
Abstract
Abstract
Background:
The main surgical methods used for the diagnosis of unknown ascites are laparotomy, laparoscopic exploration, and natural orifice translumenal endoscopic surgery (NOTES). This article introduces a novel method: transumbilical endoscopic exploration and biopsy.
Patients and Methods:
From September 2009 to January 2012, 11 patients with unknown ascites were scheduled for transumbilical endoscopic exploration and biopsy at the First Affiliated Hospital of Harbin Medical University, Harbin, China. After the patient underwent general anesthesia and artificial pneumoperitoneum, a 1.0-cm trocar was placed at the umbilical region. After initial observation of the whole peritoneal cavity with a laparoscope, a sterile endoscope (gastroscope) was put through the trocar. The surgeon regulated the depth of insertion of the endoscope and the direction of the trocar, while the endoscopic physician was in charge of turning the camera lens of the endoscope, controlling the biopsy forceps, irrigation, and suction. After exploration, four to six pieces of tissues were obtained for biopsy.
Results:
These patients were diagnosed by endoscopic exploration and pathological examination: 3 cases were tuberculous peritonitis, 2 cases were malignant peritoneal mesotheliomas, 2 cases were peritoneal carcinomatosis, 1 case was a small intestinal tumor, 2 cases were advanced ovarian cancer, and 1 case was cirrhosis.
Conclusion:
Transumbilical endoscopic exploration and biopsy is an easy, practical, and effective method for the diagnosis of unknown ascites.
