
Abstract
Abstract
The exponential increase in the rate of obesity and its associated co-morbidities has increased the demand for bariatric surgery. Over the past few decades, surgical weight reduction by gastric restriction, malabsorption, or a combination of both has been the preferred approach to achieve sustained weight loss in the morbidly obese. Although extremely effective, surgical procedures carry significant complications and risk with mortality rates of 1%. Because of the cost, surgical risk, and complications, there is a demand for less invasive procedures. Endoscopic approaches include placement of endoluminal space-occupying devices, stapling devices to reduce gastric volume, barrier devices to reduce small bowel absorptive area, and methods to regulate gastric emptying. Current and ongoing studies have delivered promising results across many aspects of endoscopic approaches. However, many technical obstacles still exist that have to be resolved with further research before endoscopic bariatrics can be widely deployed. At present the role of endoscopy is well established in preoperative evaluation as well as in recognition and management of many postoperative complications in bariatrics. In this article, we review the current and future endoscopic methods for weight reduction that are either in practice or in testing.
Introduction
The role of endoscopy in bariatric surgery is traditionally used in preoperative weight loss reduction to reduce surgical morbidity and for postoperative revision of leaks and strictures. 6 However, the role of endoscopy in bariatric surgery as a primary tool is less well established. The concept of endoscopy in bariatrics became popularized when endoluminal procedures were used in the treatment of gastroesophageal reflux disease (GERD). 2 With the success of endoscopic treatment of GERD came the concept of using endoscopy as a primary method for weight reduction. Minimally invasive procedures such as endoscopy sought to decrease complication rates, cost, and time and provide the potential avenue for bariatric surgery as an outpatient procedure. 2 Moreover, endoscopic techniques provide utility for patients who do not qualify for bariatric surgery who continue to pursue noninvasive weight reduction. 6 The intragastric balloons were the earliest devices and have been used to treat obesity for the last 20 years. The designs of space-occupying devices have improved since then. Furthermore, there have been significant additions to the armamentarium with intraluminal suturing devices, sleeves to eliminate absorptive area, and modulation of gastric emptying. In this review we have discussed various endoscopic devices and procedures that have been studied or are under investigation for application in bariatrics. The procedures and devices are classified into endoluminal space-occupying devices, gastric volume reduction procedures, and devices or procedures to eliminate small bowel absorptive area and regulate gastric emptying (Table 1).
ATIIP, adjustable totally implantable intragastric prosthesis; BIB, BioEnterics intragastric balloon; BMI, body mass index; BTXA, botulinum toxin A; NOTES, natural orifice translumenal endoscopic surgery; TERIS, transoral endoscopic restrictive implant system.
Materials and Methods
An extensive English language literature search was done using PubMed, Medline, and Google to identify peer-reviewed original and review articles or abstracts using the key words "endoscopy," "bariatrics," "endoscopically placed devices or interventions," "endoluminal surgery," "endoscopic instrumentation," "interventional gastroenterology," "laproscopic surgery," and "natural orifice transluminal surgical methods to treat obesity." In this present article we present the data available on the above methods in bariatrics based on our literature review from Jan 2001 to Nov 2011. Studies involving procedures or devices not involving luminal endoscopy were excluded. The mechanism, efficacy in clinical trials when available, limitations, and future prospects are discussed.
