
Abstract
Abstract
Purpose:
During thoracoscopic pulmonary lobectomy (TPL) in larger children (>15 kg), an endoscopic stapler (ES) and endoscopic clipper (EC) are used during dissection and division of the pulmonary vessels (PVs) and bronchus. However, in smaller children (<15 kg), ES/EC cannot be used because of limited space. We report our technique for thoracoscopic dissection and division of the PVs and bronchus in smaller children.
Subjects and Methods:
Fifteen cases of sequestration/congenital cystic adenomatoid malformation weighing less than 15 kg (range, 8–15 kg; mean, 11 kg) were the subjects for this review. With the patient under single-lung ventilation in the lateral decubitus position, four ports ranging from 5 to 12 mm were placed. After the PVs and bronchus were exposed, thick silk was used to encircle them as a traction suture. By applying traction, the PVs and bronchus could be exposed, and ES/EC were used safely by applying countertraction.
Results:
All cases had uneventful TPL (upper in 3 patients, middle in 3 patients, and lower in 9 patients). ES/EC were easy to use. Mean operative time was 220 minutes.
Conclusions:
Our technique allows the PVs and bronchus in children weighing less than 15 kg to be divided safely using ES/EC. We strongly recommend our technique, although simple, be used during TPL in smaller children.
Introduction
There are several issues to consider with regard to thoracoscopic pulmonary lobectomy (TPL). Most underlying conditions are complex, dissection can be tedious, there is a risk for bleeding, and anesthesia can be complicated. Actually, with improvements in endoscopic devices such as the endoscopic stapler (ES) and endoscopic clipper (EC) and ongoing exposure to endoscopic surgery, TPL has become safer and more effective, as the need to suture ligate the pulmonary vessels (PVs) and bronchus during TPL has been virtually eliminated. Reported operative complications of TPL include air leakage and injury to the bronchus requiring conversion to open or mini-thoracotomy.3,4 Thus, TPL is particularly challenging when the patient is small (<15 kg) because the thoracic cavity is too small to use ES/EC. 4 We report a simple technique we devised to perform TPL in children weighing less than 15 kg.
Subjects and Methods
Records of 15 patients with sequestration/congenital cystic adenomatoid malformation (CAM) weighing less than 15 kg treated by TPL were reviewed. Preoperatively, all had infective conditions of the affected lobe with respiratory symptoms and signs.
Surgical technique
The patient is positioned in the lateral decubitus position with single-lung ventilation. The lateral decubitus position allows access to the hilum both anteriorly and posteriorly. The surgeon and the assistant stand in front of the patient and view a monitor behind the patient. A 5-mm trocar is inserted in the fifth intercostal space at the mid- to anterior axillary line using the open Hasson's technique. The chest is insufflated initially using low flow pressure carbon dioxide to help collapse the lung completely. Flow of 1 L/minute at a pressure of 4–6 mm Hg is then maintained throughout the operation. A standard four-trocar technique is used. A 5-mm scope (less than 30°) is used to determine the position of the major fissure and lung parenchyma, and the other working ports are placed to give best access to structures in the fissure as this is where the most complicated dissection will be performed. In general, TPL involves the same principles as open lobectomy, namely, isolation and division of the pulmonary vein, artery, and bronchus and separation of lung parenchyma using a combination of sharp and blunt dissection and electrocautery to define and isolate the pathologic lesion. After the PVs and bronchus are exposed, a thick silk tie is used to encircle the vessels, and another is used to encircle the bronchus as traction sutures. By applying traction and countertraction, the PVs and bronchus can be exposed completely (Fig. 1). The pulmonary vessels can be ligated after being stretched slightly using EC devices such as ENDO CLIP™ (Tyco Healthcare, Norwalk, CT) or the Hem-o-lok® polymer clip (Teleflex Medical, Research Triangle Park, NC) and then divided with a LigaSure™ coagulation system (Valley Lab, Boulder, CO) or ligated directly. Pulmonary vein ligation before division of the pulmonary artery can lead to congestion in the lobe, which decreases available space in the thoracic cavity. The bronchus can be divided using an ES device such as Endo-GIA™ (Tyco Healthcare). If the exposed length of bronchus is insufficient for division with ES, the bronchus may be grasped with atraumatic forceps and ligated directly using an Endoloop® ligature (Tyco Healthcare). At this time, it is important for the bronchus to be grasped with the forceps through the loop of the Endoloop device rather than dividing it directly to keep the lung collapsed and prevent any discharges from the bronchus (Fig. 2). The endotracheal tube is ventilated to ensure that the remaining lung inflates appropriately before the procedure is completed using ES.

