
Abstract
Abstract
Background:
There are many variable techniques for laparoscopic inguinal hernia repair in children. The aim of this study was to examine the feasibility of the laparoscopic hernia technique, which is based on the same surgical principles as conventional open herniotomy.
Subjects and Methods:
Between November 2008 and August 2011, 207 pediatric patients with inguinal hernia were included in this study under informed consent. All of the patients underwent the laparoscopic technique of sac transection and intracorporeal ligation. An asymptomatic contralateral patent processus vaginalis (cPPV) was repaired using the same method. Patients were routinely followed for 2 years. Perioperative complications and recurrence rate were evaluated.
Results:
In total, 202 patients were enrolled in the final analysis. The mean follow-up period was 12.5 months. The percentage of patients with cPPV was 39.2%. The mean operation time was 26 minutes for unilateral hernias and 34 minutes for bilateral hernias. One patient had a mild hematoma in the inguinal area in the immediate postoperative period, but it resolved spontaneously within 7 days. Recurrence and metachronous hernias have not been observed thus far.
Conclusions:
Laparoscopic hernia sac transection and intracorporeal ligation can be a safe and effective alternative for conventional herniotomy.
Introduction
Recently, Becmeur et al. 7 reported a novel laparoscopic method for pediatric hernia repair, which is basically identical to conventional hernia repair. They performed complete dissection, division, and closure of the processus vaginalis at the internal ring. Long-term follow-up results showed that the recurrence rate was 1%, which was comparable to open methods. 8 We strongly agree with the hypothesis that this laparoscopic method could provide a similar result if it is performed identical to classic herniotomy. Therefore, we adopted this method of laparoscopic herniotomy for pediatric inguinal hernia and prospectively evaluated the results.
Subjects and Methods
Institutional review board approval for this study was received. Between November 2008 and August 2011, 207 pediatric patients with inguinal hernia were included in this study under informed consent. The choice of laparoscopic surgery was made according to the wish of the child and/or parent after the operative risks and advantages had been well described. All of the patients underwent the laparoscopic technique of sac transection and intracorporeal ligation. The asymptomatic contralateral patent processus vaginalis (cPPV) was repaired using the same method. Patients were prospectively followed for 2 years. Perioperative complications and recurrence rates were evaluated during this time.
The surgical technical details are as follows. The procedure was performed with the patient under general anesthesia in the supine with frog-leg position. Through a transumbilical incision, a 3-mm or 5-mm optical port was inserted using an open technique. For visualization, a 30° 3-mm camera was used for infants, and a 30° 5-mm camera was used for children. Pneumoperitonuem was achieved by maintaining the abdominal pressure up to 8–12 mm Hg. The other two 3-mm operative trocars were placed along the lateral border of the rectus muscles. The processus vaginalis was completely divided at the internal ring level and ligated with 3/0 Vicryl® (Ethicon). All these procedures were performed by one experienced pediatric surgeon. Most patients over 50 gestational weeks of age were operated on in the day-surgery center and were discharged 4–6 hours after surgery, unless the parent wanted to stay longer for personal reasons. Patients under 50 gestational weeks of age were observed for 24 hours after surgery. Follow-up evaluations were performed in the outpatient clinic on postoperative Day 7, at 1 month, and every 6 months for 2 years by independent surgeons. When the clinic visit was not possible, a telephone interview was performed by a trained clinical nurse. All data were collected prospectively.
Statistical analysis
Continuous variables were compared using an independent sample, two-tailed Student's t test. Discrete variables were analyzed with the chi-squared test, and significance was defined as a P value of<.05. Descriptive statistics are expressed as mean±standard deviation values.