Endoscopic Devices or Procedures in Bariatrics
Endoluminal space-occupying devices
The use of space-occupying devices came into practice in the 1980s when the U.S. Food and Drug Administration (FDA) approved the Garran–Edwards gastric bubble. 8 Its use was limited and abandoned because of multiple complications such as gastric erosion and intestinal obstruction.9,10 Experts redefined intragastric balloons to meet the following attributes in order to reduce complications: (1) carry a smooth surface to prevent mucosal ulcerations, (2) contain a marker that can be detected during balloon deflation, and (3) the ability to adjust the balloon with either air or fluid.9,10 The main drawback to intragastric devices was failure to achieve long-term weight reduction.11,12
BioEnterics intragastric balloon system
Despite being one of the earliest devices introduced in 1991, the BioEnterics® (Santa Barbara, CA) intragastric balloon (BIB®) system remains the most durable, applicable, and well-studied device. 13 Although it is not FDA-approved in the United States, its extensive use in Europe has demonstrated great value. 14 The BIB is an air- or saline-filled (400–800-mL) expandable and deflatable intragastric balloon placed endoscopically that mechanically promotes early satiety to decrease food ingestion that aids in behavior and dietary modification . 10 It is indicated in patients with a BMI of (1) between 27.0 and 29.9 kg/m2 in association with severe co-morbidities, (2) 30.0–34.9 kg/m2 with co-morbidities, (3) 35.0–39.9 kg/m2 without co-morbidities, and (4) 40.0 kg/m2 and above for preoperative weight reduction. 13 Systematic reviews including prospective and retrospective studies have shown that the mean weight loss range from 13% to 18% with the majority of weight reduction during the first few months of balloon placement.9,13 BIB is generally safe when balloons are kept in for less than 6 months. 13 There is a risk for balloon deflation and complications such as bowel obstruction and perforations with prolonged use. 13 It is currently used for preoperative weight reduction in superobese patients in preparation for bariatric surgery. Contraindications for balloon placement include hiatal hernias, gastrointestinal bleeding, previous gastric surgery, pregnancy, substance abuse, severe liver disease, coagulation disorders, and any contraindications to endoscopy. 13 In one of the largest retrospective studies, which included 2515 subjects, the mean weight loss was 33.9% at 6 months. 9 Mathus-Vliegen and Tytgat 8 studied the long-term outcomes with BIB with 1 year of balloon treatment and an additional 1 year of balloon-free follow-up; the study suggested that a greater part of weight loss is sustained up to 24 months after initial placement (i.e., for an additional 12 months of balloon-free period). In addition to weight loss, studies have shown resolution or improvement in co-morbidities such as diabetes and hypertension in 52%–100% of patients. 13 A meta-analysis including pooled data from 3,600 patients concluded there is a short-term excess weight loss reduction of 32% with BIB. 15
Heliosphere BAG
The Heliosphere BAG (Helioscopie, Vienne, France) is a radiopaque, spherical intragastric balloon made of polymerized material with a silicone envelope cover (for silicone porosity minimization) (Fig. 1). It has an air-filled double pouch (650–700 mL) with a simplified inflation system but has limitations due to difficult removal. Some prospective studies have reported a weight loss of up to 9% in the 4–7-month follow-up.16–18 It was approved for use in the Europe and Canada in 2004, but the superiority over other devices has not been clearly established. 15

Heliosphere bag. Reproduced with permission of Helioscopie.
Adjustable totally implantable intragastric prosthesis
