
Abstract
Abstract
Background:
LigaSure™ (Covidien, Mansfield, MA) has been used in cases undergoing laparoscopic colon and rectal resections. This study aims to analyze the efficacy and safety of the 5-mm and 10-mm devices.
Subjects and Methods:
Patients who received a laparoscopic or hand-assisted laparoscopic operation for a tumor located in the sigmoid colon or rectum since 2006 were abstracted from a prospectively designed database, and findings were analyzed in two groups based on size of the device used during the procedure. The videotapes of the procedures were watched, and operation reports were read to obtain further information on specific intra- and postoperative complications. Demographics, tumor and operation-related information, and postoperative data were compared.
Results:
Among 215 (128 [59.5%] males; median age, 59.5±13.8 years) patients, data obtained from the 5-mm (n=32) and 10-mm (n=183) groups were identical regarding demographics and data related to tumor (localization and stage) and operation (number of harvested lymph nodes, conversion rates, operation time, intraoperative bleeding, transfusion requirement, reoperation rates, complications, 30-day mortality, and length of hospital stay). However, more patients underwent an anterior resection in the 10-mm group than in the 5-mm group (31.7% versus 15.6%, P<.05). Further analyses found device-related bleeding in 8 (3.7%) cases (2 [6.3%] versus 6 [3.3%] in the 5-mm versus 10-mm group, respectively, P>.05), requiring further attempts for hemorrhage control (n=6), conversion to open surgery (n=1), or relaparotomy (n=1).
Conclusions:
The 5-mm and 10-mm LigaSure devices are similarly effective and safe during laparoscopic sigmoid colon and rectal resections. Severe bleeding from larger vessels may be observed, requiring conversion to open surgery or relaparotomy.
Introduction
An electrothermal bipolar vessel sealer instrument, LigaSure™ (Covidien, Mansfield, MA), has been introduced as an alternative to other devices or techniques for hemostasis. 5 This instrument has been shown to be effective and safe in abdominal surgery.5–8 The device is designed for laparoscopy in two sizes of functioning heads, either 5 mm or 10 mm in diameter. The 5-mm LigaSure has a smaller electrode (18 versus 22 mm) and a shorter seal width (2–4 versus 6 mm) than the 10-mm tool. According to the manufacturer, a secure seal of tissue bundles and vessels up to 7 mm with a collateral damage of 2 mm is equally warranted for both instruments. Although both devices have been used for laparoscopic left colon, sigmoid, and rectal resections, there have been limited data comparing clinical outcomes. 9 The single study included only 30 cases and revealed similar results, but as the authors mentioned, it may be biased because of the small number of patients and lack of a power analysis. 9 This is particularly true for the evaluation of complications including bleeding from the inferior mesenteric artery or thermal injuries, which are thought to be relatively rare. Thus, this study aims to analyze the effectiveness and safety of the 5-mm and 10-mm products in laparoscopic sigmoid colon and rectal tumor operations.
Subjects and Methods
The Kartal Education and Research Hospital Ethics Board approved the design and content of the study prior to data abstraction (reference number B104ISM4340029/1009/56). Data for patients who underwent a laparoscopic or hand-assisted laparoscopic colon and/or rectal resection for premalignant and malignant lesions located in the sigmoid colon or rectum between January 2006 and June 2011 were retrospectively abstracted. Those who underwent surgery for a recurrent cancer or other tumors rather than adenocarcinomas or dysplastic polyps were excluded in order to homogenize the information. Similarly, cases were also excluded if other devices or techniques were preferred for vascular ligation instead of the products studied during the procedures.
The patients were assigned into two groups according to the preferred size of the device. The primary surgeon decided the size of the instrument because there were no precise criteria for instrument preference; however, the 5-mm device was not available until May 2010 in our institution because of logistic reasons. All procedures were performed or supervised by a single surgeon (M.O.). Laparoscopic anterior resections via four or five trocars were carried out for sigmoid colon lesions. During these procedures a medial-to-lateral approach was followed, and the LigaSure device was used both as a sealing device for large vessels, including the inferior mesenteric artery and vein, and as an ordinary laparoscopic instrument for blunt or sharp dissection. The devices were used in the same consistent manner in all procedures by all surgeons. In case of a rectal tumor, hand-assisted laparoscopic low anterior resections were preferred as described in a previous study from our institution. 3
These aspects were abstracted and compared between the groups: demographics, tumor localization, presence of neoadjuvant radiation therapy, intraoperative information (type of resection, synchronous hepatic metastasectomy, operation time, quantity of bleeding, and conversion rates), postoperative data (length of hospital stay, complications, rate and cause of reoperation, and 30-day mortality), the requirement and amount of transfusions, and pathological characteristics (stage and number of harvested lymph nodes).