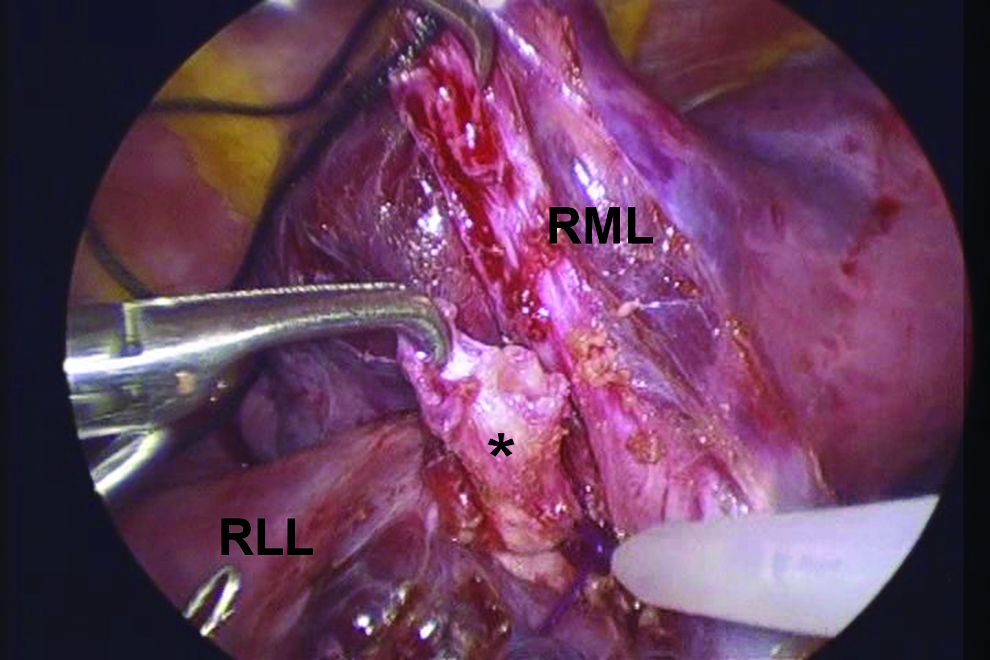
During right middle lobectomy, a thick silk tie has been placed around the bronchus as a traction suture. Then, the bronchus (asterisk) may be grasped with forceps and ligated directly using Endoloop. RLL, right lower lobe; RML, right middle lobe.
Once the lobe is separated from the rest of the lung, it is placed in a specimen bag, such as an Endo Catch™ bag (Tyco Healthcare), and then removed in pieces through a slightly enlarged port site. A chest tube is placed under direct vision in all cases.
Results
Histopathologic indications for TPL were CAM (right upper lobe, n=1; left upper lobe, n=2; right middle lobe, n=3; right lower lobe, n=4; and left lower lobe, n=1) and sequestration in the left lower lobe (n=4). Mean age at surgery was 2.0 years (range, 6 months–3 years), and mean body weight was 11 kg (range, 8–15 kg). TPL was successful in all cases, without intraoperative complications, and there was no requirement for conversion to open/mini-thoracotomy. Chest tubes were removed in all cases by the second postoperative day.
Discussion
Thoracoscopy has advanced significantly since the 1970s when Rodgers et al. 5 introduced the technique to pediatric surgery, and its safety and efficacy in children have been clearly demonstrated.4,6,7 Although the operating time is longer for thoracoscopy compared with conventional thoracotomy, some studies7–9 have shown that TPL has better clinical outcome than conventional open lobectomy because there is less postoperative pain, shorter hospitalization, and better wound cosmesis not likely to be associated with scoliosis or chest wall deformity. However, safe control of major vessels and the bronchus can be complicated. Initially, this was achieved through a mini-thoracotomy using a combination of suture ligatures and a standard surgical stapler, but over time, with technical improvement, PVs and the bronchus have come to be managed completely through endoscopic ports, eliminating the need for thoracotomy.4,6,10
Rothenberg 4 reported using ES for the main pulmonary vessels and bronchus in larger children (>15 kg), but in smaller children (<15 kg) LigaSure was used instead because most ES devices require a 12-mm port for access and at least 4 cm of intrathoracic space to open the device and are too big to fit in the thoracic cavity of a child less than 15 kg. Recently, Rothenberg et al. 11 described their experience with infants weighing less than 10 kg: the major vessels in smaller children can be divided using LigaSure, and the bronchus requires division and closure with 3-0 monofilament absorbable suture material in smaller children. Although these investigators reported no cases of stump leakage or bronchopleural fistula, the authors feel that there are technical difficulties related to suturing in such small thoracic cavities, and thus risks for leakage and injury to surrounding tissues. Indeed, Rothenberg4,10 did experience a complication during TPL when ES was used to divide the left lower lobe bronchus and the left upper lobe bronchus was injured, requiring bronchoplasty of the upper lobe bronchus as an open procedure. Our technique prevents such complications because the traction sutures greatly improve exposure. Indeed, in our patient weighing 8 kg, this technique allowed great exposure to divide safely the PVs and bronchus.
Bignon et al. 12 described that LigaSure's reliability depends on vascular diameter and on patient age. In their series, dehiscence occurred more often when vessels had diameters larger than 7 mm. Vascular accidents can be prevented by using a sealing device, such as proximal EC, during ligation of PVs in TPL. The authors also divided PVs with a ligature after ligation using EC when vessels had diameters larger than 7 mm. Then it is necessary to leave enough PV pedicle to allow easy ligation using both EC and ligature because ligature has the risk of disrupting EC. If there is not enough PV pedicle to allow ligation using both EC and ligature, PVs are sharply cut after ligation using EC. In the case of thin and fragile PVs, care is taken that EC may cause bleeding due to its slip and twist; therefore LigaSure is recommend to seal and divide it in such cases.
Although the number of cases and follow-up are limited, our technique allows the PVs and bronchus to be divided safely using ES/EC in children weighing less than 15 kg. Exposure is greatly improved, and surrounding structures can be checked adequately before devices are fired to prevent injury. We strongly recommend our technique, although simple, be used routinely during TPL in smaller children.
Footnotes
Acknowledgments
This study was supported in part by a Grant-in-Aid (S0991013) from the Ministry of Education, Culture, Sport, Science, and Technology, Japan through the Foundation for Strategic Research Projects in Private Universities.
Disclosure Statement
No competing financial interests exist.