Introduction
Patients and Methods
Patients
From September 2009 to January 2012, 11 patients with unknown ascites were scheduled for transumbilical endoscopic exploration and biopsy at the First Affiliated Hospital of Harbin Medical University, Harbin, China. Their ages ranged from 36 to 72 years, with an average age of 53.82 years; 7 patients were male, and 4 were female (Table 1). The patients were diagnosed with ascites. However, the etiology could not be defined by computed tomography, ultrasonography, gastroscopy, colonoscopy, cytological pathology, carcinoembryonic antigen, or carbohydrate antigen 19-9 tests. Surgical exploration was considered only under the condition that the course of disease was over 2 weeks, a diagnosis was not possible, and the disease was progressing. Therefore, the decision to undergo exploration and biopsy through transumbilical endoscopy represents an option of last resort.
The contraindications for the procedure are as follows: serious heart and lung dysfunction, unsteady hemodynamics, serious blood coagulation disorders, severe hepatosis, severe infections in the peritoneal cavity, multiple abdominal operations with extensive adhesion, mechanical or paralytic intestinal obstructions, and late pregnancy.
Operative procedure
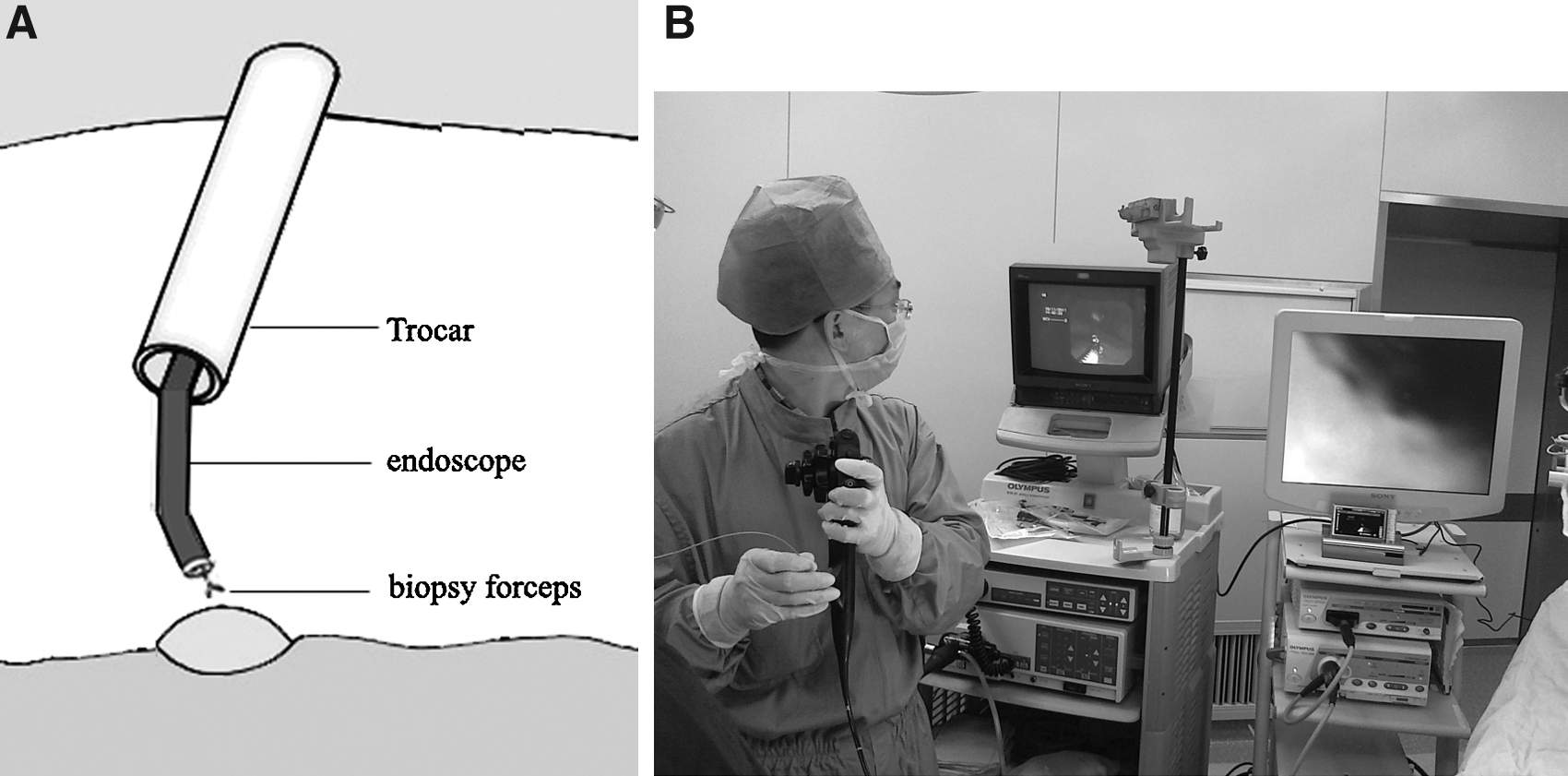
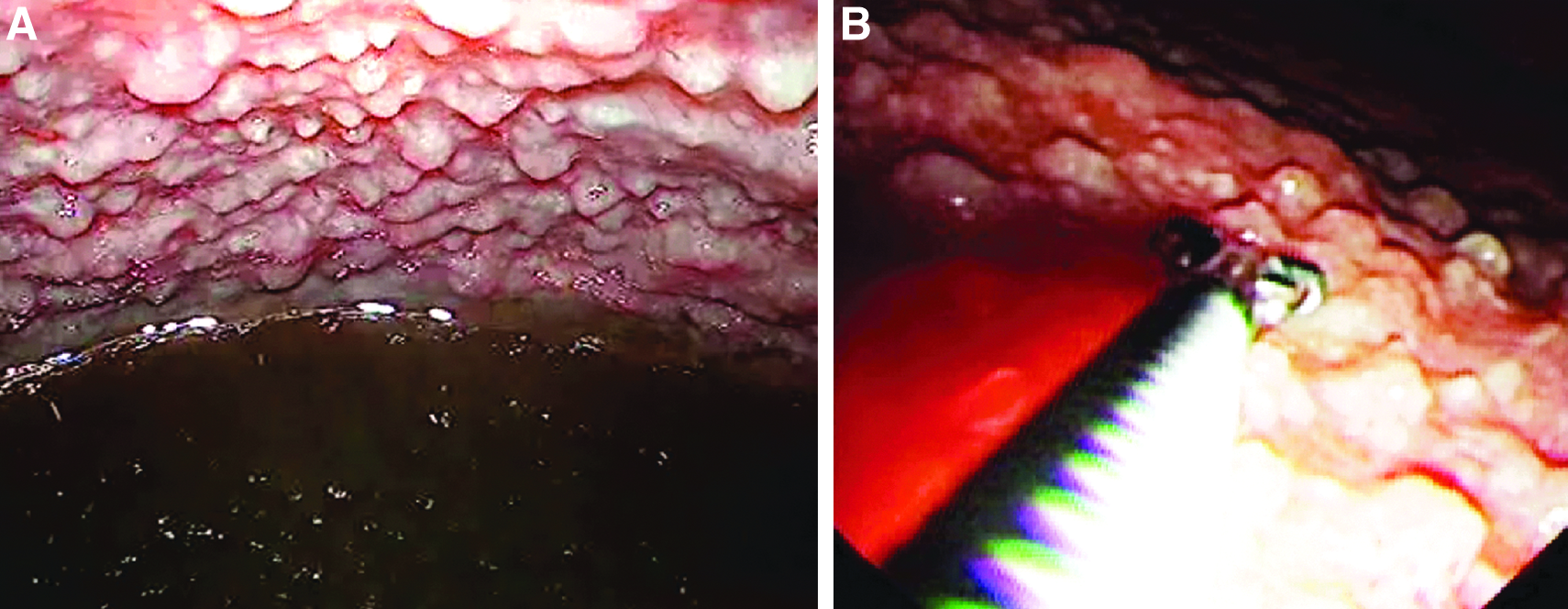
