
Abstract
Abstract
Objective:
This study assessed the safety and efficacy of laparoscopic repair of vesicovaginal fistula (VVF) by literature review and pooling analysis, and this is the first report of the experience of using this approach in a patient with a history of radiotherapy.
Subjects and Methods:
Five patients with VVF, including one with a history of cervical cancer and radiation, underwent laparoscopic repair from August 2010 to December 2011 performed by the same experienced surgeon.
Results:
The surgical procedure was uneventful in all of the patients, and no conversion to open surgery was required. Mean operation time was 134 minutes (range, 100–185 minutes). Mean blood loss was 300 mL (range, 250–370 mL), and no one required blood transfusion. Mean hospital stay was 4 days (range, 3–6 days). Laparoscopic repair was successful in 4 patients at the mean follow-up period of 8 months (range, 2–15 months), even in the patient with a history of radiotherapy. VVF recurred in 1 subject, who underwent repeat laparoscopic repair, and 2-month follow-up revealed no fistula.
Conclusions:
Laparoscopic surgery may be a good alternative to the open approach to manage even complicated VVF if it is performed by skilled surgeons.
Introduction
Different surgical approaches have been introduced for management of VVF, including endoscopic treatment, a vaginal or abdominal approach, and combined technique. 3 Laparotomy and extensive dissection in the inflamed tissues from previous surgery may increase peri- and postoperative morbidity rates and prolong the convalescence period. It is also disappointing for women who had undergone the gynecologic surgery to experience repeat operation, especially via the open abdominal approach for management of the fistula.
Laparoscopy as a minimally invasive intervention can be a suitable alternative for those patients who have been selected for abdominal surgery to manage VVF. Here, we present our experience in performing laparoscopic repair of VVF in 5 patients. Likewise, the usage of this approach in a patient with a history of radiotherapy and also in another patient with a history of failed laparoscopic VVF repair is presented for the first time. Furthermore, literature review and pooling analysis of some previous reports were performed using the key words “laparoscopy,” “vesicovaginal fistula,” “uterovaginal fistula,” and “robotic repair” in PubMed.
