
Abstract
Abstract
Introduction:
About 0.2–10% of patients with prior orchiopexy will require reoperation for recurrent cryptorchidism. The most common approach for these patients has been an open inguinal repeat orchiopexy. The aim of this report is to show results and feasibility with the totally laparoscopic approach for failed prior open orchiopexy.
Subjects and Methods:
Nine patients with 11 recurrent undescended testes were treated by the totally laparoscopic orchiopexy approach. We used a four-port technique, starting with laparoscopic dissection of the vas deferens and spermatic vessels as high as possible in order to get adequate length of these structures. The inguinal internal ring was opened, and the testis was dissected to finally bring it into the abdominal cavity. A transcrotal trocar was introduced all the way to the abdominal cavity to finally pull through the testis into the scrotum.
Results:
Laparoscopic orchiopexy was performed satisfactorily in all but 1 case in a mean time of 90 minutes. We did not experience any perioperative complications. In a mean follow-up of 25 months there has not been any recurrent cryptorchidism or atrophic testis.
Discussion:
Laparoscopy offers the advantage of achieving an extensive mobilization of spermatic vessels and a careful dissection of the vas deferens. The totally laparoscopic approach for a failed orchiopexy represents a feasible, safe, and successful procedure.
Introduction
Numerous surgical techniques have been described with different success rates; however, the open inguinal approach has been traditionally the standard of care. The success rate has been reported to range from 88.6% to 100%. 2 A large retrospective report of 8425 undescended testes found that the success rate was related to anatomical testicular position as follows: 74% for abdominal testes, 82% for peeping testes, 87% for canalicular testes, and 92% for testes located beyond the external ring. 3 It was also found that different surgical techniques had different success rates.
It has been reported that up to 0.2–10% of the patients will require reoperation for recurrent cryptorchidism.4–6 Reoperations of the inguinal area represent a technical challenge requiring advanced skills and anatomical knowledge. The most common approach for these patients has been an open inguinal repeat orchiopexy. 7 Reoperation through the same approach has the potential high risk of injury to the vas deferens and spermatic vessels because of extensive scar tissue. There have been some reports of difficult undescended testes or repeat orchiopexy that have been operated on with the aid of laparoscopic mobilization of testicular vessels; however, an inguinal incision is still being performed.8–10 The aim of this report is to show the results and feasibility with the totally laparoscopic approach for failed prior open orchiopexy.
Subjects and Methods
Between 2001 and 2010, 9 patients with 11 recurrent undescended testes underwent a totally laparoscopic repeat orchiopexy in Monterrey, Mexico. All of the patients had a prior conventional orchiopexy performed by another surgeon, and previous clinical information or surgical details were unavailable for all of the patients. Two of the patients had had three prior unsuccessful orchiopexies. The mean age of the patients at the time of the reoperative surgery was 5.5 years (range, 2.5–6 years). Preoperative physical examination found six testes located at the external inguinal ring (supra scrotal) and five testes within the inguinal canal. There was no need to perform an imaging study because all testes were palpable. Follow-up was achieved with regular office visits, physical examination, and scrotal ultrasound. Success was defined by physical and ultrasonographic examination as achieving a bottom scrotal position of the testis with an adequate size and lack of testicular atrophy.
Operative technique
Surgical technique followed the same principles and was similar in all patients. The objective was to perform an adequate laparoscopic dissection/mobilization of the vas deferens and spermatic vessels until an adequate length was obtained. General anesthesia and a urinary catheter were used on all the patients. Pneumoperitoneum of 8–10 mm Hg was established with the Veress technique. A four-port technique was used with a 4-mm 45° scope and 2–3-mm instruments. A 5-mm umbilical trocar was used for the scope and bilateral flank 2–3-mm working ports. The forth trocar was a 5- or 10-mm trans-scrotal trocar used at the end of the surgery to descend the testis. Visualization of the abdominal cavity was performed followed by incision of peritoneum at the internal inguinal ring in a circumferential manner. Figure 1 shows the laparoscopic view of vas deferens and spermatic vessels in a patient with a prior bilateral failed orchiopexy.
