
Abstract
Abstract
Background:
Only a few studies have addressed long-term results comparing laparoscopic and open splenectomy in idiopathic thrombocytopenic purpura (ITP). We analyzed the 1-year results comparing age, sex, length of preoperative steroid therapy, diagnosis-to-splenectomy interval, and preoperative platelet count in relation to postoperative response after open and laparoscopic splenectomy.
Subjects and Methods:
Data collected from two groups, treated by laparoscopic and open splenectomy, respectively, of 20 patients each were retrospectively reviewed. Positive response to splenectomies, evaluated according to the International Working Group guidelines reported by the American Society of Hematology, was statistically related through Student's t test and the Pearson correlation test to the above-mentioned factors.
Results:
Positive response to splenectomy was observed in 80% and 85% of patients, respectively, in the laparoscopic and open groups (P>.10). No statistical differences were observed comparing each of the studied factors between laparoscopic and open splenectomy responder patients (P>.10). When percentage increase of postoperative platelet count was related to diagnosis-to-splenectomy interval, a positive correlation was found in the laparoscopic group (r=0.544, P<.05). In addition, a significant negative correlation in both groups was observed comparing preoperative platelet count and percentage postoperative platelet increase, with a greater increase of postoperative platelet count in patients with a lower preoperative platelet count (laparoscopic group, r=−0.663; open group, r=−0.656; P<.01).
Conclusions:
In this series long-term results after laparoscopic splenectomy in ITP patients were as effective as after the open approach. Higher postoperative platelet percentage increase was achieved in both groups in patients with a lower preoperative platelet count. Finally, laparoscopic splenectomy in this study seems to be superior to the open approach in patients with a longer diagnosis-to-splenectomy interval.
Introduction
With the advent of mini-invasive surgery, laparoscopic splenectomy has become the technique of choice for surgical removal of the spleen in several centers.1,6–9 It has been widely used, especially in ITP disease, which represents in most reported series the main indication for the laparoscopic approach.7–10 Although the laparoscopic removal of the spleen has shown some specific advantages10–13 and the laparoscopic approach might better preserve postoperative systemic immune function than open surgery,12–14 only few studies have compared long-term results of laparoscopic and open splenectomy in ITP patients.
In this study we retrospectively evaluated results of splenectomy, comparing two homogeneous groups of patients with ITP treated with the laparoscopic and the open approaches, respectively, for removal of the spleen.
Subjects and Methods
From 106 patients who underwent splenectomy for ITP from 1982 to 2009 at our institution, we retrospectively collected data concerning the following parameters: age, sex, length of preoperative steroid therapy, diagnosis-to-splenectomy interval, preoperative platelet count, and postoperative platelet count at 1 year after splenectomy. In only 20 cases treated by laparoscopic splenectomy and in another 20 cases operated on with open surgery were all of the above-mentioned data available. We performed a retrospective matched cohort study in these two subgroups of 20 patients each. Data assessed for each patient in the two groups are reported in Tables 1 and Table 2, respectively.
F, female; M, male.
F, female; M, male.
In the two groups, age, sex, length of preoperative steroid therapy, diagnosis-to-splenectomy interval, and preoperative platelet count were statistically comparable (P>.10). Mean age of the patients was 30.0 years (range, 17–50 years) in the open splenectomy group and 29.7 years (range, 19–50 years) in the laparoscopic splenectomy group. Male to female ratio was 0.81 (9 men and 11 women) in the open group and 0.81 (9 men and 11 women) in the laparoscopic group.
At the time of diagnosis, platelet count ranged from 9 to 90×109/L in the open group (mean value, 39×109/L) and from 8 to 80×109/L in the laparoscopic group (mean value, 28.8×109/L). Alternative etiologies of thrombocytopenia were accurately ruled out before treatment.
All patients were previously treated with corticosteroid therapy (prednisone, 1–2 mg/kg/day), and the length of presurgical medical treatment ranged from 2 weeks to 36 months (mean value, 9.9 months) in the open group and from 2 weeks to 30 months (mean value, 9.4 months) in the laparoscopic group.
In the open splenectomy group, 12 patients (60%) did not respond to steroids, whereas in 8 cases (40%) corticosteroid therapy was associated with temporary remission and relapse of the disease with the interruption of medical treatment. In the laparoscopic splenectomy group, 12 patients (60%) were unresponsive to preoperative steroid therapy, and the remaining 8 patients (40%) were responsive but relapsed at the withdrawal of therapy.