Finally, device-related complications were searched with two techniques. First, operation reports were reviewed for possible intraoperative complications including device-related bowel injury or vessel bleeding, and second, videotapes of the procedures were watched by an investigator (C.G.) for patients who had been reported to have an intraoperative complication or a postoperative problem including prolonged hemorrhagic drainage or a reoperation due to missed bowel injury or intraabdominal hemorrhage. At the end of the analyses, the link between the use of the device and the problem was defined as “likely,” “possibly, or “not related.” Complications related to the LigaSure use were separately analyzed in terms of treatment and outcome, and the risk factors were evaluated for the prediction of device-related complications.
Statistical analysis
Data were analyzed by using SPSS version 15.0 for Windows. Results were given as percentages, mean and standard deviations, or median and ranges. Quantitative and qualitative variables were compared with Student's t test and chi-squared (Pearson's or Fisher's Exact) test, respectively.
Results
In total, 215 (128 [59.5%] males; median age, 59.5±13.8 years) patients have undergone a laparoscopic or hand-assisted laparoscopic resection of the sigmoid colon or rectal adenocarcinomas or dysplastic polyps using either a 5-mm (n=32; 14.9%) or 10-mm (n=183; 85.1%) LigaSure during the study period at our institution. Most of the tumors were located in the rectum (n=152; 70.7%). Demographics, localizations, and pathological stages of the tumor and number of patients requiring neoadjuvant chemoradiation therapy were similar in the two groups (P>.05 for all) (Table 1). However, resection types were statistically different within the groups because there were more patients undergoing an anterior resection in the 10-mm group than the 5-mm group (31.7% versus 15.6%, P=.022) (Table 1). Other intra- and postoperative parameters were comparable between the groups, including operation time, intraoperative bleeding, transfusion requirement, number of harvested lymph nodes, conversion rate, length of stay, complications, reoperations, and 30-day mortality (Table 2).
Pairwise comparisons revealed P values as follows: P=.025 for anterior versus low anterior, P=.999 for anterior versus abdominoperineal, and P=.055 for low anterior versus abdominoperineal resections.
Operation reports and videotapes were evaluated for inspecting device-related complications. Operation reports reported bleeding from the inferior mesenteric artery in 7 cases, 2 (6.3%) in the 5-mm and 5 (2.7%) in the 10-mm group (P=.279); all were decided to be highly likely related to the instrument use according to operation movies of the procedures, and among those, conversion to open surgery was required in a single patient (Table 3 and Fig. 1). No device-related problem was observed in operation movies of patients whose postoperative period was complicated with prolonged hemorrhagic drainage (n=7), relaparotomy (n=2), or both (n=1). Reoperation notes were evaluated for 3 patients who had a second laparotomy due to intraabdominal sepsis secondary to missed bowel injury (n=2) or prolonged hemorrhagic drainage complicated with hemodynamic instability (n=1). The reports revealed injuries in the 2 cm of tissue proximal to the anastomosis and on the ileum, which were expected to be related to the stapler application and insertion of the trocar and which were not likely to be caused by thermal injuries secondary to use of the LigaSure. However, reoperation notes indicated bleeding from the middle colic artery in a patient who underwent a subtotal colectomy with anterior resection, and that was decided to be possibly related to LigaSure use (Table 3). Thus, there were 8 patients (3.7%) who had LigaSure-related problems, and possible predictive factors for complications linked to the device were questioned. The ages were similar in those who had complications (59.3±13.5 years) and those who did not (63.7±20.2 years) (P=.345). Other aspects were also identical for the device-related complications, including gender (6 [4.7%] in males versus 3 [3.4%] in females, P=.742), localization of the tumor (3 [4.8%] for sigmoid colon versus 6 [3.9%] for rectum), neoadjuvant chemoradiation therapy (4 [3.6%] among receivers versus 5 [4.8%] among non-receivers), and resection type (2 [3.2%] for anterior, 5 [4.2%] for low anterior, and 2 [6.3%] for abdominoperineal, P=.794).