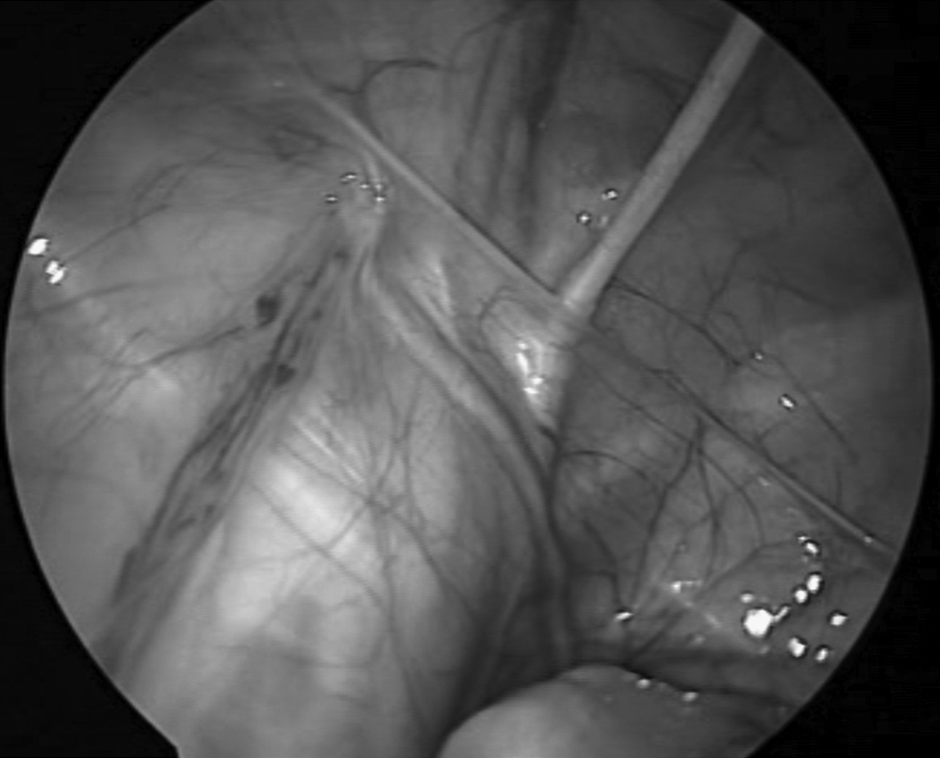
Laparoscopic view of vas deferens and spermatic vessels in a patient with a prior bilateral failed orchiopexy.
Following this, laparoscopic dissection of the vas deferens and spermatic vessels was performed as high as possible in order to get adequate length of these structures. To perform an adequate surgery it was indispensible to have extensive mobilization of the cord structures without harming vasculature that could cause testicular atrophy. Testis dissection was performed carefully. The inguinal internal ring was opened in order to get access to the inguinal canal and dissect the testis from scar tissue to finally bring the testis into the abdominal cavity. Once the testis was in the abdominal cavity, the vas deferens and spermatic vessels were adequately dissected. Vas deferens dissection was performed using a special atraumatic grasper that has a groove on it for traction. Once adequate mobilization of vessels and vas deferens was achieved, a 5- or 10-mm trocar was introduced through the scrotum medially to the epigastric vessels, with special care taken to avoid bladder injury (the Prentiss maneuver) (Fig. 2). This maneuver has the objective of shortening the distance of the testes to the scrotum and has been traditionally used as an alternative for high undescended testis, repeat orchiopexy, or older patients in whom the inguinal canal have been anatomically changed.11,12 Using the trans-scrotal trocar the testis was easily pulled down to the scrotum. Special care was taken to prevent torsion of cord structures. Finally, the testis was fixed with 5-0 polypropylene to the dartos and septum of the scrotum.
