
Abstract
Abstract
Introduction:
Current surgical techniques for gastroesophageal reflux in infants involve gastric fundoplication and crural repair. These operations are complicated by a high recurrence rate in the infant population. The primary cause of failure is generally related to recurrent hiatal hernia. Minimal dissection of the gastroesophageal junction has been linked to reduced hiatal hernia formation. We propose an alternative plication technique for modifying the gastroesophageal junction called cardiaplication. In an effort to evaluate the effectiveness of this alternative plication technique, an animal model was developed.
Materials and Methods:
After Institutional Animal Care and Use Committee approval, 12 Yucatan piglets, weighing 10–12 kg, underwent laparotomy and cardiaplication. Plication was performed by embrocating the cardia of the stomach and secured with two or three interrupted sutures over a 1-cm length. The technique was then evaluated by comparing cardia yield pressures (CYPs). Pre- and postoperative CYPs were determined by filling the stomach with water until the cardia became incompetent. These values were compared using Student's t test for paired samples.
Results:
Cardiaplication was successfully completed in all pigs. CYP increased in all animals after cardiaplication from a mean of 12.5±9.6 to a mean of 76±25 cm of H2O (P<.001).
Discussion:
Cardiaplication results in an increase in CYP in young pigs. This procedure may be an alternative antireflux operation for infants. With cardiaplication there is the potential benefit of not needing to modify the crura or the gastroesophageal junction. This may translate into fewer postoperative complications and less need for reoperations due to recurrent hiatal hernia.
Introduction
St Peter et al. 10 have shown in a randomized clinical trial that minimizing the hiatal dissection can lead to less wrap failure due to herniation through the esophageal hiatus. Other risk factors for recurrent postoperative GERD are patients less than 1 year of age and patients with neurologic impairment.11–15 Others have speculated that risk of recurrence is more often related to preoperative presence of a hiatal hernia, postoperative retching, and postoperative esophageal dilation. 16
Seemingly, where a minimal dissection operation reduced GERD recurrence (as measured by need for repeat operation), an operation that necessitates no dissection of the hiatus may have even lower incidence of postoperative recurrence. We have developed a novel surgical approach for refractory GERD called cardiaplication that aims to lengthen the intra-abdominal esophagus without performing any dissection of the hiatus (Fig. 1). In this article we describe the technique as a proof of concept in a porcine animal model.
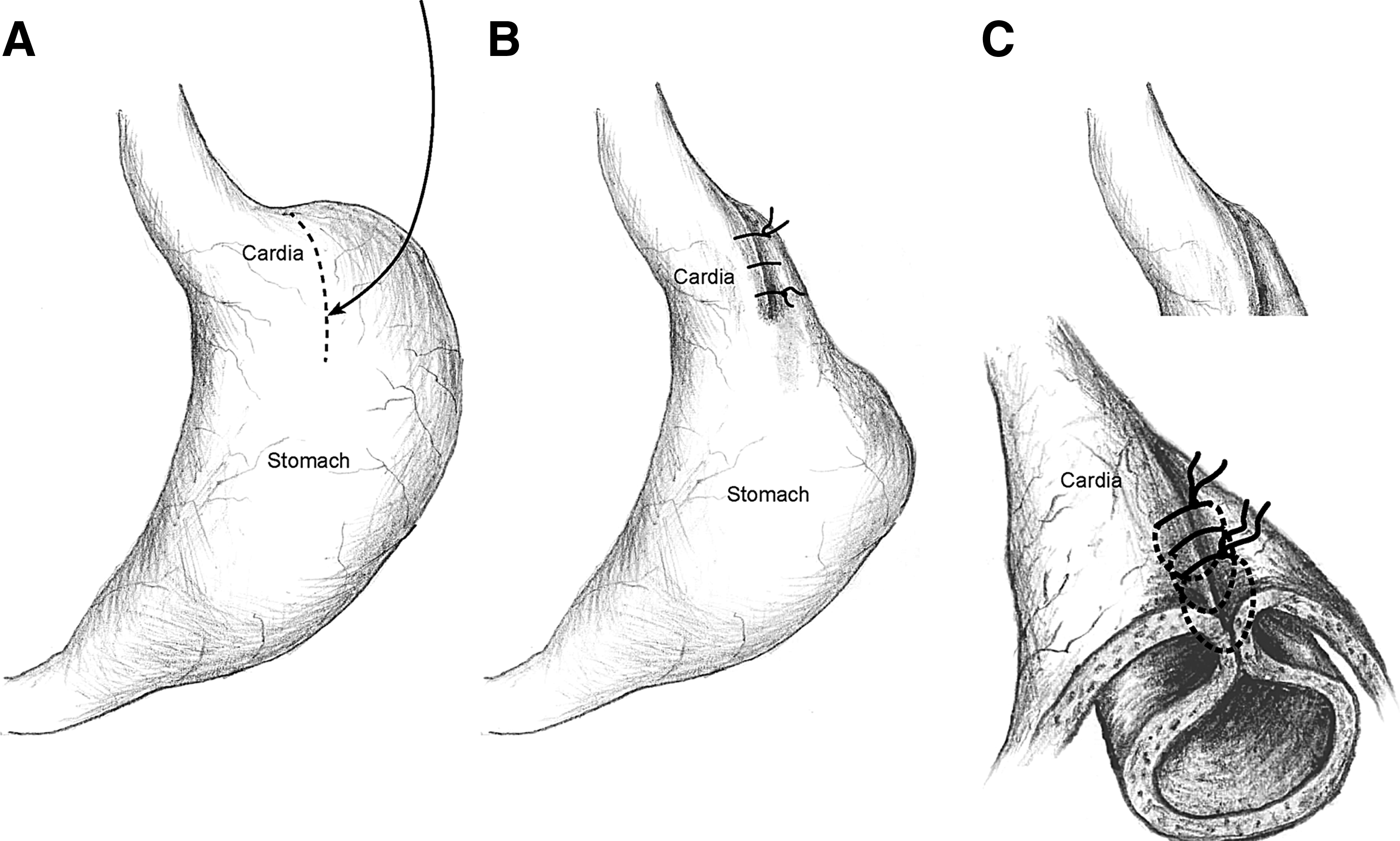
Illustration of cardiaplication showing
Materials and Methods
Animals and anesthesia
After approval by the Emory University Institutional Animal Care and Use Committee, 12 8-week-old Yucatan piglets with a mean weight of 10.7±0.8 kg were obtained and underwent open laparotomy, gastrotomy, and cardiaplication. The animals were sedated with intramuscular ketamine (10 mg/kg) and azaperone (15 mg/kg). After an intravenous application of ketamine (10 mg/kg) and propofol (1 mg/kg), the animals were endotracheally intubated, and anesthesia was maintained by 2%–3% isoflurane inhalation. Each pig was positioned in a supine position to facilitate exposure to the stomach. After intubation, an 8-mm red rubber catheter was placed as an orogastric tube and placed on low continuous suction to evacuate gastric contents.