The adjustable totally implantable intragastric prosthesis Endogast® (Districlass Médical S.A., Chaponnay, France) is a polyurethane air-filled (300-mL) oval prosthesis with permanent implantation. It is implanted by a combined endoscopic and surgical procedure with intragastric and suprafascial fixation using a method similar to that of the percutaneous endoscopic gastrostomy technique. It has a proximal gastric positioning that is aimed at influencing gastric accommodation, electrical activity, and neurohormonal mechanisms that helps with satiety enhancement. In a prospective study involving 57 patients, a mean BMI loss of 7.4%, 8.4%, and 12.2% was reported at 3, 6, and 12 months, respectively. 19 The device is well tolerated with a small proportion of patients having early local subcutaneous infection and late port erosion as seen with percutaneous endoscopic gastrostomies.
Silimed gastric balloon
The Silimed (Rio de Janeiro, Brazil) gastric balloon is a transparent spherical silicon shell (650 mL, saline filled) with a self-sealing valve. The Silimed gastric balloon is advanced by scope traction under direct visualization. A pilot study recruiting 52 patients showed 100% success rates in placement, with short procedure duration and no procedure-related complications. 20 A follow-up study from the same center including 16 patients with a follow-up of 5–6 months showed significant weight loss with the Silimed gastric balloon. 21
Semistationary antral balloon
The semistationary antral balloon (JP Industria Farmaceutica, Ribeirao Preto, Brazil) is a small, pear-sized and -shaped device (150–180 mL, saline filled) that contains a 30-cm silicone duodenal stem at the caudal end used as an anchor to the antrum and a 7-g metallic counterweight tip at the conical pole oriented to the pylorus. 22 It is designed for intermittent occlusion of the pyloric opening that prolongs gastric emptying while stimulating antral and proximal duodenal satiety receptors. 22 A pilot study recruiting 26 subjects showed median weight reduction of 6.5 kg (range, 3.7–19.9 kg) with a median implantation period of 4 months. 22
Butterfly
The butterfly (Wilson-Cook Medical, Winston-Salem, NC) is a long polyethylene ribbon folded into loops that is tightly packed to give a shape of a butterfly. 23 The device is advanced over a plastic tube with a Savary guide wire using an overtube. 23 The experimental device was shown to be safe and effective in two small pilot studies.24,25
Endoluminal gastric restriction
Transoral endoscopic restrictive implant system
The transoral endoscopic restrictive implant system (TERIS; BaroSense, Redwood City, CA) is a restrictive implant consisting of five implants that are placed around the cardia of the stomach in a circular fashion to create a narrow lumen for early satiety. 26 The results of short-term studies by de Jong et al. 26 showed weight loss of 12.3% and 22.2% at 1 and 3 months, respectively. Its mechanism parallels laparoscopic gastric banding with advantages of easy reversibility, and its use is performed as an outpatient procedure. 26 Complications include throat pain, fever, epigastric pain, nausea, vomiting, reflux, and perforation. 26
StomaphyX endoluminal suturing device
The StomaphyX™ endoluminal fasteners and delivery system (EndoGastric Solutions, Redmond, WA) is a FDA-approved device used for transoral tissue approximation and ligation in the gastrointestinal tract. 27 It utilizes polypropylene H-fasteners to create full-thickness pleats of tissue approximation (Fig. 2). 27 Its primary use has been seen in RYGB revision of gastric pouches, leaks, gastrojejunostomy dilatation, and gastrogastric fistula formation.27–29 Although its use as a primary means of endoscopic weight reduction is experimental, it has shown advantages over postoperative laparoscopic revision with excess body weight loss of 10.6%, 13.1%, and 17.0% at 1, 3, and 6 months, respectively. 27 The advantages lie in cost and time reduction in comparison with reoperative bariatric surgery, both open and laparoscopic methods. 27
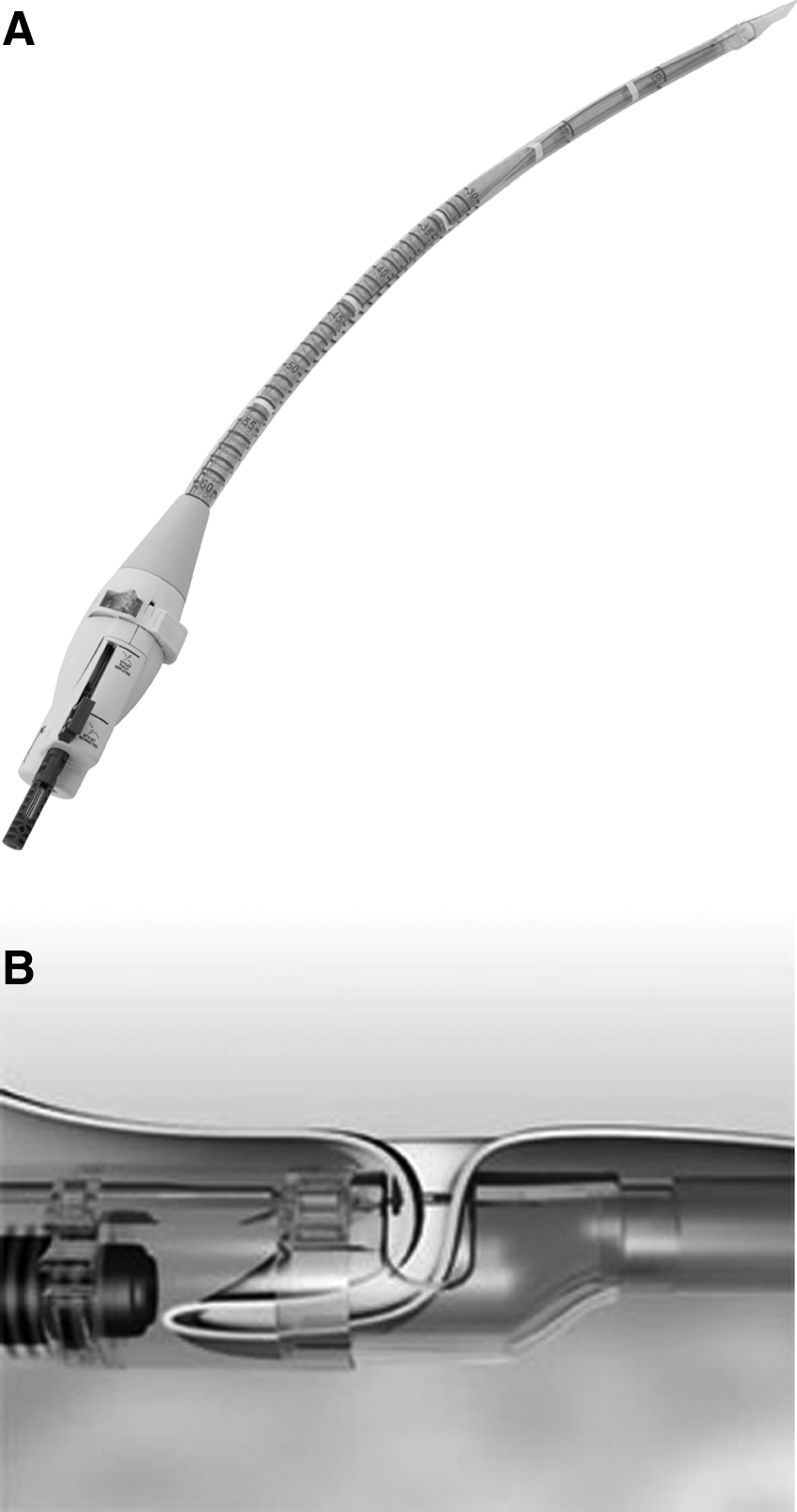
StomaphyX.