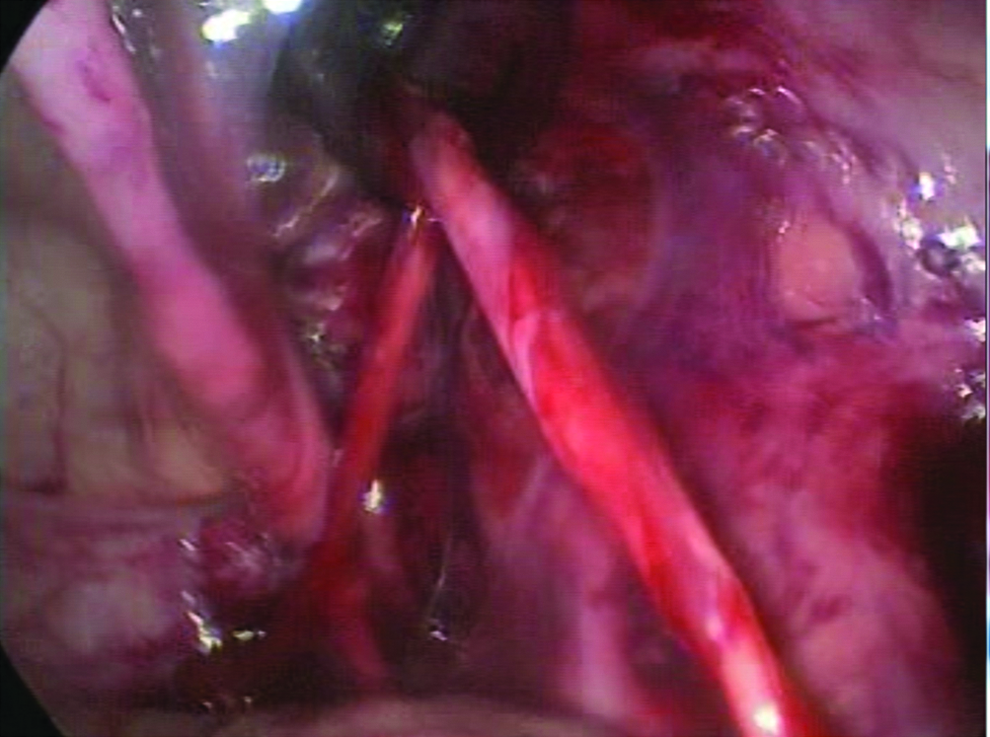
Laparoscopic Prentiss maneuver.
Figure 3 shows a patient with bilateral inguinal scars due to failed orchiopexies in which a totally laparoscopic approach was successfully performed. Adequate length of cord structures allowed easy traction of the testis to the scrotum.

Patient with bilateral inguinal scars due to failed orchiopexies in whom a totally laparoscopic approach was successfully performed.
Results
Eleven recurrent cryptorchidism cases were managed laparoscopically in 9 patients (2 bilateral). Surgery in 90% of the cases was performed successfully with a totally laparoscopic approach. One case had to be converted to an open conventional procedure because of extensive scar tissue found during inguinal dissection. It was also found that the vas deferens was adherent to the skin. During laparoscopy in 1 of the patients, we found that the affected side had a wide internal inguinal ring; however, physical examination did not find any bulging, and no further procedure was performed besides orchiopexy. The rest of the cases were performed satisfactorily in a mean time of 90 minutes (range, 140–70 minutes) with minimal blood loss. All procedures were performed in an ambulatory basis. Besides the case that was converted, we did not experience any perioperative complication.