Gastrostomy
A midline laparotomy incision was made followed by dissection to expose the stomach. A purse-string suture approximately 1–2 cm in diameter using 3-0 suture was made on the anterior gastric wall. In the center of the purse string, a perforation was created using electrocautery, and a 16-French feeding tube was inserted into the stomach. The purse-string was then tightened to secure the tube in place. The feeding tube was then connected to intravenous tubing to allow the introduction of normal saline into the stomach. An intravenous line was placed in the stomach and secured in a similar fashion. This intravenous line was connected to a pressure transducer and monitor. Next the duodenum was exposed and clamped to prevent distal transit of gastric contents. Intragastric pressures were recorded as baseline cardia pressure, prior to the instillation of intragastric fluid.
Saline was then infused into the stomach, and gastric pressures were recorded. Fluid was infused until reflux was observed into the esophagus or a decrease in intragastric pressure was noted. Intragastric pressures were recorded as the pressure necessary to produce reflux in the normal, in vivo porcine LES. This was recorded as the preoperative cardia yield pressure (CYP). After completion of the measurement, the stomach was emptied by placing the 16-French feeding tube on gentle suction.
Cardiaplication
A 1–2-cm plication of the cardia of the stomach was then performed over a bougie. Plication was performed by manually invaginating the cardia of the stomach into the stomach lumen. It was secured in place using 3-0 silk sutures in an interrupted fashion (Fig. 2). The intragastric pressure necessary to produce reflux or disrupt the plication was then measured and recorded as described above. This was recorded as the postoperative gastric yield pressure.

Cardiaplication performed with interrupted sutures on the cardia of the stomach.
Statistical analysis
Mean±standard deviation (SD) values were calculated for all measurements. Pre- and postoperative CYPs were compared using a Student's t test for matched, paired samples. A value of P<.05 was considered statistically significant.
Results
Cardiaplication was successfully performed in 12 Yucatan piglets. No complications were encountered during the laparotomy/gastrotomy/cardiaplication procedure or during the measurement of the CYP. Average operative time was 56 minutes (range, 34–75 minutes), and estimated blood loss was minimal.
Average preoperative CYP was 12.5 (SD±9.7) cm of H2O compared with postoperative CYP of 75.9 (SD±25.3) cm of H2O with a mean increase of 63.4 (SD±25.8) cm of H2O. Based on a paired t test, this was a statistically significant increase in yield pressure (P=.0001). The results for the individual piglets are shown in Table 1.
Pressure data are in cm of H2O.
Discussion
As a proof of concept, cardiaplication was performed and tested in an animal model. These preliminary data confirm that by reinforcing the LES and tubularizing the stomach, plication of the gastric cardia significantly increases the resistance at the gastroesophageal junction as determined by a significant increase in the CYP. The concept of CYP as a means of testing the effectiveness of an antireflux procedure is not new. This technique has been well described for evaluating fundoplications and as a measure for LES incompetence in pig models.17–19
Cardiaplication is a novel and innovated surgical technique aimed at addressing medically refractory GERD in children. The technique is performed solely on the left side of the stomach. The operation requires minimal dissection of the gastrosplenic ligaments only. After mobilization, the cardia of the stomach is invaginated in to the stomach, tubularizing this portion of the stomach. The tissue is then secured using two or three interrupted sutures. This imbricated tissue creates an internal flapper valve at the level of the LES. By focusing solely on the left side of the stomach for the operation, the hiatus is left untouched. This eliminates any potential disruption or scaring that would alter natural growth. By invaginating the cardia of the stomach, the remaining stomach is tubularized. The impact of this is that the intra-abdominal portion of the esophagus is effectively lengthened. Additionally, the imbricated tissue creates an intralumenal flapper valve below the level of the LES. This flapper valve reinforces the sphincter, allowing for food to travel from the esophagus into the stomach but limiting the ability of acid to reflux back up into the esophagus.
In addition to this animal model, cardiaplication has also been conducted with favorable results in a small, select patient population. 20 Ongoing clinical trials are now underway to further evaluate this surgical model in infants.
Footnotes
Disclosure Statement
No competing financial interests exist.