All the patients, in both the laparoscopic group and the open group, were symptomatic with various degrees of mucocutaneous bleeding and menorrhagia in the women, when surgery was proposed.
Time interval between diagnosis and splenectomy ranged from 4 to 60 months (mean value, 20.0 months) in the open group and from 4 to 40 months in the laparoscopic group (mean value, 18.4 months).
Open splenectomy was performed in the traditional fashion. Through a midline abdominal incision, the gastrosplenic ligament and short gastric vessels were accurately identified and divided. Splenocolic and splenodiaphragmatic ligaments were then dissected. Finally, the splenic artery and vein were ligated and divided.
Laparoscopic splenectomy was performed in a standardized technique through a Hasson-type trocar inserted in the left subhepatic region, two 5-mm trocars in the subxiphoid and in the subcostal anterior axillary line, and a 12-mm trocar lateral to the Hasson-type trocar. 15 With the patient in the semilateral position, the gastrosplenic, the splenocolic, and the splenodiaphragmatic ligaments were dissected, and the splenic hilum vessels were secured using an endovascular stapler. Both in the open group and in the laparoscopic splenectomy group, the splenic hilum, the tail of the pancreas, splenocolic and gastrosplenic ligaments, omentum, and paraduodenal area were always checked for accessory spleens.
Results of surgery were evaluated at 1 year after splenectomy through assessment of blood platelet count and remission of symptoms.
Based on the recommendations of the International Working Group reported by the American Society of Hematology, 16 in this study a positive response was considered to have occurred when the postoperative platelet count was ≥100×109/L and bleeding was absent (complete response) or in patients with a postoperative platelet count ≥30×109/L and a twofold increase in platelet count from baseline and absence of bleeding (response).
Response to splenectomy was related for each group to age and sex of patients, length of preoperative corticosteroid therapy, preoperative platelet count, and time interval between diagnosis and surgery.
Statistical analysis was performed using Student's t test and Pearson's correlation test.
Results
Accessory spleens, removed surgically, were found in 3 patients (15%) in the laparoscopic group and in 3 patients (15%) in the open group.
At 1 year after surgery in the laparoscopic group a complete response was observed in 15 of 20 (75%) and a response in 1 of 20 (5%), for an overall positive response rate of 80% (16/20). In the open group a complete response was observed in 16 of 20 (80%) and a response in 1 of 20 (5%), for an overall response rate of 85% (17/20). The rate of responders in the two groups was not statistically different (P>.10).
No statistically significant differences were also observed comparing each factor, including age, sex, length of preoperative steroid therapy, and diagnosis-to-splenectomy interval, between laparoscopic and open splenectomy responder patients (P>.10).
When only the parameter of percentage increase of postoperative platelet count was considered, correlation between age, sex, length of preoperative steroid therapy, and rate of increase of postoperative platelet count was statistically not significant in both open and laparoscopic groups (P>.05 with a Pearson's correlation coefficient r<0.444) (Table 3).
The critical value of the Pearson correlation coefficient r in a two-tailed test with 18 degrees of freedom and .05 level of statistical significance is 0.444; with .01 level of significance, r is 0.561.
In contrast, correlation between diagnosis-to-splenectomy interval (in months) and postoperative platelet percentage increase showed a statistical difference between the laparoscopic and open groups. In the laparoscopic group (Fig. 1a), unlike in the open group (Fig. 1b), a positive statistical correlation was found (laparoscopic group, r=0.544, P<.05; open group, r=0.137, P>.05).