Regular office visits were scheduled as follow-up for most of the patients for a mean interval of 25 months (range, 12–40 months). All patients had a regular follow-up for at least 1 year at 1, 3, 6, and 12 months after surgery. During follow-up, size and position of the testis were clinically evaluated. Besides physical examination, all patients were evaluated with testicular ultrasound to assess position, size, and vascularity. During this time there has not been any recurrent cryptorchidism or atrophic testis found during physical examination or ultrasound examination. All testes were found to be located low at the bottom of the scrotum. Finally, there were no inguinal hernias or hydroceles found during follow-up.
Discussion
This small retrospective series of cases represents a proposal for the treatment of recurrent cryptorchidism. Instead of performing a repeat anterior orchiopexy, we believe that laparoscopy may represent an advantage to treat these complicated cases. Similar to recurrent inguinal hernias, a posterior laparoscopic approach to the inguinal area represents an opportunity to work with less fibrotic and scar tissue. Laparoscopy offers the advantage of achieving an extensive mobilization of spermatic vessels and a careful dissection of the vas deferens all the way to the posterior wall of the bladder and retroperitoneum. Direct magnification of inguinal structures offers the opportunity to avoid any injury of these structures during dissection in the inguinal canal. Finally, the laparoscopic approach has the advantage of identifying and treating contralateral inguinal pathology or other genitourinary tract malformations.
Traditionally, recurrent undescended testes have been treated with conventional open repeat surgery. Cartwright and Snyder 13 have proposed a surgical technique that has been considered the gold standard for reoperative orchiopexy. They described a repeat inguinal approach with en bloc mobilization of the spermatic cord and extensive dissection of the proximal spermatic vessels with a success rate of 95%, although other series have reported a success rate from 80% to 100%. 14 On the other hand, Dudley and Docimo 14 have proposed Bianchi's high scrotal incision orchiopexy to treat undescended testicles in patients with prior groin surgery and iatrogenic cryptorchidism; this group reported a success rate of 95% with a high scrotal incision orchiopexy performed on 21 patients.
There have some reports in the literature regarding laparoscopic assistance for repeat orchiopexy.8,15 Leung et al. 8 published their experience in 18 patients with unpalpable and repeat undescended testis using a laparoscopic-assisted procedure. They performed what they called “laparoscopic mobilization of testicular vessels,” consisting of mobilization of testicular vessels to about 2 cm proximal to the internal inguinal ring; however, the rest of the procedure was performed with a standard inguinal approach. 8 Also, Tong et al. 15 reported 35 cases of patients with undescended testes with prior inguinal surgery who were treated with a laparoscopic-assisted orchiopexy with a success rate of 92%.
Regarding technical procedure, it is important to mention that we performed a modified laparoscopic Prentiss maneuver, which has not been reported previously for repeat laparoscopic orchiopexy. Theoretically, the Prentiss maneuver, besides decreasing the distance of the testis from the scrotum, straightens the angulation of the testicular artery, preserving blood flow to the testis and relieving tension on testicular vessels. 11 Increasing the length of cord structures and relieving tension constitute basic principles in any repeat orchiopexy, and we believe they are key factors to a successful repair.
All reoperative orchiopexies for failed conventional surgery are technically demanding procedures that require advanced laparoscopic skills. To date we have performed 144 laparoscopic orchiopexies for canalicular palpable testes (authors' unpublished data). This experience on treating cryptorchidism by laparoscopy has given us the expertise to perform reoperative inguinal surgery by laparoscopy.
Finally we believe that failure of conventional orchiopexy surgery is due to incomplete spermatic cord and inguinal canal dissection/mobilization. The laparoscopic approach offers the advantage of completing an extensive dissection that will result in lengthening of the spermatic cord structures and a successful procedure.
Conclusions
The totally laparoscopic approach for a failed open conventional orchiopexy represents a feasible and safe option to treat recurrent cryptorchidism. We have performed this procedure for recurrent cryptorchidism with an acceptable success rate. Finally, larger prospective and comparative series are still needed.
Footnotes
Disclosure Statement
No competing financial interests exist.