Subjects and Methods
Five patients with VVF underwent laparoscopy from August 2010 to December 2011 performed by the same experienced surgeon. All of the 5 patients had undergone conservative management, including urethral catheterization and anticholinergic administration, that was not successful. Intravenous pyelography, voiding cystourethrography, and cystoscopy were performed to confirm VVF and exclude other forms of fistula, such as ureterovaginal fistula.
Biopsy of the fistula orifice was performed in a patient with a history of cervical cancer and radiotherapy; final pathology was negative for malignancy. None of the patients had a history of VVF repair, and all of them underwent laparoscopic repair of VVF using the O'Connor technique. Preoperatively, all of the patients were informed about the possibility of open conversion.
Surgical technique
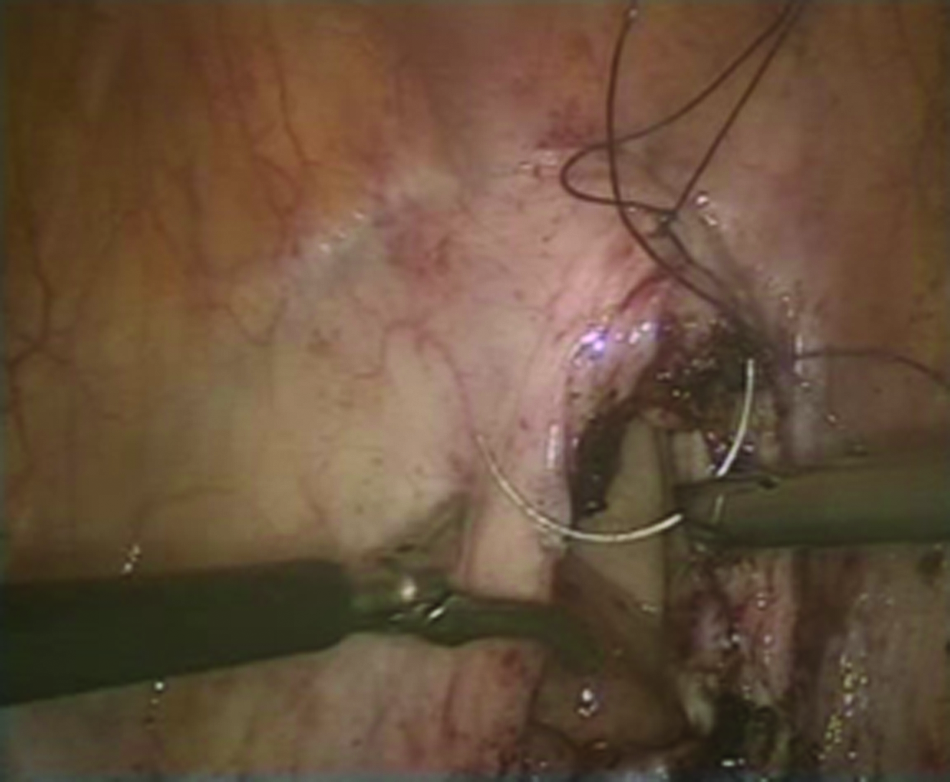
With the patient in the Trendelenburg position under general anesthesia, a 12-mm trocar was fixed in the umbilicus via the open technique, and four 5-mm trocars with a fan-shape structure were inserted after the pneumoperitoneum was created. The bladder was filled by 200 mL of normal saline (0.5% NaCl), and then the vesicovaginal space was entered using an incision of the peritonea on the bladder dome. The bladder was bivalved from the dome to the fistula orifice by scissors. The fistula tract was excised, and then the vagina and bladder were dissected (Figs. 1 and 2). The vagina and bladder were repaired by 2-0 Vicryl™ suture (Ethicon) using a running pattern in one layer (Figs. 3 and 4). To prevent gas leakage from the vagina, a Foley catheter was inserted in the vagina, and its balloon was inflated. The omental flap was mobilized and then fixed by 3-0 Vicryl sutures between the bladder and vagina in 4 patients; there was no proper omentum available to place between the bladder and vagina in a patient with a history of radiotherapy. At the end of the procedure (Fig. 5), an 18 French urethral catheter was fixed. Suprapubic cystostomy was not performed.
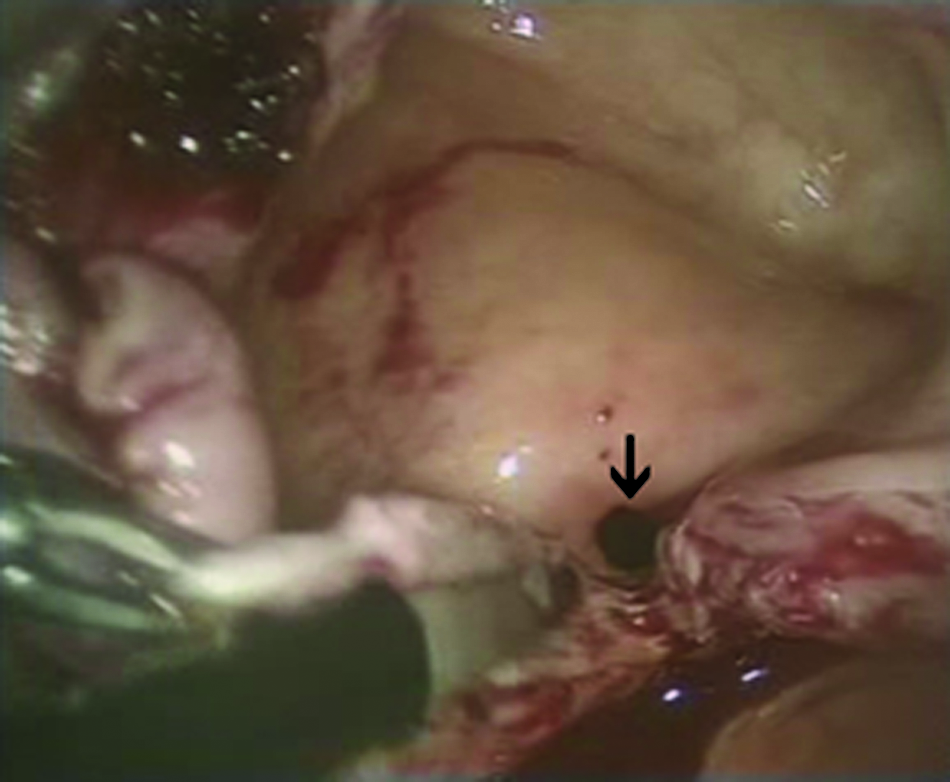
The bladder was bivalved near to the orifice (indicated by the black arrow) of the fistula.