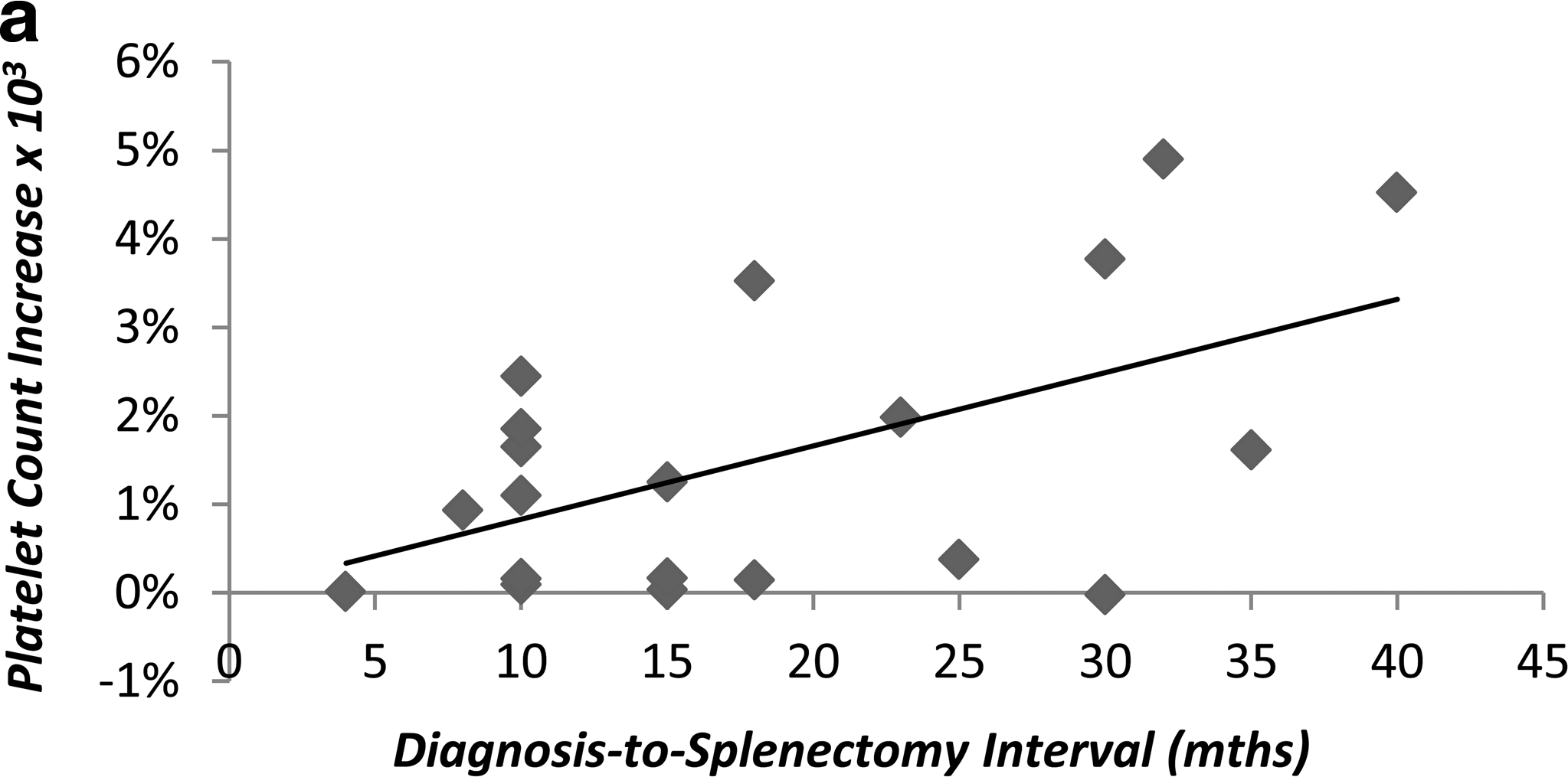
Correlation between post-splenectomy platelet count increase (percentage of preoperative value) and length of diagnosis-to-splenectomy interval (months). Scatter plots and linear trend lines are shown for the
Comparison between preoperative platelet count and postoperative platelet count increase at 1 year after surgery showed, both in the open group and in the laparoscopic group, a significant negative correlation (laparoscopic group, r=–0.663, P<.01; open group, r=–0.656, P<.01) with a higher increase of postoperative percentage platelet count in patients with a lower preoperative platelet count (Fig. 2).
