
Abstract
Abstract
Background:
Leakage from the clipped cystic duct stump (cystic duct stump leak [CDSL]) as a cause of biliary peritonitis has not been emphasized enough. It deserves special mention because it is not an uncommon cause and it is easier to treat. With the advent of laparoendoscopic single-site (LESS) cholecystectomy, its occurrence in relation to other causes of biliary peritonitis needs reexamination.
Subjects and Methods:
Details of 756 patients undergoing LESS cholecystectomy were analyzed, and patients presenting with biliary peritonitis were identified. The investigative profile included an ultrasound, contrast-enhanced computed tomography scan, and endoscopic retrograde cholangiopancreatography (ERCP) to identify the site of leak. The management in addition to stenting included abdominal tube drainage.
Results:
There were 5 (0.66%) patients, all female, with biliary peritonitis, and 4 of them (0.53%) had cystic stump leakage as identified by ERCP. The usual time of presentation was in the first week after surgery, with acute abdominal pain and vomiting. Common bile duct stenting was carried out, after choledocholithotomy where required, at the same ERCP session. Tube abdominal drain was required in 2 patients, and 1 patient had to undergo exploratory laparotomy for an associated acute intestinal obstruction. All the patients recovered completely. The stent was removed between 4 and 6 weeks after ERCP.
Conclusions:
Effective CDSL management requires early recognition and management. ERCP is the cornerstone for correct identification, and common bile duct stenting was curative in all patients.
Introduction
Subjects and Methods
Retrospective and prospective data of all patients undergoing LESS cholecystectomy from December 2009 to December 2011 were reviewed for cystic duct leaks. The analysis of these patients included available data on the pathological state at presentation, associated co-morbidities, operative details, clinical details of postoperative presentation, and investigations for their identification. Prospectively the investigations included a hepatobiliary profile, a hemogram, an abdominal ultrasound (US), contrast-enhanced computed tomography (CECT), and, if required, ERCP. All the patients were operated on by the same surgeon. Transumbilical single-incision multiple-port laparoscopic cholecystectomy was performed using routine laparoscopic instruments. A superior one-third transumbilical flap was raised and undermined for 1–2 cm. A centrally placed 10-mm flap valve trocar and two flanking 5-mm tube trocars were inserted through separate transfacial punctures, in the same transverse line. The cystic duct was clipped three times with LIGACLIP® (Ethicon) clips and transacted (cut) with two clips on the proximal cystic duct stump in all patients. Endoloops or intracorporeal knots were not used. The drain was not left in any patient except in the patient with peroperatively diagnosed right hepatic duct injury, which was repaired laparoscopically with 3-0 Vicryl® (Ethicon) sutures.
Patients readmitted with biliary peritonitis after the initial assessment with US/CECT were followed with daily US, and where there was collection of more than 500 mL, a Morrison's pouch drain was inserted under US control. Five hundred milliliters was kept as the cutoff point because lesser collections usually get absorbed completely. Patients with an increasing collection or persistent tube drainage underwent ERCP with or without choledocholithotomy (CDL) and stenting with an FG (French size) 7–10 stent. The stent was removed anytime after the fourth week. Intraoperative cholangiography was not carried out in any patient.
Results
LESS cholecystectomy was performed in 756 patients. There were five (0.66%) records of biliary peritonitis, and all were in females. Four of the patients had acute cholecystitis, 1 patient had gallbladder empyema, and 1 patient presented with chronic cholecystitis (Table 1). The cystic duct was edematous in all patients with acute cholecystitis and empyema. The right hepatic duct was injured during surgery in 1 patient; this was fortunately discovered peroperatively and repaired immediately. The remaining 4 (0.53%) patients (or 80% of those with biliary peritonitis) had CDSL (Table 1). Preoperatively none of the patients had a common bile duct (CBD) stone on US and CECT, and only 1 patient's serum bilirubin level was raised to 2.79 mg%. In this patient levels of the liver enzymes aspartate aminotransferase and alanine aminotransferase were raised, and the level of alkaline phosphatase was marginally raised. Total and differential leukocyte counts showed polymorphonuclear leukocytosis in 3 patients (Table 2).