The patients were required to fast for 12 hours before the operation. After the patients was administered general anesthesia, a 1.0-cm incision as made in the umbilical region; after artificial pneumoperitoneum (the pressure was usually 10–15 mm Hg, where 1 mm Hg=0.133 kPa) was induced, a 1.0-cm trocar was placed. A laparoscope was inserted through the trocar to observe the entire peritoneal cavity, then the laparoscope was withdrawn, and a sterile endoscope (gastroscope, sterilized by low-temperature hydrogen peroxide plasma) was inserted through the trocar. The surgeon regulated the depth of insertion of the endoscope and trocar direction, while the endoscopic physician was in charge of turning the camera lens of the endoscope, controlling the biopsy forceps, washing, and suction (Fig. 1). The endoscope was first inserted under the surface of the ascitic fluid to suck the ascitic fluid. Then, using the endoscope for visualization, four to six pieces of tissue were caught by biopsy forceps through the biopsy hole of the endoscope (Fig. 2). The extent of bleeding was then carefully observed; in the case of continuous bleeding, thrombase was sprayed locally, or electrocoagulation was performed.
Results
There were 11 cases of unknown ascites, which were diagnosed by endoscopic exploration and postoperative pathological examination: 3 cases were tuberculous peritonitis, 2 were malignant peritoneal mesotheliomas, 2 were peritoneal carcinomatosis, 1 was a small intestinal tumor, 2 were advanced ovarian cancer, and 1 was cirrhosis.
As follow-up treatment, 3 patients were scheduled for antituberculosis treatments, 6 cases underwent chemotherapy, 1 case received hepatoprotective treatment, and 1 case underwent small bowel tumor excision (Table 1).
