
Abstract
Abstract
Objective:
To retrospectively review our experience with respect to evaluating the feasibility and safety of laparoendoscopic single-site (LESS) dismembered pyeloplasty for ureteropelvic junction obstruction (UPJO) through a retroperitoneal approach.
Patients and Methods:
Between March 2011 and January 2012, 10 consecutive patients underwent LESS retroperitoneoscopic dismembered pyeloplasty performed by one experienced laparoscopic surgeon at our institution. A single-port access was inserted through a 2.5-cm transverse skin incision below the 12th rib along the midaxillary line. Standard steps of the multisite retroperitoneoscopic Anderson–Hynes dismembered pyeloplasty technique using conventional instruments or a combination of conventional and bent laparoscopic instruments were performed. Follow-up studies were conducted by intravenous urography (IVU), diuretic renal scan, and renal ultrasonography.
Results:
LESS retroperitoneoscopic dismembered pyeloplasty was successful in 9 patients, whereas 1 required four-port retroperitoneoscopic conversion because of difficulties in remaining in the retroperitoneal space due to a peritoneal tear during the procedure. The mean operative time was 148.4 minutes (range, 103–210 minutes). The mean estimated blood loss was 31 mL (range, 10–70 mL), and the mean postoperative hospital stay was 5.7 days (range, 3–13 days). Intraoperative complications were limited to the one case of peritoneal tear. An aberrant crossing vessel was noted in 4 patients, and transposition was not required in these patients. Urine leakage occurred in 1 patient postoperatively and was successfully treated by conservative management. The mean follow-up period was 6.2 months (range, 5–10 months). Satisfactory drainage with decreased hydronephrosis on IVU, diuretic renal scan, and renal ultrasonography was observed in all cases at the 3-month imaging studies.
Conclusions:
In experienced hands, LESS retroperitoneoscopic dismembered pyeloplasty is a feasible and safe alternative for correcting UPJO, although it remains technically challenging. The long-term outcome awaits further studies.
Introduction
To our knowledge, because of a small working space and difficulty in anatomic orientation by retroperitoneal approach, the transperitoneal approach, often concealed at the umbilicus, is typically used for LESS pyeloplasty.2–7 Little information is available about experience with LESS pyeloplasty via a retroperitoneal approach. However, the retroperitoneal approach has some obvious advantages, including a short and direct access to the target lesion and a potential reduction in invasiveness. In this study, we retrospectively review our experience with respect to evaluating the feasibility and safety of retroperitoneal LESS dismembered pyeloplasty.
Patients and Methods
Patients
Between March 2011 and January 2012, retroperitoneal LESS dismembered pyeloplasty was performed in 10 consecutive patients by one experienced laparoscopic surgeon (X.C.)8–10 at our institution. This study obtained informed consent from the patients and ethics approval from the ethics committee at Xiangya Hospital, Central South University, Changsha, Hunan Province, China. Also, we obtained informed consent from the adult participants or from the parents of the child participants in our study. The informed consent was written and specified in the operative consent. The patients included 6 men and 4 women, with an average age of 23.8 years (range, 9–42 years), and their average body mass index was 26.1 kg/m2 (range, 21.7–29.8 kg/m2). Of the 10 patients, 9 had UPJO on the left side and 1 on the right side. Nine presented with mild to moderate flank pain, and 1 was asymptomatic and discovered incidentally by renal ultrasonography for a health examination. No patients had undergone renal surgery previously. The diagnosis was established by renal ultrasonography, intravenous urography (IVU) with high-volume contrast medium, magnetic resonance urography, and/or retrograde pyelography.