EndoCinch suturing system for endoluminal vertical gastroplasty
Endoluminal vertical gastroplasty is a method of surgical weight reduction through gastric restriction. An endoluminal platform such as the EndoCinch™ suturing system (Davol Inc., a division of C.R. Bard, Cranston, RI) that was initially used for the treatment of GERD has expanded its utility to bariatric surgery. 2 The system works by deploying stitches in the anterior and posterior stomach wall from the proximal fundus to the distal body of the stomach to create a vertical gastroplasty resulting in a significant decrease in stomach distensibility (Fig. 3). 30 Fogel et al. 31 showed that the percentage of excess body weight loss was 21% at 1 month and 58% at 12 months. Ongoing clinical trials are currently being done to further refine the technique and long-term durability.
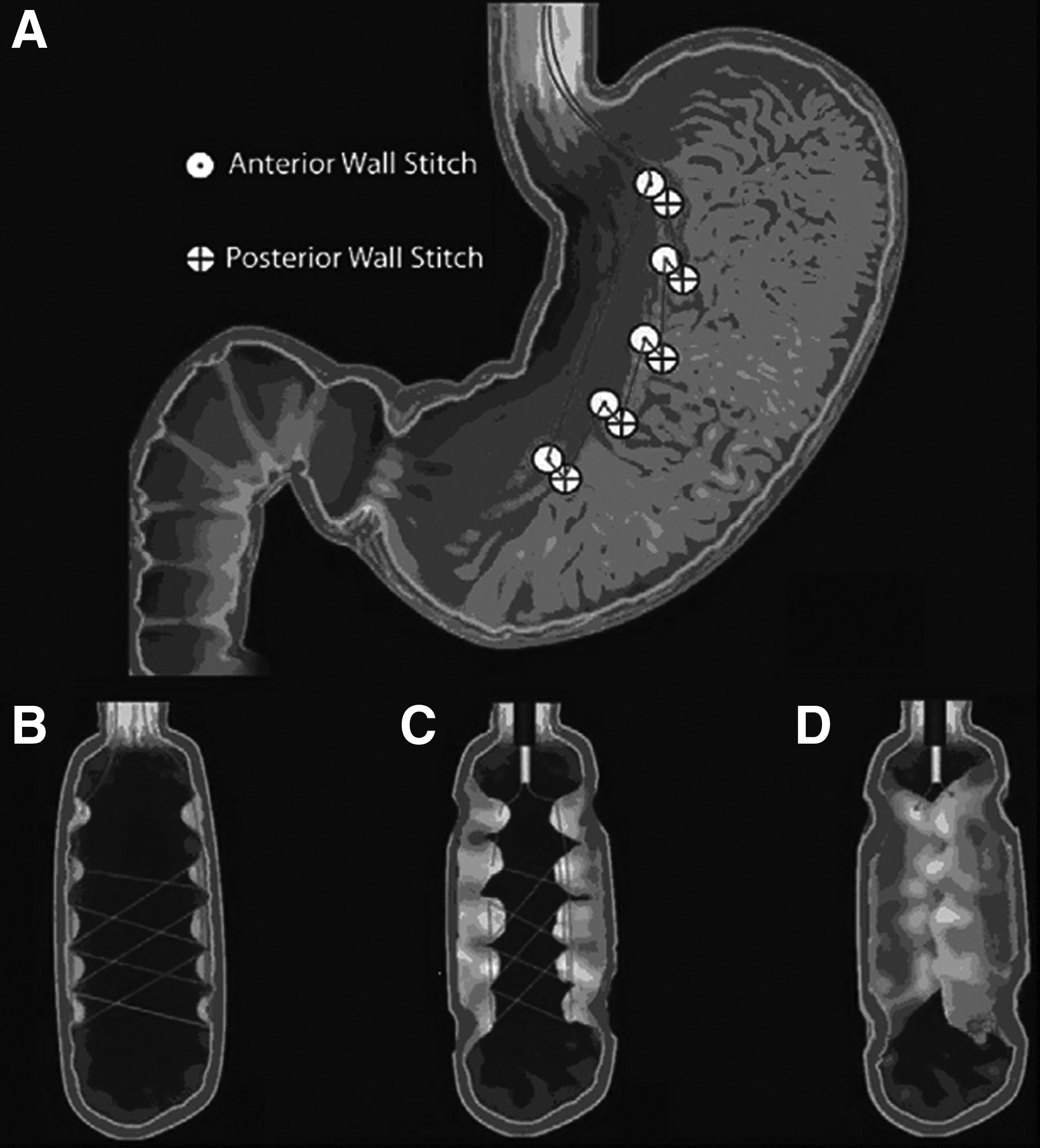
EndoCinch suturing system for endoluminal vertical gastroplasty.