Discussion
Regarding ascites of unknown etiology, surgical exploration is the last resort in terms of diagnostic methods. 2 Exploratory laparotomy was wildly popular in the past, but this technique involves more injuries and more complications. In recent years, exploratory laparoscopy has been developed to be a minimally invasive surgery. Because of the need for one observation hole of 1.0 cm and two operation holes of 0.5 cm, at least three trocars were inserted. 3
Along with the development of digestive endoscopy, the endoscopic physician could diagnose and treat many diseases that needed to be performed by a surgeon in the past, such as endoscopic mucosal resection, endoscopic submucosal dissection, and endoscopic retrograde cholangiopancreatography. Since the conception of NOTES has been put forward, endoscopic surgery has been developed to a new level. 4
The main approach for NOTES is as follows:
1. Transgastric: Kalloo et al.
5
in 2004 first described peritoneal cavity exploration and liver biopsy with the use of a gastroscope.6,7 2. Transcolonic: Fong et al.
8
in 2007 completed the feasibility study for transcolonic peritoneoscopy in animals; this approach was then used in the clinic.9,10 3. Transbladder: Lima et al.
11
in 2006 researched the technique's feasibility and safety for use in the bladder in animals for NOTES, and clinical trials were reported by Gettman and Blute
12
in 2007. 4. Transvaginal: Animal experiments in 2007 were followed by transvaginal NOTES.13,14
The technique allows physicians to explore and operate in the pelvic cavity by the transgastric approach. It is notable that it is practical to explore the epigastric cavity by transcolonic and transvaginal approaches. However, the possibility of peritoneal cavity infection represents a challenge for those who wish to perform transcolonic NOTES. Whether reproductive function may be influenced by a tranvaginal operation remains to be elucidated. Slim and Launay-Savary 15 reported a study of 121 people who underwent NOTES cholecystectomy; 117 (94%) were unwilling to undergo a surgery using the transvaginal approach. Therefore the potential risks and advantages must be evaluated strictly in order to find the optimal operative approach.
The umbilicus is a natural scar left over after closure of a natural orifice; therefore, the transumbilical incision can be hidden by skin ruga with only minimal scar formation.16,17 More and more reports on transumbilical single-port laparoscopic surgery can be found in recent years involving the use of a laparoscope and instruments inserted through a special trocar (TriPort or R-port [Advanced Surgical Concepts, Wicklow, Ireland] or Uni-X [Pnavel Systems, Inc., Morganville, NJ]) at the umbilical region. The transumbilical endoscopic approach taken here has the following advantages. It is simple and rapid and involves less frequent infection. Lighting, observation, biopsy, and certain simple treatments could be completed through a single port, so the operation was relatively simple compared with laparoscopy and NOTES. The duration of the operation was as short as 20–30 minutes. The rate of abdominal infection among patients treated with the transumbilical approach is lower than among those treated with NOTES because the endoscope does not need to pass through the nonsterile cavity of the stomach or colon. Therefore the rate of infection is equivalent to that associated with a laparoscopic operation. However, the endoscope must be sterilized, and the biopsy hole of the endoscope should be rinsed carefully with ultramicrosoft acidification water and then sterilized by low-temperature hydrogen peroxide plasma, which is the sterilization method used in laparoscopy.
Transumbilical endoscopic exploration and biopsy are of tremendous value in the clinic. The endoscope can bend with more flexibility and rotate at 360° to explore all the organs in the pelvic cavity, the anterior abdominal wall, 75% of the diaphragmatic surface, and two-thirds of the surface of the liver, as well as the gallbladder, appendix, intestinal serosa, part of the duodenal serosa, the anterior wall of the stomach, and the omentum majus. Even a millet-like node of 1–2 mm in diameter can be found with the endoscope, while it is difficult for ultrasonography, computed tomography, and magnetic resonance imaging to diagnose the metastatic diseases of the peritoneum and the surface of the viscus, intra-abdominal adhesions, and inflammation. Therefore, the endoscope facilitates diagnosis and prognosis. Tissue to be identified as malignant or benign can be gripped by the biopsy forceps and manipulated under the endoscope.
This article introduced a novel approach for peritoneal cavity exploration in patients with ascites of unknown etiology, which has proven to be easy, practical, and effective.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grants 30972907 and 81070373).
Disclosure Statement
No competing financial interests exist.