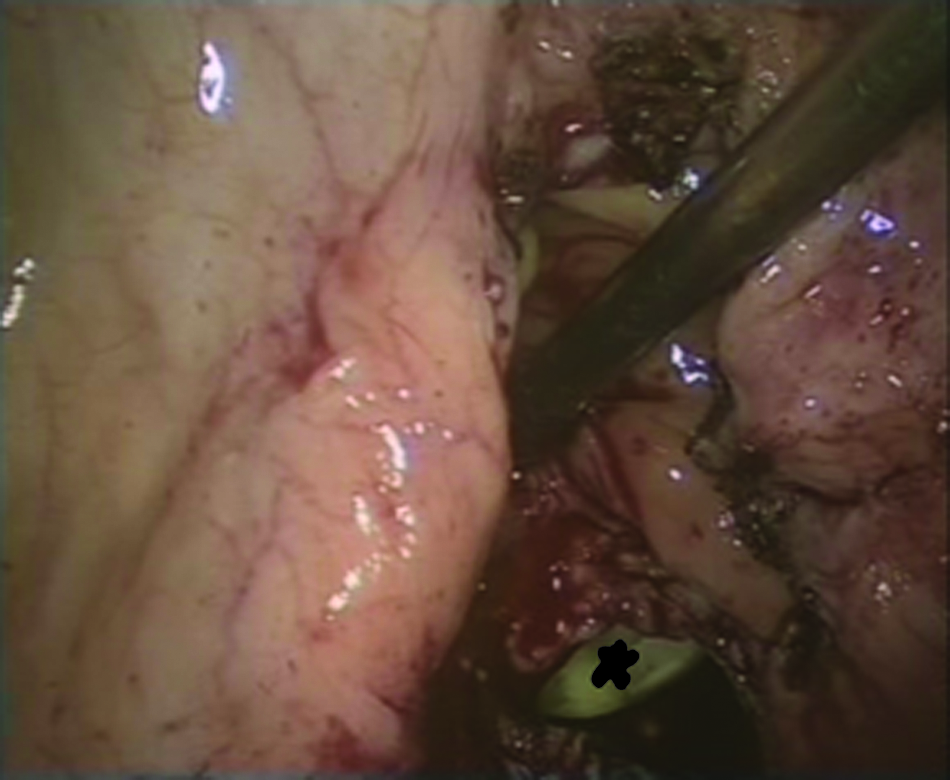
The vagina was opened after excision of the fistula tract. The balloon of the Foley catheter (marked by black asterisk) is seen in the vagina lumen.

Laparoscopic repair of the anterior vaginal wall using running 2-0 Vicryl sutures. Black asterisk reveals the vagina lumen.
Laparoscopic repair of the bladder walls using running 2-0 Vicryl sutures.
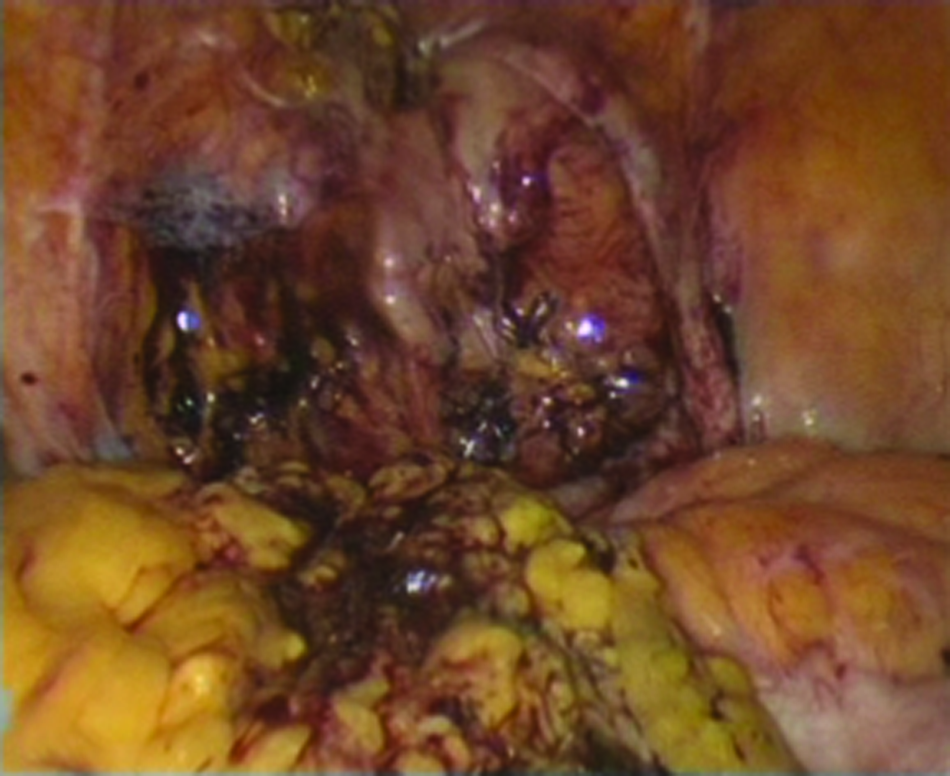
Anterior view of the bladder at the end of the laparoscopic repair.