The learning rate is defined as the percentage decrease in operative time per doubling of cumulative procedure number. 9
Results
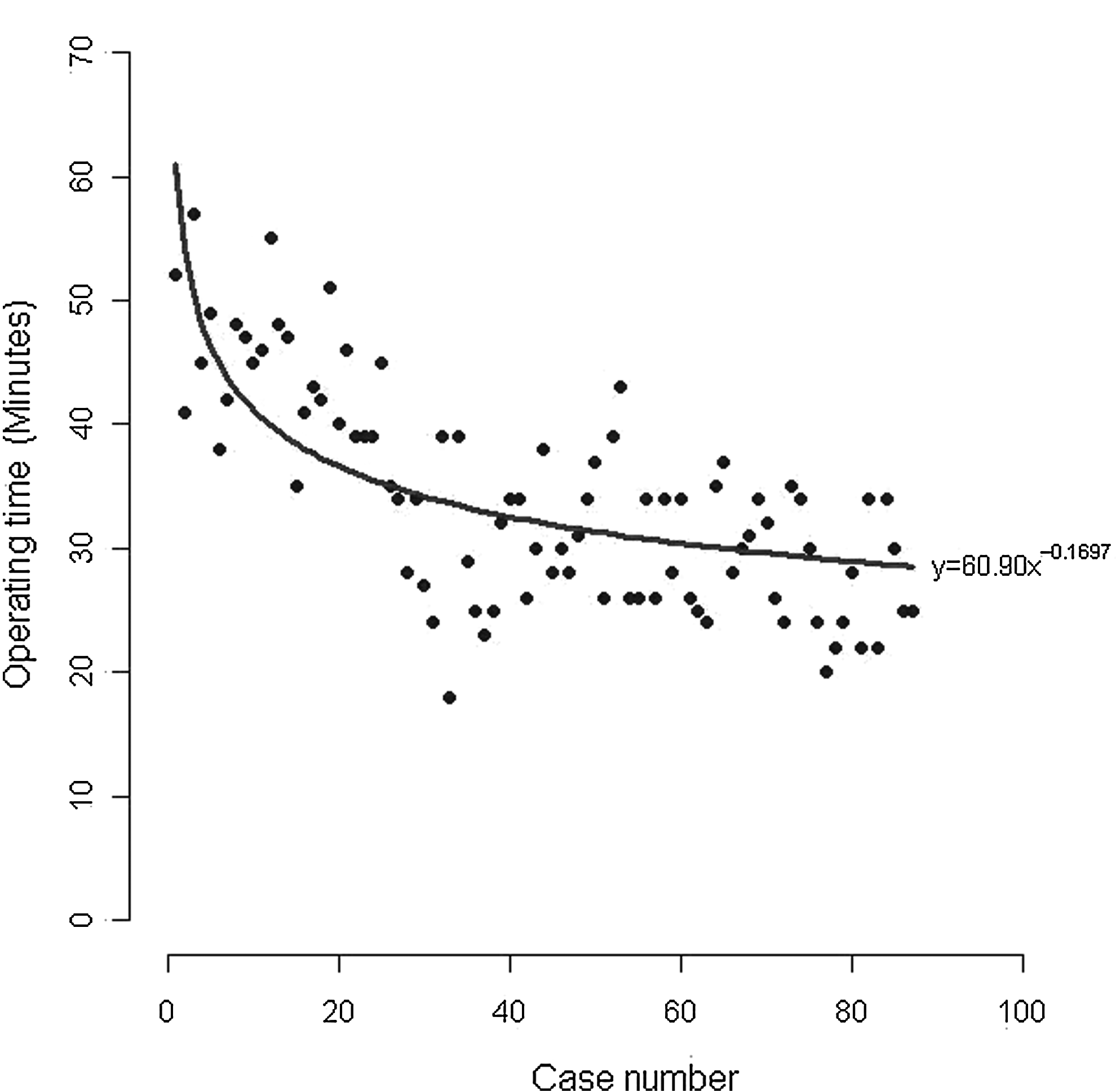
Out of 207 eligible patients, we obtained complete follow-up information from 202 patients. Therefore, 202 patients were enrolled in the final analysis. The mean follow-up period was 12.5 months (range, 4–34 months). The male to female ratio was 1.7:1 (Table 1). Bilateral hernias at the time of diagnosis occurred in 13 cases. Among the 189 unilateral hernias at presentation, the overall percentage of patients with cPPV was 39.2%. There was no significant correlation between age and detected rate of cPPV (Table 2). One patient had a mild hematoma in the inguinal area in the immediate postoperative period, but it resolved spontaneously within 7 days. Recurrence and metachronous hernia were not observed during the follow-up period. Operation time was 26.0±10.2 minutes for unilateral hernia repair and 34.01±8.7 minutes for bilateral hernia repair. Figures 1 and 2 show the learning curves of this technique with scatter plot diagrams. The learning rate of laparoscopic herniotomy was 14.62% for unilateral hernia repair and 11.10% for bilateral repair.

A scattergram of the operating time for unilateral hernia. The learning rate equation used was:
A scattergram of the operating time for bilateral hernia. The learning rate equation used was:
cPPV, contralateral patent processus vaginalis.