Operative technique
The patients were subjected to general endotracheal anesthesia and placed on a maximally flexed table to extend the ipsilateral flank in the full lateral decubitus position. A 2.5-cm transverse skin incision, with finger-and balloon-dissecting and a retroperitoneoscopic approach, was used as described in a previous series. 10 A single-port access was inserted through the lumbar incision. The pneumoretroperitoneum was established by carbon dioxide insufflation at 12–14 mm Hg. The procedure was performed through the single-port access using conventional instruments or a combination of conventional and bent laparoscopic instruments. (Fig. 1). The retroperitoneal fat and adjacent tissues outside of Gerota's fascia were routinely dissected and removed. Gerota's fascia was opened longitudinally, the lower pole of the kidney, the dilated renal pelvis, and the upper ureter were then mobilized, and the status of UPJO was assessed (Fig. 2A). If a crossing vessel was encountered and was a vein or a small artery concomitant with intrinsic stenosis of UPJ, the vessel was just dissected free. If the crossing vessel was a large arterial branch and it was expected that the vessel could press on the ureteropelvic anastomosis after surgery, however, the renal pelvis and ureter were transposed anterior to the vessel.

The procedure was performed through the single-port access using conventional instruments or a combination of conventional and bent laparoscopic instruments.
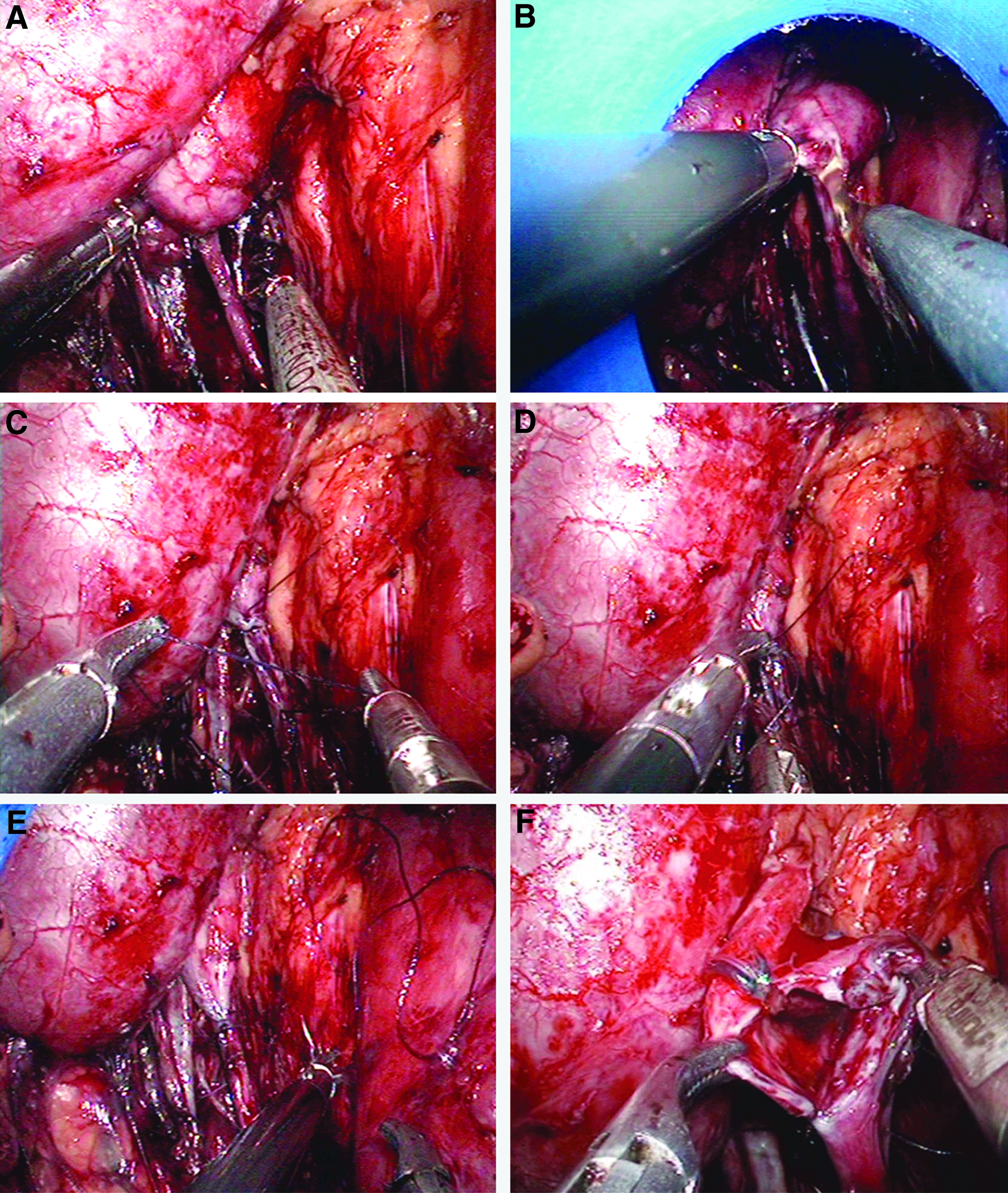
A standard Anderson–Hynes dismembered pyeloplasty was performed. In brief, the renal pelvis was partly divided with scissors from the most dependent part, cephalad toward the renal pelvis, and keeping the most lateral extent of the renal pelvis undismembered for traction (Fig. 2B). Traction was maintained, and the ureter was spatulated, extending inferiorly through the stenosis of the UPJ for about 2 cm. The most dependent part of the pyelotomy was sutured to the apex of the spatulated ureter using a 4-0 Vicryl® (Ethicon) suture (Fig. 2C–E). The stenotic segment of the UPJ and the redundant renal pelvis were removed. The posterior pelvic–ureteric anastomosis was completed with an interrupted suture, and the remaining