LESS, laparoendoscopic single-site.
Patient 4.
Patient 1.
Co-morbidities of diabetes and hypertension.
CBD, common bile duct; CT, computed tomography; TLC, total leukocyte count; DLC, differential leukocyte count; P, polymorphs; Gb, gallbladder; Hb, hemoglobin; TLC, total leukocyte count; US, ultrasound.
Three patients with CDSL presented between 3 and 4 days postoperatively, and 1 patient presented on Day 18. The presenting symptom in all patients was abdominal pain starting in the right hypochondrium, then becoming generalized and accompanied by generalized abdominal tenderness and guarding. Three patients presented with various degrees of generalized abdominal distension (Table 3).
At the time of readmission all the patients except Patient 3 had a raised polymorphonuclear count, and serum bilirubin was marginally raised in all patients compared with the preoperative levels (Table 4). US/CECT in 2 patients showed a generalized fluid collection, 1 patient had collection in the right subphrenic and lesser sac, and 1 patient had fluid collection only in Morrison's pouch. CBD stone was reported in 2 patients, while the CBD was reported as normal in the rest. ERCP with stenting was done only in patients presenting with persistent drainage of more than 200 mL/day because lesser drainage output usually stops by itself. ERCP had to be performed in all patients and showed partial cystic stump leak in 3 patients (Fig. 1) and total CDSL in 1 patient. The timing of ERCP relative to the time of presentation with biliary peritonitis is shown in Table 4. All patients were stented with an FG 7–10 stent. In 2 patients an US-guided abdominal drain was inserted, in 1 patient a pelvic drain was used, and in the remaining patient it was in the left hypochondrium (Table 5). Patient 3 only required ERCP and stenting, while the fourth patient developed adhesive acute intestinal obstruction, secondary to biliary peritonitis, on postoperative Day 9 for which an exploratory laparotomy had to be done. The area of the Morrison's pouch and around the CBD was not disturbed because of dense adhesions, and a pelvic drain was left for drainage. The subsequent course was uneventful in all the patients, and CBD repair was not required in any patient. The discharge time was 1–7 days, and the stent was removed at between 4 and 6 weeks (Table 6).
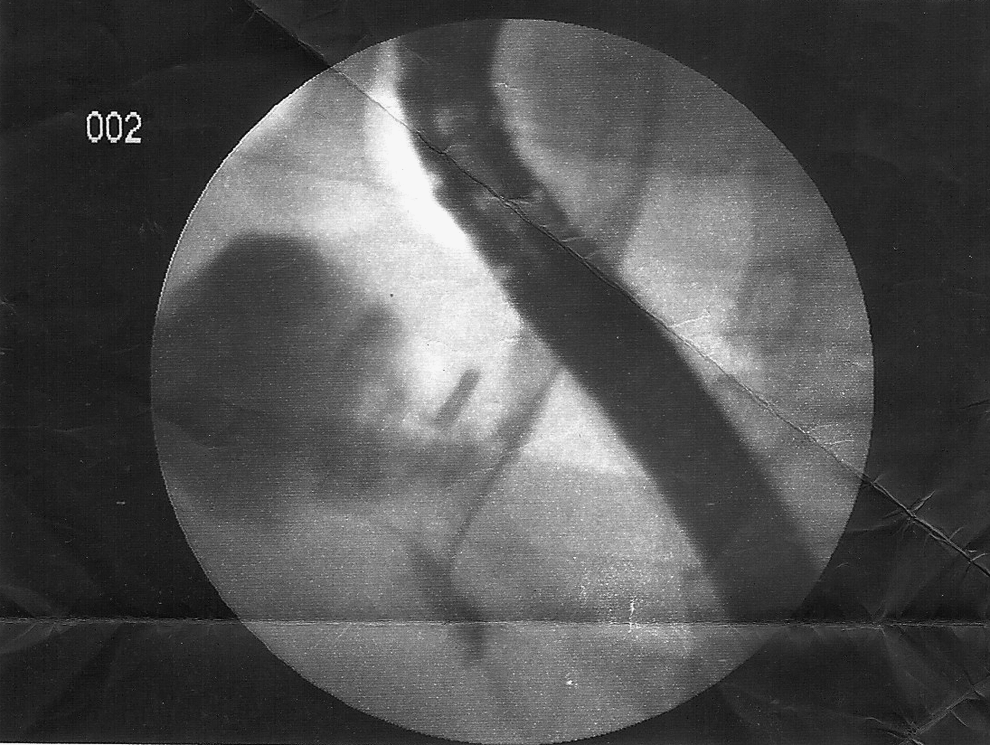
Common bile duct stent in place. The open cystic duct is seen as the dark shadow.