Sleeve stapler for transoral gastroplasty
Transoral gastroplasty is another emerging technique that works by creating a full-thickness plication in the proximal stomach. It uses restriction to induce early satiety and to reduce stomach capacity. 2 The TOGA® sleeve stapler (Satiety Inc., Palo Alto, CA) is a stapling device that enters through the gastric lumen and plicates the anterior and posterior walls of the stomach, creating a restrictive sleeve that extends from the esophagus to the distal lesser curvature (Fig. 4). 2 Preliminary studies showed promising results with weight loss of 17.6%, 24.5%, and 26.5% at 1, 3, and 6 months post-treatment. 32 Follow-up studies found even better results with weight loss of 19%, 34%, and 46% at 1, 3, and 6 months post-treatment. 33 Complications that were seen in human studies included nausea, vomiting, abdominal pain, and transient dysphagia. 32 With further device experience and technique, future use of TOGA may be safer and feasible. In a recently published multicenter study TOGA showed 45% excess BMI loss 12 months after the procedure without severe complications. 34 The role of TOGA appears to be promising.
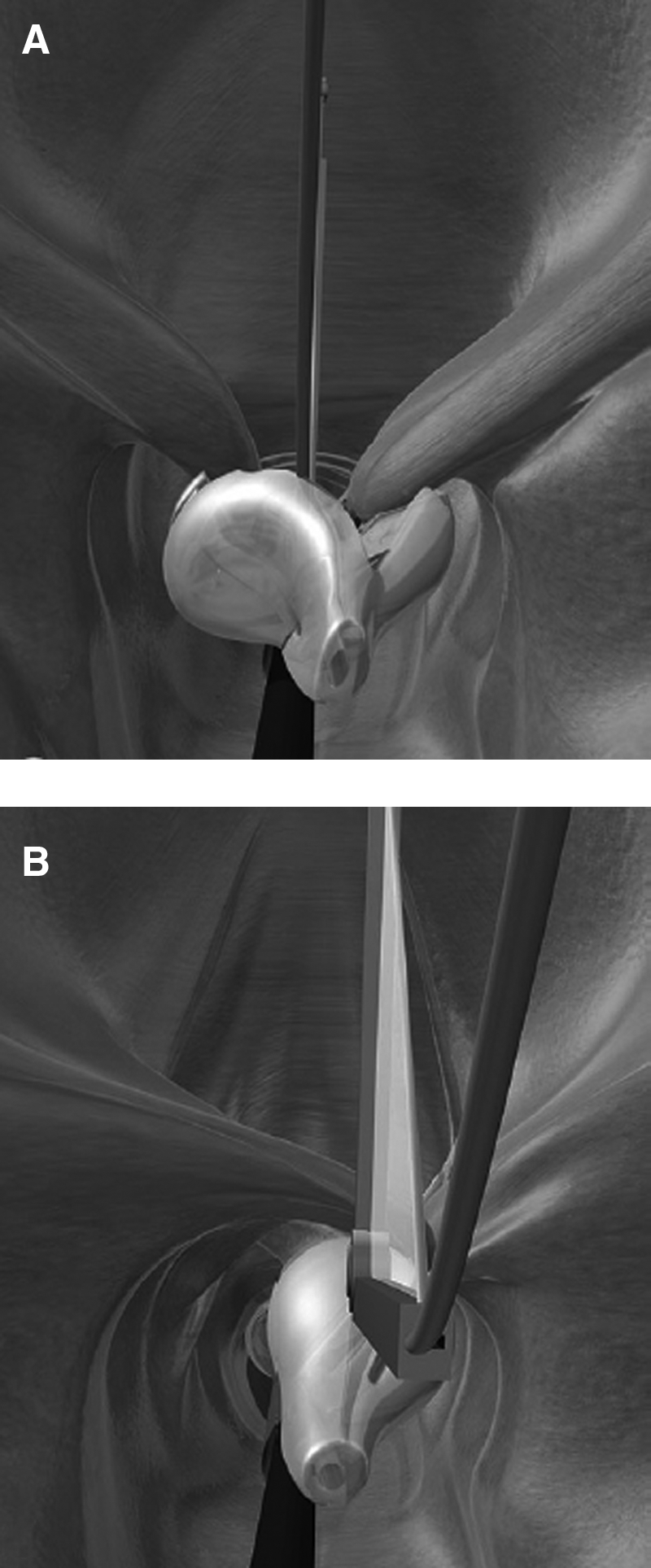
TOGA sleeve stapler for transoral gastroplasty.