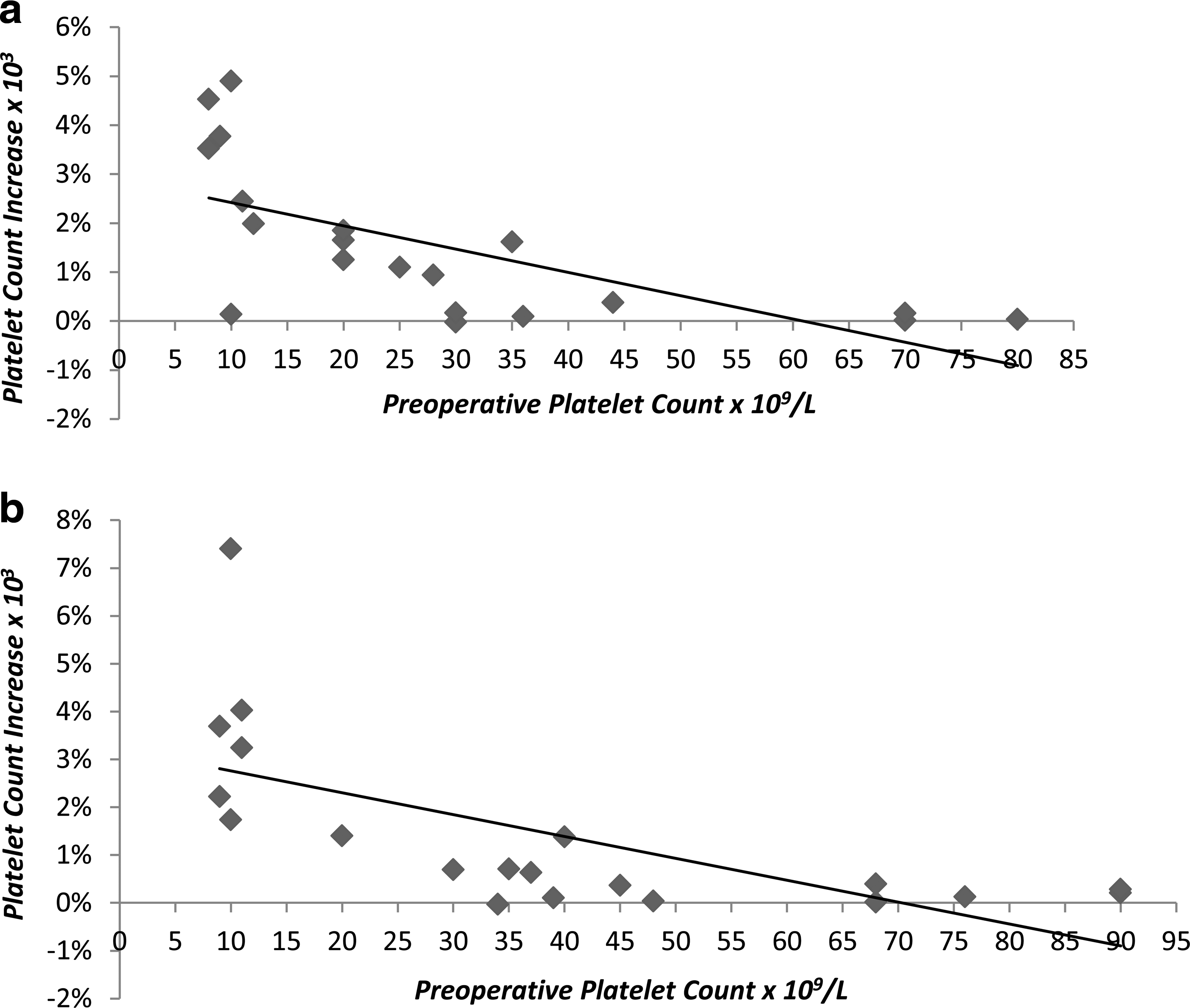
Correlation between post-splenectomy platelet count increase (percentage of preoperative value) and preoperative platelet count. Scatter plots and linear trend lines are shown for
Discussion
ITP is an autoimmune disease characterized by the destruction of opsonized platelets in the reticuloendothelial system,4,17 particularly in the spleen, and/or suppression of platelet production, 17 resulting in a persistent low platelet count.4,18
Steroid therapy and splenectomy are the most effective forms of treatment in the management of this disease.1–4,11 Steroid therapy shows a cure rate ranging from 64% to 88%.3,4,6,8,18–24 In about 12%–36% of patients, however, relapse of the disease is observed,2,4,8,19 and in about 12% of cases only a partial response has been observed.2,4
Splenectomy is the standard second-line treatment for chronic ITP3,4 and is the treatment of choice in the majority of patients affected by ITP refractory to corticosteroid therapy,1–4 when steroids are contraindicated, or in patients with a low compliance for medical treatment. 5 Its efficacy is probably related to the fact that splenectomy removes both the principal site of autoimmune cell production and also the major site of platelet destruction,2,20 improving the platelet survival time. 25
Splenectomy has a high success rate. As reported in the literature a complete response after splenectomy has been observed in 66%–100% of cases.2–4,6,18–22,24 About 80% of patients with ITP respond rapidly, often within 1 week.3,4,6,18–22,26,27 Splenectomy, however, may be followed by a high initial relapse rate, which anyway may decline over time.1–3 In fact, in several studies a 15% relapse rate has been observed within the first year,2,4,8,24,26 but afterward the remission rate remains almost stable, with two-thirds of patients remaining asymptomatic 10 years after surgery.3,6
Only a few literature reports so far have addressed results after laparoscopic splenectomy in ITP patients. In these studies long-term results showed remission rates ranging from 67.9% to 72% 5 years after surgery.8,12,13,23,27–33
Data are still controversial when the laparoscopic approach has been compared with the open approach.11,12,28,29,34,35 Shimomatsuya and Horiuchi 28 compared operating time, blood loss, length of hospital stay, and platelet count response and observed a shorter operating time and a longer hospital stay in the open splenectomy group. Blood loss was less for open splenectomy than for laparoscopic splenectomy, and no significant difference was noted in the postoperative platelet count. Lozano-Salazar et al. 29 compared 26 patients and 22 patients who underwent, respectively, open and laparoscopic splenectomy. Operative time was longer in the laparoscopic group, and response rates were similar in both groups. Watson et al. 12 reported 47 patients and 13 patients with ITP operated on with open splenectomy and the laparoscopic technique, respectively. Blood and platelet transfusion requirements in this study were reduced by the laparoscopic approach. Long-term normalization of platelet counts was similar in the two techniques.
