologies improving the skills of surgeons and interventionists without patient exposure, and thus offering an attractive alternative to LCD, it has to be carefully considered whether or not LCD should be the favored educational method.3,9
Sugarman et al. 10 recently chose an approach similar to ours to investigate the opinion of performing operators/interventionalists and attendees during LCD. They conducted a survey including the participants of Vascular Interventional Advances meetings serving as faculty or attendant professionals during LCD meetings in two consecutive years (2009–2010). They came to results similar to ours. For most of the respondents, observing LCD was more valuable than watching an edited video. About one-third of respondents thought that LCD patients are exposed to more risk than non-LCD patients. However, in their survey, the majority of respondents indicated that they would support the decision of a family member to be an LCD patient, and few indicated that they personally would agree to be an LCD patient. 10
The results of our survey add further insights into the feeling about LCD. Conducting a survey on LCD in the largest international society for minimally invasive pediatric surgery, we are able to give a representative statement on pediatric LCD. Our results clearly show that members of IPEG regard LCD as an essential part of surgical education. However, LCD does represent a controversial topic among both performing surgeons and attendees during LCDs in pediatric surgery. The majority of the IPEG community appear willing to continue LCD during pediatric surgical meetings. If IPEG decides to go on with LCD, our attention has to be drawn to patient safety issues and ethical considerations in this field. We strongly recommend establishing an ethical code of conduct for LCD following the existing versions of other societies, but adapted for pediatric sugery.
Footnotes
Acknowledgments
The authors would like to thank Jennifer Clark, Executive Director of IPEG, for her outstanding help with all administrative issues. We thank Marten Bökamp, Senior Consultant at ![]() , Heidelberg, Germany, for expert assistance with the Web design of this survey. The survey was financed by a research grant of the Hannover Medical School, Hannover, Germany.
, Heidelberg, Germany, for expert assistance with the Web design of this survey. The survey was financed by a research grant of the Hannover Medical School, Hannover, Germany.
Disclosure Statement
No competing financial interests exist.