pyelotomy was closed with a running suture (Fig. 2F). After one segment of 3 French ureteral catheter with appropriate length as the guide wire was passed into the 6 French double-J stent (4.7 French for children) from the proximal side hole into the stent, the stent was inserted in an antegrade fashion into the bladder (Fig. 2G). After the ureteral catheter was withdrawn, the proximal end of the stent was placed in the renal pelvis. Then the anterior pelvic–ureteric anastomosis was completed with an interrupted suture. Hemostasis was checked carefully after the pressure of the pneumoretroperitoneum was lowered. A closed suction drain was placed through the incision. The Foley catheter was removed 2 or 3 days postoperatively. The retroperitoneal drain was subsequently removed if there was no increase in output and it was less than 10 mL. The stent was removed in 4–6 weeks. IVU, diuretic renal scan, and renal ultrasonography were performed 3 months postoperatively.
Results
LESS retroperitoneoscopic dismembered pyeloplasty was successful in 9 patients, whereas 1 required four-port retroperitoneoscopic conversion because of difficulties in remaining in the retroperitoneal space due to a peritoneal tear during the procedure. The patients' characteristics and surgical demographics are presented in Table 1. The mean operative time was 148.4 minutes (range, 103–210 minutes). The mean estimated blood loss was 31 mL (range, 10–70 mL), and the mean postoperative hospital stay was 5.7 days (range, 3–13 days). Intraoperative complications were limited to the 1 case of peritoneal tear. Intrinsic stenosis of the UPJ concomitant with a vein or a small artery was found in 4 cases, and thus transposition was not required in these patients. Urine leakage occurred in 1 patient postoperatively and was successfully treated by conservative management. The mean follow-up period was 6.2 months (range, 5–10 months). Nine patients who presented with flank pain preoperatively were all symptom free postoperatively. Satisfactory drainage with decreased hydronephrosis on IVU, diuretic renal scan, and renal ultrasonography was observed in all cases at the 3-month imaging studies.
Ranges are given in parentheses.
Four-port retroperitoneoscopic conversion.