Results
The surgical procedure was uneventful in all of the patients, and conversion to open surgery did not happen. Mean operation time was 134 minutes (range, 100–185 minutes). Mean blood loss was 300 mL (range, 250–370 mL), and no one required blood transfusion in the peri- and postoperative periods. Mean hospital stay was 4 days (range, 3–6 days). Patients' characteristics are summarized in Table 1.
The urethral catheter was withdrawn 2 weeks after confirmation of the absence of leakage in cystographic slides. Recurrence of incontinence occurred in 1 patient at the mean follow-up period of 8 months (range, 2–15 months); repair was successful in the other 4 subjects, even in the patient with a history of radiotherapy. Etiology of the recurrence in the aforementioned patient was a pinpoint fistula orifice missed in the first laparoscopic repair. This patient underwent repeat laparoscopic management of VVF using the O'Connor technique; at 2-month follow-up, there was no recurrence, and the patient was dry.
Discussion
VVF is an uncommon complication of gynecologic surgery, especially hysterectomy, with a prevalence of 0.1%–0.2%). 4 Selection of the surgical approach depends on the cause of the fistula, its size, location of the orifice, and expertise of the surgeon.
Nezhat et al. 5 in 1994 reported the first laparoscopic repair of VVF, and since then (and including the first account), 28 different reports, including the experience of laparoscopic repair of fistula in a total number of 125 patients, have been published.1–28 From these reports, 5 patients had vesicouterine fistula,6,7,9,10 and another 8 subjects had undergone robotic repair of VVF.4,11,12,28 Therefore, we analyzed a total of 130 patients, including those who underwent laparoscopic repair in previous studies as well as our 5 patients.
Tricks of the trade of laparoscopic repair of VVF
Laparoscopy can be a good alternative in patients who are candidates for the open abdominal approach. This modality has been concomitant with less pain, better cosmetic appearance, shorter hospital stay, and more rapid convalescence. Noticeable magnification of laparoscopy creates better exposure of soft tissues in the pelvic region, which helps the surgeon dissect the tissues around the fistula tract more precisely.13,14 This operation is ergonomic, and sawing is more comfortable compared with laparoscopic pyeloplasty. It is also more feasible than radical prostatectomy because the operation field is not in the deep pelvic area. Recently, using robotic device has been concomitant with good results in 8 patients with VVF.4,11,12
Of the 130 patients with fistula studied, 19 (14.6%) had a history of cesarean section and obstructed labor. Others (84.7%) had a fistula secondary to a gynecologic surgery, such as abdominal or vaginal hysterectomy. Only 1 subject suffered from fistula due to ureterolithotomy. Although there are few reports on patients with hysterectomy because of malignancy, 18 our experience is the first report of laparoscopic repair of VVF in a patient with a history of radiotherapy following hysterectomy performed for the cervical carcinoma.
Fistulas repaired by laparoscopic surgery were between 3 mm17 and 40 mm28 in size. Mahapatra and Bhattacharyya 7 believed that laparoscopy is not an appropriate modality for management of a large fistula or a fistula with a history of treatment failure, whereas Porpiglia et al. 22 revealed the efficacy of laparoscopy in treatment of 4 cases of fistulas with a mean size of >18 mm. Some reports confirmed the importance of laparoscopy in large VVFs as well as fistulas with a history of treatment failure.6,7,14,19 Of 18 patients with a history of failed abdominal or vaginal repair,1,3,6,8,15,16,18–21 3 had undergone two sessions of failed operation, and finally laparoscopic repair has been concomitant with successful outcome. We found no report of laparoscopic management of VVF in a patient with a history of previous failed laparoscopic repair, and our third case seems to be the first report.