AIO, acute intestinal obstruction; ERCP, endoscopic retrograde cholangiopancreatography.
CDL, choledocholithotomy.
ERCP, endoscopic retrograde cholangiopancreatography.
Discussion
Post-laparoscopic biliary peritonitis, manifesting in any form, is a serious complication and requires urgent diagnosis and management to offset the associated morbidity and mortality. CDSL forms an important subgroup of this complication and has been classified as Strasberg Type A, 3 and may occur because of a number of reasons. The causes of CDSL include clip displacement, cystic duct necrosis, elevated CBD pressure, and of course a missed or unrecognized perioperative cystic duct injury. 4 Elevated CBD pressure transmitted to the cystic duct and resulting in cystic stump blowout forms an important cause of CDSL. The pressure increase may follow either a preoperatively missed CBD stone or because of a migrated CBD stone during gallbladder manipulation. In two of our patients there were CBD stones seen on postoperative ERCP. None of these patients had any CBD stones reported preoperatively, nor was there any index of suspicion favoring the presence of CBD stones. CBD stones alone may not be the only reason for the increase in CBD pressure and subsequent leakage because an optimally clipped cystic duct can withstand pressures of as high as 300 mm Hg. 5 It thus appears that there must be, in addition, an associated cause favoring the slippage of the clips. The fact that 3 out of 4 patients had acute cholecystitis may further this explanation, where the subsidence of the cystic duct edema may have resulted in clip slippage because of loosening, or there may have been clip-induced necrosis.
In all the patients with CDSL, there was polymorphonuclear leukocytosis, and the bilirubin was only marginally raised. In the absence of CBD block the elevated serum bilirubin is probably because of peritoneal absorption, and the leukocytosis because of a low-grade infection. Serum bilirubin levels have been reported to be elevated in 29% of patients, 6 and aspartate aminotransferase, alanine aminotransferase, and alkaline phosphatase to be elevated in up to 60%–70% of patients with CDSL. 7
The average time of presentation of CDSL is between 3 and 4 days postoperatively6–8 as in our patients except in one who presented at 18 days postoperatively. However, on proper evaluation it could be ascertained that the patient did have pain with feeling of distension of abdomen on postoperative Day 5, which she attributed to her persisting dyspepsia, and she reported back only after her distension and generalized abdominal pain had increased.
US and CECT are not very useful in diagnosing the site of the leak and providing information regarding the state of CBD and amount of fluid collection in the abdomen. ERCP is more informative and provides a more complete information about the CDSL in the majority of patients.1,8,9 In our series, too, the patients were correctly diagnosed and stented after ERCP. Magnetic resonance cholangiopancreatography too has shown a diagnostic sensitivity of 95% and specificity of 100% for biliary leaks but a 70% accuracy in pinpointing the site. 10 Magnetic resonance cholangiopancreatography may be advantageous in a CBD stricture or block, especially where ERCP fails to demonstrate the proximal biliary channel, but the drawback is that because it is noninvasive it cannot be therapeutic.