Eagle Claw VII
A similar device is the Eagle Claw VII (Apollo Group and Olympus Corp., Tokyo, Japan), which is an endoscopic suturing device that is premounted alongside a standard endoscope. 35 It contains a curved needle that is advanced through an overtube and can be driven into stomach tissue to create intracorporeal knots.35,36 The result is a proximal gastric pouch with a restrictive band at its outlet. The device has been tried in animal models and is currently under investigation in humans.
Butterfly endoluminal gastroplasty
Another investigational endoluminal procedure that uses gastric restriction is the butterfly endoluminal gastroplasty procedure 37 (Wilson-Cook Medical). The butterfly procedure is an endoluminal technique that creates a small gastric pouch to promote restriction similar to endoluminal vertical gastroplasty and adjustable gastric banding. 37 The device is in developmental stages, with a preclinical study suggesting its restrictive characteristics similar to adjustable gastric banding. 38
Eliminating small bowel absorptive area
Duodenojejunal bypass sleeve
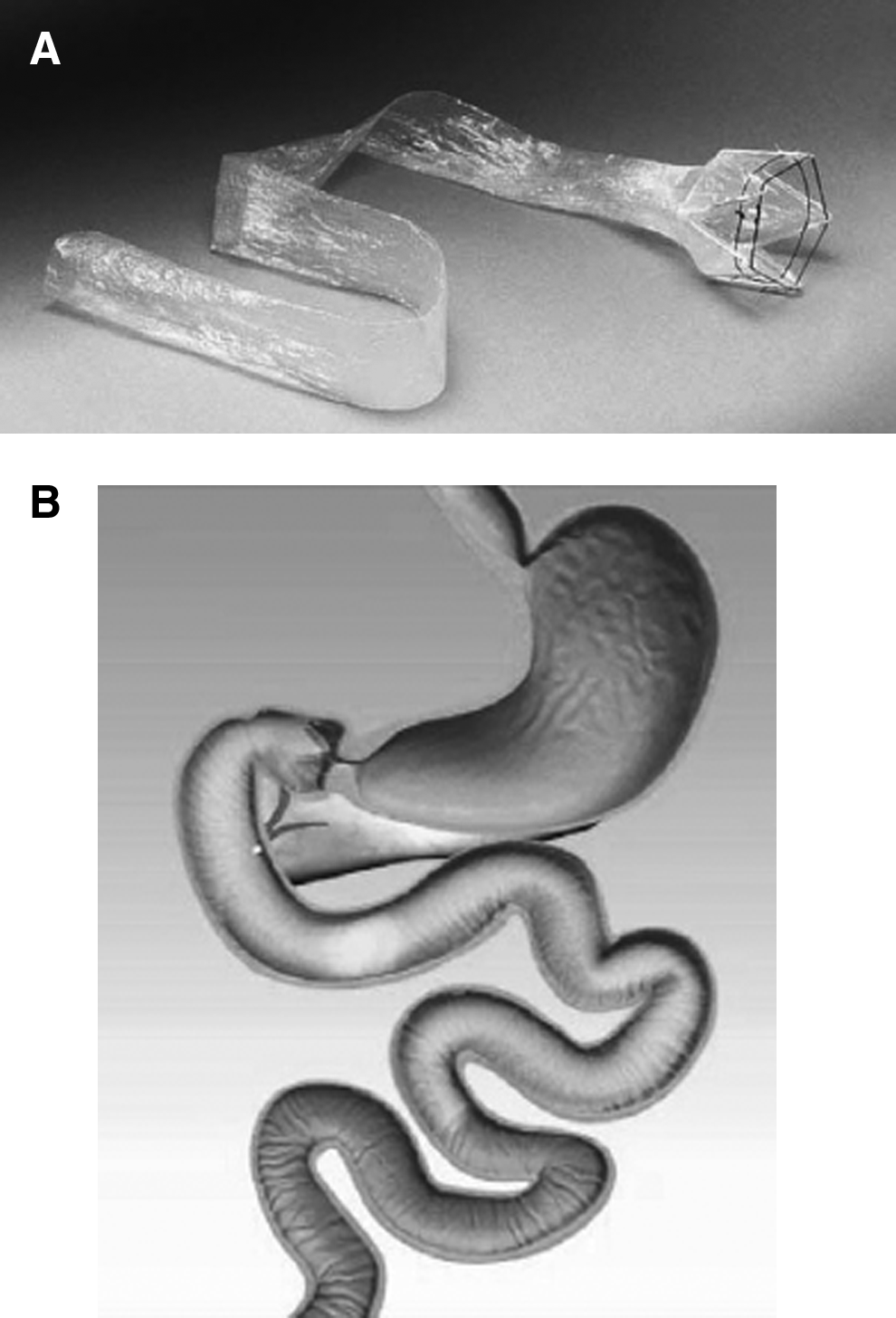
The duodenojejunal bypass sleeve (EndoBarrier®; GI Dynamics Inc., Watertown, MA) is an endoluminal device used to bypass the proximal small bowel. The EndoBarrier is a self-expanding implant that is placed in the duodenum and extends into the proximal jejunum and works by creating a physical barrier to prevent absorption and mixing of digestive enzymes (Fig. 5).2,39 It is placed endoscopically with fluoroscopic guidance to confirm appropriate device placement. 39 In a sham-controlled trial, Gersin et al. 40 showed more than 10% excess weight loss. In animal studies, Tarnoff et al. 41 proposed its potential as a novel treatment for type 2 diabetes by altering the incretion pathway by changing glucagon-like peptide-1 and other signals that affect gastric emptying. Similarly, Aguirre et al. 42 evaluated the duodenojejunal bypass sleeve in rats, showing substantial weight loss and effect on glucose homeostasis with diet-induced obesity. They proposed that the duodenojejunal bypass sleeve can decrease fasting blood glucose and insulin levels, which may in turn alter hepatic glucose output. These preliminary studies in animal studies show promising potential in weight reduction and with metabolic syndrome.