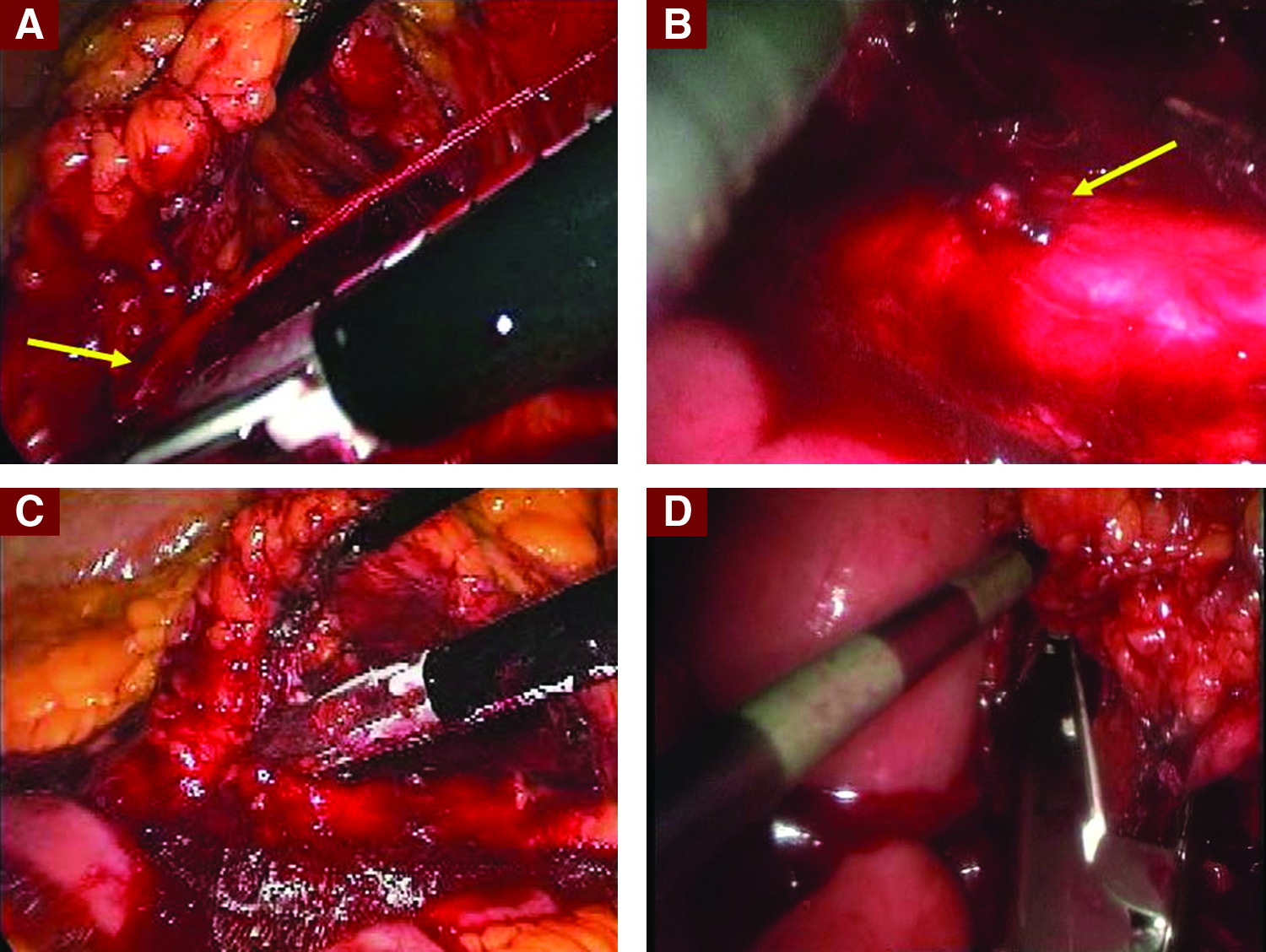
Bleeding from
IMA, inferior mesenteric artery; MCA, middle colic artery.
Discussion
Laparoscopic colorectal surgery has been shown to be safe; however, it necessitates special equipments for dissection, coagulation, or vascular fixation. LigaSure is a multifunctional instrument maintaining dissection, grasping, sealing, and dividing minor vessels. 10 LigaSure can be used as a coagulator, dissector, and grasper and thus may also reduce instrument traffic in laparoscopic surgery. 11 The device is particularly necessary for separating large vessels, and LigaSure is advocated to secure vessels up to 7 mm in diameter.5,12 Prospective single-armed or comparative studies have revealed that LigaSure use may be safe in colorectal surgery, and the results are comparable to those obtained after use of 5-mm ultrasonic shears (Harmonic® scalpel [Ethicon]) and conventional technique using electrocautery and clipping.13–15 A meta-analysis has shown that LigaSure may reduce the operation time, blood loss, complications, and postoperative pain. 16 Although the device is believed to be secure and effective for laparoscopic colorectal operations, there are limited data comparing the 5-mm and 10-mm sealers on a clinical basis on humans.8,9 The single comparative study included only 30 cases; thus, as the authors mentioned, it may be underpowered because of the small number of patients, especially in evaluating the risk of complications taht are relatively rare. 9 Thus, further information evaluating the safety and effectiveness of the LigaSure in colorectal surgery is extremely necessary.