Discussion
Laparoscopic techniques for pediatric inguinal hernia have been evolving over recent years. There are still debates regarding the use of laparoscopy for pediatric inguinal hernia, but laparoscopic techniques seem to have several indisputable advantages. First, the magnified view of the internal ring gives surgeons an accurate diagnosis of inguinal hernia, including contralateral pathology, as well as easy identification of the cord or spermatic vessels, which is a technical challenge in performing conventional hernia repair on small babies. Other advantages are accurate diagnosis of contralateral pathology and prevention of metachronous hernia. 10 However, in some series, there has been a greater incidence of hernia recurrence compared with conventional open repair4,11 as well as complications related to the techniques, especially postoperative hydrocele. 12 These are major obstacles to adopting laparoscopy for pediatric inguinal hernia. A variety of laparoscopic techniques have been introduced in the past two decades such as the Z-type suture, 13 W-type suture, 14 flip-flap techniques, 11 subcutaneous endoscopically assisted ligation, 12 etc. However, these methods are technically similar in that herniotomy, which is a vital step of conventional herniorraphy, is not performed. Most previous laparoscopic techniques focused on the ligation of the internal ring without herniotomy; some of them focused on the ideal method of complete ligation of the internal ring.15,16 We believe that the high recurrence rate and postoperative hydrocele of these laparoscopic techniques are mostly due to not performing herniotomy.
Becmeur et al. 7 and Tsai et al. 10 introduced laparoscopic hernia sac transection (herniotomy) and intracorporeal ligation for pediatric inguinal hernia repair. Those techniques have almost identical surgical principles to those of conventional repair. We adopted this technique for pediatric hernia and performed prospective follow-up of the results. In this series of 202 patients and 317 hernia repairs, no recurrence was found during the mean follow-up of 12.5 months. Our results were comparable to those of conventional open repair in terms of the low recurrence rate and very low complication rate. In addition, we experienced no complications specific for laparoscopic hernia repair, such as postoperative hydrocele. However, 1-year follow-up is a relatively short interval to rule out future recurrence; therefore long-term follow-up should be performed to clarify these results.
The operative technique is very easy for the laparoscopic surgeon to learn. Therefore, qualified laparoscopic pediatric surgeons could adopt this technique with a short learning curve. The mean operation time of our study was 26 minutes for unilateral hernia repair and 34 minutes for bilateral hernia repair.
We applied the learning rate for objective analysis of learning curves for this procedure. 9 The learning rate was first described in energy-industry reports as the percentage at which the unit cost decrease with every doubling of cumulative production. 17 In our study, we defined the learning rate as the percentage decrease in the operation time per doubling of cumulative procedure number. The learning rate of laparoscopic herniotomy was 14.62% for unilateral hernia repair and 11.10% for bilateral repair (Figs. 1 and 2). The plateau of the learning curve was between 10 and 20 procedures.
This is the first report to show the learning curves of pediatric laparoscopic hernia repair, although it has a limitation in that it is a single surgeon's experience. The operation time is comparable to that of conventional repair, and the learning curve is short. These results could refute the prejudice that laparoscopic handling of the internal ring and intracorporeal suture ligation are difficult and troublesome.
Another important merit of this laparoscopic technique is that the operation could be performed with minimal to no handling of the cord structure when the surgeon ligates the internal ring. By lifting the peritoneum using the dissecting forcep, the peritoneum is easily detached and dissected from the surrounding structures at the internal ring level. The previously reported laparoscopic hernia repairs that ligate the internal ring without sac dissection and transection carry the risk of inadvertent entrapment of the vas and cord structure, especially if there is peritoneal thickening due to chronic irritation and incarceration in the internal ring. 10 In addition, not performing herniotomy leads to a postoperative scrotal hydrocele. Moreover, blunt dissection of the cord structure during conventional hernia repair has been considered the main reason for testicular atrophy and cord injury. This more delicate handling technique of the hernia sac can theoretically bring a better result for inguinal hernia repair, but long-term follow-up study to investigate testicular atrophy as well as testicular function should be performed for verification.
The intriguing finding for cPPV is that there is no correlation between age and cPPV. According to previous reports, a younger age group had a higher proportion of cPPV, 18 but our results showed no significant relationship between age and cPPV, even though we analyzed the results after stratification by short age intervals. How to treat cPPV is an unresolved issue for pediatric inguinal hernia. There is lack of evidence on whether laparoscopic treatment of cPPV brings additive complications. 3 If we use this laparoscopic technique that involves minimal touching of the cord structures, it may produce no additive complications as well as prevent contralateral metachronous hernia. However, the detected rate of cPPV is much higher than the actual incidence of contralateral metachronous hernia. 19 Therefore, we should take caution in treating cPPV and performing surgery in selected cases because the benefit of cPPV ligation is unclear in the absence of robust knowledge about the natural course of cPPV.
Conclusions
Laparoscopic hernia sac transection and intracorporeal ligation can be a safe and effective alternative for conventional herniotomy. To evaluate the most adequate standard technique for laparoscopic pediatric inguinal herniorraphy, a prospective clinical trial should be performed.
Footnotes
Acknowledgments
The research was supported by a grant from Korea University.
Disclosure Statement
No competing financial interests exist.