Gastrointestinal sleeve device
The ValenTx endoluminal bypass (ValenTx Inc., Carpinteria, CA) is an implantable sleeve that works as an artificial conduit to bypass the stomach and small bowel. The device acts to mimic the effects of the traditional RYGB by restricting the amount of food intake, excluding food from the stomach and small bowel, and leaving undigested food exposed to the jejenum. It is implanted endoscopically beginning at the gastroesophageal junction with extension to the jejunum. Ongoing clinical trials are underway that have shown some promising results with an average excess weight loss of 39.5% in a 12-week trial. 43
Natural orifice translumenal endoscopic surgery via gastrojejunal bypass
Weight reduction via endoscopy is a novel field with new approaches. Natural orifice translumenal endoscopic surgery (NOTES) utilizes flexible endoscopy performed a natural orifice to reach the lumen of the gastrointestinal tract. 37 Its use is expanding with potential for reducing complications such as surgical site infections, time, and cost. 37 Swain's endoscopic “sewing machine,” marketed as the EndoCinch suturing system (Davol Inc.), showed great potential with its success in the treatment of GERD. 37 Kantsevoy et al. 44 demonstrated the technical feasibility of creating a gastrojejunal anastamosis endoscopically in a porcine model. Its practical use has been studied for bariatric surgery, but human studies are still lacking. The technique involves passage of a flexible endoscope into the stomach with penetration of the stomach wall into the peritoneal space. In the peritoneal cavity, a loop of small bowel is retracted into the gastric lumen to create a gastrojejunostomy. 44 Similar newer platforms are being developed with innovative flexible endoscopy with ShapeLock™-based technology (USGI Medical, San Clemente, CA) that allows for improved stability and versatility.36,45 Its utility is being explored for presurgical, postsurgical, and primary weight loss reduction. Current limitations with NOTES are risk of iatrogenic injury due to limited working space leading to complications including infection, bleeding, visceral injury, anastomotic or entry site leaks, and adhesions.
Regulating gastric emptying
Gastric electrical stimulation
Gastric electrical stimulation is a well-known technique used in patients with gastroparesis. However, its use in obesity is currently being investigated with promising results. The abiliti® (Intrapace Inc., Menlo Park, CA) and the Transcend® implantable gastric stimulation (Transneuronix, Mt. Arlington, NJ) systems are gastric pacing devices that are delivered endoscopically to regulate gastric emptying. 36 Shikora et al. 46 showed that an implantable gastric stimulation device can lead up to an excess weight loss of greater than 30% at a mean follow-up of 29 months. Some limitations included technical difficulties such as lead dislodgement and failed circuit conduction. 46 The effect on obesity is preliminary but adds a new dimension to endoscopic management for primary weight reduction.
Endoscopic injection of botulinum toxin A
Many studies have shown the usefulness of botulinum toxin A (BTXA) in the treatment of achalasia and gastroparesis. 47 However, its use in obesity is novel. Foschi et al. 48 studied the use of BTXA for the treatment of obesity in a randomized, double-blind, controlled study. They hypothesized that intraparietal administration of BTXA in the antrum and fundus of the stomach of obese patients would reduce gastric emptying, increase satiety, and induce weight loss. Their results showed that BTXA patients had a significant higher weight loss, BMI reduction, greater prolongation in gastric emptying time, and higher satiety visual (analogic) scale value compared with control groups through 8 weeks of treatment. They proposed that BTXA may play an important role in altering the level of ghrelin and sensory activity of the intestine in regulating total gastric capacity and emptying. The attractive benefit to intraparietal injection of BTXA is its safety and lack of significant side effects.
Other modalities
Ablation devices: sclerotherapy and radiofrequency electrocoagulation
The role of ablation as a primary means of surgical weight reduction has not been well developed. However, the use of sclerotherapy in postsurgical revision has been characterized in a few studies.49,50 Its use may have a prominent role in postsurgical revision as well as primary weight reduction in future studies.