Management of CDSL leaks is best done by a CBD stenting that bridges the leakage site and facilitates the bile flow across the ampulla. Complete cure rates have varied from 94% 7 to 100%.6,9 The stent most commonly used is 7–10 FG size and is removed from any time from 4 to 6 weeks after placement.11,12 In our patients, too, ERCP with CDL, where required, and stenting was curative in all patients, and none of the CDSLs required any formal closure. In 1 patient ERCP and stenting were delayed for 10 days after readmission because of the fluctuating clinical and US evidence of amount of peritoneal fluid. Post-stenting, all patients had stoppage of leakage from the stump by Days 4–7 (Table 6). This agrees with the value of 6.8 days (range, 1–28 days) as reported by Li and Liu. 11 Endoscopic sphincterotomy has also been advocated as an additional procedure along with ERCP but is not universally accepted as a necessity. 13 However, it may be advocated in patients with associated spasm or narrowing of the ampullary end of the CBD. Formal corrective surgery for CDSLs by laparotomy or relaproscopy was not required in any of our patients. One of our patients did require laparotomy for related adhesive acute intestinal obstruction. Wise Unger et al. 7 and Woods et al. 6 have reported laparotomy or relaproscopy for CDSL ligation or clipping in their series. Alternative methods tried from time to time have ranged from endonasobiliary drains9,12 to percutaneous transhepatic biliary drainage14,15 to sealing with cyanoacrylate. 16
The problem of CDSL may in great part be offset by tying the cystic duct instead of clipping it, at least in those patients with edema of the cystic duct, wide cystic duct, or where cystic duct cut-through has occurred because in these patients postoperative cystic duct leakage is a distinct possibility.
All our patients recovered after the above management and were discharged within 3–4 days after the stenting with or without drainage of abdominal collection. One patient in whom laparotomy was required was discharged on Day 7.
So is there a difference in the incidence of CDSL after LESS cholecystectomy. We had an incidence of 0.53% biliary leaks, and 80% were CDSL. There are no publications of biliary leaks or of CDSL after LESS cholecystectomy in the literature to date. However, reports of complications after standard cholecystectomy cite an incidence of biliary leaks varying from 0.6% 2 to 1.0%.1,17 The incidence of CDSL has been reported as 0.12% to 0.26% 4 and as 31% of all biliary complications. 6 Our figure of 80% incidence of CDSL is high compared with all studies to date, although the total incidence of biliary peritonitis matches the reported figures. The high incidence of CDSL can be attributed to the CBD stones found postoperatively in 2 patients, which were either missed preoperatively or dislocated peroperatively. In the report by Pinkas and Brady 18 remnant CBD stones were reported and extracted in 20% of patients post-SLC.
Although there is no apparent change in the total incidence of biliary complications in LESS cholecystectomy compared with SLC, the incidence of CDSL as 80% of all biliary complications after LESS cholecystectomy in our series is significant. This is because it is much higher than reported after SLC and thus needs further longer and larger follow-up. What also needs to be considered is whether there is a shortcoming in the clip application on the cystic duct in LESS cholecystectomy.
Thus our protocol for managing any patient presenting with acute pain in the post-laparoscopic cholecystectomy period starts with an immediate evaluation with US or CECT along with hepatic biochemistry and total and differential leukocyte counts. A collection in and around the Morrison's pouch is evaluated with an abdominal US on a daily basis, and a right Morrison's pouch drain is introduced in persisting collections of more than 500 mL. An increasing collection of fluid in the abdomen or persistent drain output of more than 500 mL in a 24-hour period is an indication for an ERCP evaluation, and CDL and stenting are carried out if required. This was completely curative in all patients.
Footnotes
Disclosure Statement
No competing financial interests exist.