Schlinkert and Mann 34 compared 14 open procedures and 7 laparoscopic splenectomies in ITP patients and showed a shorter hospital stay, a lesser parenteral narcotic requirement, and a longer operative time in the laparoscopic group. Long-term results were not mentioned in this study. Delaitre and Pitre, 35 comparing two groups of 28 patients each, reported a recurrence of ITP in 2 patients of the laparoscopic group and in 4 patients of the open group. Vecchio et al. 11 compared a laparoscopic group and a open group of patients affected by ITP and observed a lesser amount of operative bleeding in the laparoscopic group (P<.01) than in the open group. Need for platelet transfusion was less in the laparoscopic group, with only 30% of patients transfused in the laparoscopic group compared with 100% of the open group. The number of units of platelets transfused for each patient was also higher in the open group than in the laparoscopic group.
In our study long-term results were similar in both the open and the laparoscopic splenectomy groups. Based on the recommendations of the International Working Group reported by the American Society of Hematology, we considered a positive response to splenectomy had occurred when the postoperative platelet count was ≥100×109/L in the absence of bleeding (complete response) or when the postoperative platelet count was ≥30×109/L with a greater than a twofold increase in platelet count from baseline in the absence of bleeding (response). Using these criteria a positive response was observed at 1 year after surgery in 80% of patients in the laparoscopic group and in 85% of patients in the open splenectomy group. No statistical difference, according to Pearson's correlation test, was observed in both the open and the laparoscopic groups when the rate of increase of the postoperative platelet count was related to age, sex, and length of preoperative therapy.
In the literature the response to splenectomy has been related positively with some factors like patients' age less than 40 years4,8,19,33 or the length of the disease before surgery. 1 In this study we failed to confirm these results.
Results after splenectomy have been also related to the preoperative platelet count. According to some authors, 8 patients with high preoperative platelet counts successfully respond to open splenectomy. Very few results are reported after laparoscopic splenectomy. Duperier et al. 8 suggested that a better response rate to splenectomy can be found in the group of patients with a preoperative platelet count of less than 30×109/L. In our series, we did not find in either laparoscopic or open responder patients a statistically significant difference when preoperative platelet counts were compared. When the single parameter of postoperative platelet count percentage increase was considered, however, a negative correlation between preoperative platelet count and postoperative platelet percentage increase was observed, suggesting that a greater increase of platelet count after both laparoscopic and open surgery should be expected in patients with a lower preoperative platelet count. Therefore, it appears that there could be a correlation between the entity of preoperative thrombocytopenia and splenectomy response, suggesting a low threshold of preoperative platelet count as an important factor to propose as an indication for surgical spleen removal in ITP patients.
A short diagnosis-to-surgery interval has also been hypothesized as a factor influencing a good response to splenectomy. So far, some studies2,4 have reported no evidence to assess the relationship between diagnosis-to-surgery interval and positive response to splenectomy. In our study the laparoscopic group showed a statistically significant positive correlation when diagnosis-to-splenectomy interval was related to postoperative percentage increase of platelet count. This result was not confirmed in our open group. If this finding is confirmed in other studies, it should be, however, relevant in clinical practice, suggesting that the longer the diagnosis-to-splenectomy interval, the better the response to the laparoscopic removal of the spleen. Immunologic studies in ITP patients throughout the natural course of the disease and immunological changes after laparoscopic compared with open splenectomies are probably needed to better address the observation of this study.
Footnotes
Disclosure Statement
No competing financial interests exist.