Potential futuristic devices
Polymer pill
The polymer pill (BaroNova Therapeutics, Inc., Foster City, CA) is an expandable pill that is ingested or delivered endoscopically and that works by endoluminal restriction. It works to occupy space in the stomach for up to 1 week before biodegradation and passage through the gastrointestinal tract. It has the potential to be dose-titrated to achieve the desired effect of weight reduction; however, its use has not been clinically tested. 51
Preoperative Endoscopic Evaluation
As per the American Society for Gastrointestinal Endoscopy 52 and the European Association for Endoscopic Surgery, 53 the role of a routine esophagogastroduodenoscopy prior to bariatric surgery is imperative to detect upper gastrointestinal abnormalities. Because obesity is shown to be associated with a significantly increased risk of GERD, erosive esophagitis, and esophageal adenocarcinoma, endoscopic evaluation is important to detect such abnormalities preoperatively, especially in symptomatic patients. 54 Studies have shown positive findings including esophagitis, erosive gastritis, gastric ulcers, and hiatal hernia in as high a percentage as 75%–80% of subjects on preoperative endoscopy, a high proportion of which were seen in asymptomatic patients.55,56 The impact of these positive findings on the management plan has not been systemically evaluated.
It is important to remember that some operations done for obesity, for example, RYGB and sleeve gastrectomy with duodenal switch and biliopancreatic diversion, make parts of the gastrointestinal tract very difficult to access after the surgery. Also, in patients undergoing laparoscopic adjustable gastric banding the presence of a hiatal hernia is associated with higher rates of band slippage and might warrant alternative bariatric intervention. It is thus highly recommended to perform a preoperative examination of the upper gastrointestinal tract especially in these settings.
There have been concerns regarding the safety of endoscopy under sedation in morbidly obese patients due to a high incidence of hypoxia related to sleep apnea. Appropriate risk stratification and endoscopy under monitored anesthesia care are suggested approaches to prevent complications. 57 In high-risk patients alternative modalities such as upper gastrointestinal series and noninvasive Helicobacter pylori testing may be useful.
Intraoperative Endoscopic Evaluation
Endoscopic evaluation has been shown to assist the surgeon to immediately assess staple lines for hemorrhage, evaluate pouch size, measure stomal diameter, and test for integrity of the gastrojejunal anastomosis and pouch to help prevent early postoperative leaks in cases of RYGB. 58 Intraoperative pneumatic leak testing of gastrojejunal anastomosis during RYGB may help in reducing the incidence of postoperative leaks. 59
Endoscopy in Postbariatric Suergery Complications
Bariatric surgeries are associated with complications such as bleeding, infection, anastomotic leaks, anastomotic strictures, and marginal ulcers, which may occur early or late in the postoperative course in up to 40% of patients. 58 Endoscopy is valuable in evaluation of symptoms and signs in postbariatric patients and also helps in endoscopic management of many of the complications,thus avoiding a complex surgery (Table 2).58–66 The need for surgical revisions after failures in gastric bypass have been relatively common with gastrogastric fistula formation, dilated pouch, and dilated gastrojejunostomy. 49 Dilated gastrojejunostomy is a known complication of RYGB that occurs in 2%–4% of patients that can lead to loss of restriction and dietary excess.49,50 Spaulding 50 used sodium morrhuate as a sclerotherapeutic agent to decrease the size of gastrojejunostomies in patients with dilated gastrojejunostomies after RYGB.
Staple line disruptions and leaks usually need surgical intervention but have been managed endoscopically at some centers using partially covered self-expanding metal stents, Polyflex® (Boston Scientific, Natick, MA) stents, argon plasma coagulation, endoscopic clips, and fibrin glue.
Conclusions
At present the role of endoscopy is valuable in preoperative evaluation as well as recognition and management of many postoperative complications in bariatrics. Evolution of endoscopic methods in weight loss procedures also seems promising. Currently, clinical results with intragastric balloons, especially the BIB system, are the best studied. Endoscopic gastric volume reduction procedures using the EndoCinch suturing and TOGA sleeve stapler systems have shown good results in preliminary studies, but further studies are needed to determine their usefulness. Several other methods, such as use of an EndoBarrier or injection of BTXA, are under investigation. None of these endoscopic devices or procedures is currently approved by the U.S. FDA. Investigational use of these treatments or any other devices in development should only be provided through a multidisciplinary strategy and within a dedicated weight loss program. At present, the clinical utility of endoscopic procedures or devices is limited to preoperative weight loss in morbidly obese subjects who are not otherwise surgical candidates. Future research will open areas for widened clinical utility of these devices.
Footnotes
Disclosure Statement
No competing financial interests exist.