Discussion
In the last two decades, laparoscopic surgery has evolved rapidly for a variety of ablative and reconstructive urological procedures and is associated with decreased postoperative pain and shorter convalescence. Nevertheless, efforts are ongoing to further minimize morbidity and visible scarring of laparoscopic surgery, focusing on reducing the total number of necessary skin incisions for trocar positioning. In response, LESS has recently emerged as a potentially less invasive alternative to conventional laparoscopy. We agree with the opinion that LESS seems ideally suited for upper tract reconstructive procedures such as pyeloplasty and benign ablative indications such as simple nephrectomy with strict patient selection. 5 We started the practice of LESS beginning in March 2011, when the first LESS retroperitoneoscopic decortication was performed in a patient with a large and posterior renal cyst. With increasing experience of LESS, we have expanded the indication in urologic surgery, including adrenalectomy, nephrectomy, 10 and pyeloplasty through the retroperitoneal approach. In this study, we report our initial experience with and the short-term outcome of LESS retroperitoneoscopic dismembered pyeloplasty using conventional instruments or a combination of conventional and bent laparoscopic instruments.
There is no doubt that LESS dismembered pyeloplasty is a technically challenging and lengthy surgical procedure, especially through the retroperitoneal approach. Not only is proficiency required for intracorporeal freehand suturing and knotting, but also the internal nature of LESS may be responsible for that. Because surgical instruments were placed in parallel, the major problem performing LESS was lack of triangulation previously associated with the classic three-port technique. Furthermore, the single incision allows only a narrow range of motion for the laparoscopic instruments. 11 These limitations made dissection, intracorporeal freehand suturing, and knotting more technically challenging. Therefore, we used three main strategies in dissection, suturing, and knotting. First, we always kept the camera superiorly and the two working ports at 4 and 8 o'clock intracorporeally, which allowed for ergonomics similar to those of standard laparoscopy. As a result, the surgeon can use both hands to control inline, uncrossed instruments to complete manipulation. Second, in making a knot, we often used two curve graspers instead of the combination of one curve grasper and one needle holder because the grasper has a longer and more curved tip. That could offset the shafts adequately to accomplish a satisfactory degree of triangulation and be helpful for making loops for knot-tying with a minimal excursion range. Third, the distal segment of the suture was routinely folded to form an acute angle (Fig. 2C and D), which could also contribute to making multiple loops.
The placement of the double-J stent is another technical challenge in LESS pyeloplasty. Some surgeons preferred to place the double-J ureteral stent in a retrograde manner using cystoscopy at the beginning of the procedure. 2 However, earlier the double-J stent would hinder trimming of the renal pelvis ureter and suture of the posterior anastomosis. Furthermore, dissection may be more difficult owing to the decompression of the renal pelvis by the stent. In the popular laparoscopic intracorporeal method, antegrade stent insertion can be performed through the assistant trocar over a guide wire 9 or percutaneously by introducing a guide wire via an angiocatheter. 12 We preferred to use an antegrade manner but with a modified technique to suit LESS pyeloplasty. In our procedure, one segment of 3 French ureteral catheter with appropriate length as a guide wire was passed into the 6 French double-J stent from the proximal side hole into the stent. The main advantage of this modified technique has been that the insertion of the stent into the bladder could be completed without the need of additional ports or the change of the patient's position.
In the published literatures, conventional laparoscopic pyeloplasty can be performed through a retroperitoneal or transperitoneal approach with similar results. 13 For LESS pyeloplasty, the transperitoneal approach, often concealed at the umbilicus, has been preferred by most laparoscopic surgeons2–7 because it offered a larger working space for suturing and a subjective improvement in cosmetic outcome. However, the retroperitoneal approach for LESS pyeloplasty offers various obvious advantages. First, it provides a shorter and more direct access from the port site to the kidney than that of the transumbilical approach. Thus it may allow a wider range of motion of laparoscopic instruments, facilitating the suturing and dissection. Second, it does not require mobilization of intraperitoneal organs or retraction of organs, which may reduce the risk of intraperitoneal organ injury and subsequent adhesive intestinal obstruction. In contrast, through the transperitoneal approach, an additional trocar 14 or transparietal stitches 15 were at times needed to retract the intraperitoneal organ for exposition. Third, because the retroperitoneal approach does not violate the peritoneal cavity, it may reduce the risk of potential deleterious effects of peritoneal exposure to blood and urine and peritoneal irritation by insufflated carbon dioxide. 16 Although the retroperitoneal approach may compromise the cosmetic benefit compared with the transumbilical approach, a small port site scar at the back is usually acceptable to the patients.