The demographics and tumor-related aspects were identical within the two groups in the current study, showing that both groups were homogeneous; however, there were statistically more patients who underwent an anterior resection in the 10-mm LigaSure group. We do not know the reason of this finding, but we think that it may be incidental because in our practice there were no precise criteria for device preference according to type of resection. The intra- and postoperative parameters were similar between the groups regarding operation time, intraoperative bleeding, transfusion requirements, number of harvested lymph nodes, conversion rate, and length of stay. This is an important conclusion showing that the 5-mm device may be as effective and safe as the 10-mm device in patients undergoing sigmoid colon or rectal surgery. Furthermore, the current study also analyzed other rare measurements, including complications, reoperations, and mortality, and questioned device-related problems. The results revealed that these parameters were also identical between the groups; however, we do not know the power of this conclusion because these complications were rare among the patients studied. Some may believe that the length of stay and the rates of anastomotic leak and 30-day mortality are quite high in the current study. However, we believe that our data are comparable to those obtained from the recent prospective randomized trials on laparoscopic colorectal surgery,17–19 although the current information represents a long study period and also includes the results of our initial experience, when the learning curve was not completed.
Device-related complications were evaluated by an investigator who was not the primary or supervising surgeon. It was decided that in 8 (3.7%) cases, the complications might be highly likely (n=7) or possibly (n=1) secondary to the use of the LigaSure. In our opinion, the rate of device-related problems was tolerable (3.7%) from two perspectives. First, we believe that arterial bleeding is not an exceptional situation, and most surgeons have experienced it in laparoscopic and open surgery.20,21 Second, in our study, the intraoperative bleeding was controlled with further attempts and necessitated conversion to open surgery in only 1 case. We believe that when severe bleeding from the inferior mesenteric artery occurs during laparoscopic colorectal surgery, laparoscopic control of the hemorrhage may be generally achieved. In addition, delayed hemorrhage may also occur in cases operated on with LigaSure as was observed in a patient who underwent a subtotal colectomy. The current study did not determine predictive risk factors for device-related complications. Finally, we believe that device-related thermal injury is an extremely rare situation because we did not observe it in this large series of patients.
The present study has some restrictions. The lack of a power analysis due to the retrospective nature of the study may limit the reliability of our results. This is particularly true for complications that are rare, such as the incidence of bleeding from the inferior mesenteric artery. Thus, although no statistical difference was observed between the groups, it is possible that a significant difference in the risk of bleeding may be present if the sample size was larger. In addition, the numbers of patients in the groups were unbalanced because of the fact that the primary surgeons decided the device preference. Furthermore, the factors affecting the decision-making were not clear, and the 5-mm instrument was not available in a particular period of the study. However, because the groups were homogeneous regarding demographics and localization and stage of the tumors, we believe that the comparisons evaluating intra- and postoperative results were reliable. Another restriction was the heterogeneity in the procedures. Although the study may be criticized because it has included both anterior and low anterior resections in both groups, we believe, however, that the ligation of the inferior mesenteric artery that takes place in both procedures is of paramount importance in disclosing the performance of the devices. In addition, in our opinion, the current data contain valuable information because the study includes an adequate number of patients analyzed for intra- and postoperative features and focuses on device-related complications, and consequently reflects our 5-year experience on the safety and effectiveness of the instruments.
In conclusion, we believe that 5-mm and 10-mm LigaSure devices are similarly effective and safe during laparoscopic sigmoid colon and rectal resections. Although severe bleeding from larger vessels or the inferior mesenteric or middle colic artery may be observed during or after the use of LigaSure, the rate of this complication is tolerable. This complication is generally controlled laparoscopically and does not require conversion to open surgery. Delayed bleeding may also happen and may necessitate relaparotomy. We believe that device-related thermal injury is an extremely rare situation.
Footnotes
Disclosure Statement
No competing financial interests exist.