Twenty-seven (21%) patients had undergone repair of the fistula using no cystotomy incision (bivalve of the bladder); hence, the bladder was only incised at the fistula tract. This technique requires catheterization of the fistula tract preoperatively. The main advantage of this approach is avoidance of the bladder opening and less postoperative urinary symptoms. The possible drawbacks of the aforementioned surgery are less exposure of fistula and the need to catheterize the tract.
Fistula repair was performed in 73 (56%) patients using vertical cystotomy. This approach is concomitant with better exposure and more precise dissection. Thirty (23%) patients had undergone the operation using combination of the techniques mentioned previously (limited cystotomy: dissection between the bladder and vagina and small longitudinal cystotomy near the tract of fistula).
No flap was interposed between the bladder and vagina in a study by Lee et al. 23 on 5 patients, and no failure was reported. There is general agreement to interpose the flap, especially the omentum, between two adjacent organs. Laparoscopic repair failed in 2 subjects in two different studies13,14 because there was no proper material to place in the very inflamed operation field. We repaired laparoscopically the VVF due to malignancy and radiotherapy successfully without using the omental flap. Different materials have been used as a flap for interposition between two organs, including the omentum, pericolic fat, and peritoneal flap. Fibrin glue and TachoSil® (Takeda Pharmaceuticals) were interposed as a flap with good results in 2 subjects in two separate studies.4,16
Some reports revealed that the bladder and vagina had been repaired by running or interrupted sutures in one or two layers. In two studies with a total of 13 patients, the bladder was reconstructed in one layer, and repair of the vagina was not performed; only the omental flap was interposed between the bladder and vagina.7,24 Failure of treatment was reported in 1 out of 13 patients (success rate, 92.3%).
The operation time varied from 70 minutes 24 to 390 minutes 1 in different studies. Otsuka et al. 18 reported their experience of laparoscopic repair of VVF with the mean operation time of 280 minutes in 8 patients; compartment syndrome occurred in one of their patients in the lower extremities because of prolonged operation time.
Hospital stay slightly depends on the financial and insurance policies in different countries. A few studies reported that patients were discharged with a urethral catheter and drain on the first postoperative day,17,20 whereas other centers kept their patients in the hospital while the urethral catheter and drain were kept in place (2 weeks). 15
Of the 130 patients in the literature review, conversion to open surgery was reported in 6 (4.6%) subjects2,6,14,18 because of severe inflammation and adhesion in two, 2 difficulty in suturing in two, 6 requirement of bladder augmentation in one, 14 and prolonged operative time in one patient. 18
Of 124 patients who underwent complete laparoscopic surgery for managing VVF, 8 (6.5%) had a recurrence of the fistula in the follow-up period, and the overall success rate in the pooling analysis was 93.5%. Laparoscopic repair in 2 of the 8 aforementioned patients had been performed without interposition of a flap.3,14 This success rate is nearly similar to the outcomes of classic open approach (94%–100%). 13
The maximum reported perioperative blood loss has been 333 mL. 13 Some previous studies reported blood loss of less than 200 mL.21,23 Noticeable magnifications may improve homeostasis and decrease blood transfusion.
Major complications in different reports were compartment syndrome in lower extremities, 18 enterocutaneous fistula, 3 and inferior epigastric artery injury 3 in 3 patients. These complications were resolved using fasciotomy, conservative treatment, and laparoscopic repair of the injured artery, respectively. Therefore, the laparoscopic approach can be a safe procedure with a major complications rate of 2.3%.
Conclusions
Laparoscopy with noticeable magnification in the pelvic region helps the surgeon perform better dissection in the inflamed tissues and may be a suitable alternative to the open abdominal approach in patients with VVF. Our experience and review of other reports revealed that this modality is concomitant with a high success rate, even in the early period of fistula formation, large and complicated fistula secondary to radiation, and recurrence after open or laparoscopic repair with a negligible complication rate. We recommend that this surgical approach be performed by highly skilled surgeons in equipped centers.
Footnotes
Disclosure Statement
No competing financial interests exist.