Although the retroperitoneum initially affords a relatively smaller working space than the peritoneal cavity, which can result in difficulty in orientation and visibility, 17 as the dissection proceeds, the retroperitoneal space can be readily enlarged and developed as necessary. 18 In our experience, it was necessary to dissect and remove the retroperitoneal fat outside of Gerota's fascia and the perirenal fat located at the lower pole to widen the working space. Furthermore, we believe that it is also very important to keep the integrity of the peritoneal envelope for good exposure of the surgical field, especially in LESS procedures. In our series, 1 patient required four-port retroperitoneoscopic conversion owing to difficulties in remaining in the retroperitoneal space because unskillful manipulation caused peritoneal rupture at the early stage.
Our experience about orientation in the retroperitoneum can be summarized as follows. First, the patients were placed at a lateral decubitus position, and the incision was made below the 12th rib along the midaxillary line. Thus, after the laparoscope was introduced into the retroperitoneal cavity, the erector muscle of the spine could be identified posteriorly from the port. This procedure not only facilitated the opening of Gerota's fascia without causing injuries to the peritoneum, but also prevented the port from getting too close to the rib, allowing movement of the instruments. Second, after Gerota's fascia was opened, the psoas major muscle could be used as a landmark for orientation. Generally, the dilated renal pelvis and the upper ureter could be easily identified between the lower pole of the kidney and the psoas major muscle.
Although the present series included only 10 patients, we showed clearly that LESS retroperitoneoscopic dismembered pyeloplasty is technically feasible and can be accomplished reasonably quickly. Our success rate was 90%, and it was equivalent to that reported by Tugcu et al. 2 and Tracy et al. 4 In the present study, the mean operative time was lower than that reported by Tugcu et al. 2 and Tracy et al. 4 (148.4 versus 204.5 and 207 minutes, respectively). The reduction of the mean operative time may be explained by two reasons. First, our extensive experience with many previous traditional retroperitoneoscopic procedures that also required proficient intracorporeal freehand suturing techniques and retroperitoneal LESS ablative surgeries could shorten the learning curve of LESS dismembered pyeloplasty. Second, as previously discussed, the retroperitoneal approach provided rapid and direct access to the urinary tract and avoided mobilization of intraperitoneal organs or retraction of organs, which could also be responsible for that reduction. Although the long-term results of LESS retroperitoneoscopic dismembered pyeloplasty are awaited, the encouraging early results suggest a promising potential for LESS retroperitoneoscopic dismembered pyeloplasty to become a viable alternative to conventional retroperitoneoscopic dismembered pyeloplasty in the future.
Our study had several limitations. This study has a small number of patients, and we did not obtain enough data to use a comparative cohort of patients who underwent conventional retroperitoneoscopic pyeloplasty so that a reasonable comparison can be made. Furthermore, lack of cosmetic and pain assessment does represent another limitation. Therefore, a validated questionnaire and longer follow-up are needed to assess the benefits in cosmesis and convalescence compared with conventional retroperitoneoscopy.
Conclusions
In this study, we demonstrated our initial experience with and the short-term outcome of LESS retroperitoneoscopic dismembered pyeloplasty at our institution. In experienced hands, LESS retroperitoneoscopic dismembered pyeloplasty is a feasible and safe alternative for correcting UPJO, although it remains technically challenging. The long-term outcome awaits further studies.
Footnotes
Disclosure Statement
No competing financial interests exist.