
Abstract
Abstract
Objectives:
To identify the optimal treatment for extrahepatic bile duct stones using endoscopy, laparoscopy, and the combination of the two in different conditions and to develop phasic treatment protocols for their minimally invasive treatment.
Patients and Methods:
Of 2718 cases of extrahepatic bile duct stones collected from June 2005 to December 2011, 50 were randomly selected to receive open bile duct exploration and T-tube drainage, serving as the control group. For the rest, a one-scope protocol, two-scope protocol (two-scope protocol A or two-scope protocol B), or three-scope protocol was adopted according to the specific conditions of stones and the endoscopic treatment results. The treatment outcomes and postoperative clinical indicators of the minimally invasive treatment protocols were analyzed and compared with those of the control group.
Results:
Among the 2668 cases of extrahepatic bile duct stones receiving the phasic minimally invasive treatment, the treatment success rate was 97.79%, and there were no severe postoperative complications. Compared with the control group, the minimally invasive treatment protocols had higher success rates, less trauma, and significantly shortened hospital stays.
Conclusions:
The protocols were applied step by step based on the different types and levels of extrahepatic bile duct stones, fully embodying the advantages of the combined minimally invasive treatment of endoscopy and laparoscopy, thus expanding the scope of minimally invasive surgical treatment for extrahepatic bile duct stones and improving treatment success rate.
Introduction
Patients and Methods
General information
In total, 2718 patients (1161 men, 1557 women) with extrahepatic bile duct stones were treated from June 2005 to December 2011. The patients ranged in age from 18 to 92 years with an average age of 61.74 years. Among them, there were 423 patients with extrahepatic bile duct stones alone and 2295 with extrahepatic bile duct stones complicated with cholecystolithiasis.
First, 50 patients were randomly selected to receive open common bile duct exploration and T-tube drainage, serving as the control group (9 patients with extrahepatic bile duct stones alone, 41 patients with extrahepatic bile duct stones complicated with cholecystolithiasis). The rest received emergency surgery or elective surgery to remove the stones by duodenoscopy after hospitalization, and further treatment protocols were determined based on the treatment outcomes.
Selection of phasic treatment protocols
After successful stone removal via duodenoscopy, patients with extrahepatic bile duct stones alone were cured and discharged from the hospital. This was referred to as the one-scope protocol (therapy by duodenoscopy alone). Patients with extrahepatic bile duct stones complicated with cholecystolithiasis received laparoscopic cholecystectomy (LC), which was referred to as two-scope protocol A (combination therapy of duodenoscopy and laparoscopy). If stone removal via duodenoscopy failed and the endoscopic nasobiliary drainage (ENBD) succeeded, laparoscopic bile duct exploration combined with removal of all bile duct stones with the choledochoscope and other apparatuses was performed. Then, primary suture of the bile duct incision was performed. This was referred to as the three-scope protocol (combined therapy of duodenoscopy, laparoscopy, and choledochoscopy). Finally, if ENBD failed, a laparoscopic bile duct exploration combined with use of the choledochoscope was performed to completely remove the stones; a T-tube was inserted for drainage. This was referred to as two-scope protocol B (combined therapy of laparoscopy and choledochoscopy). Figure 1 shows a flowchart of the phasic treatments.
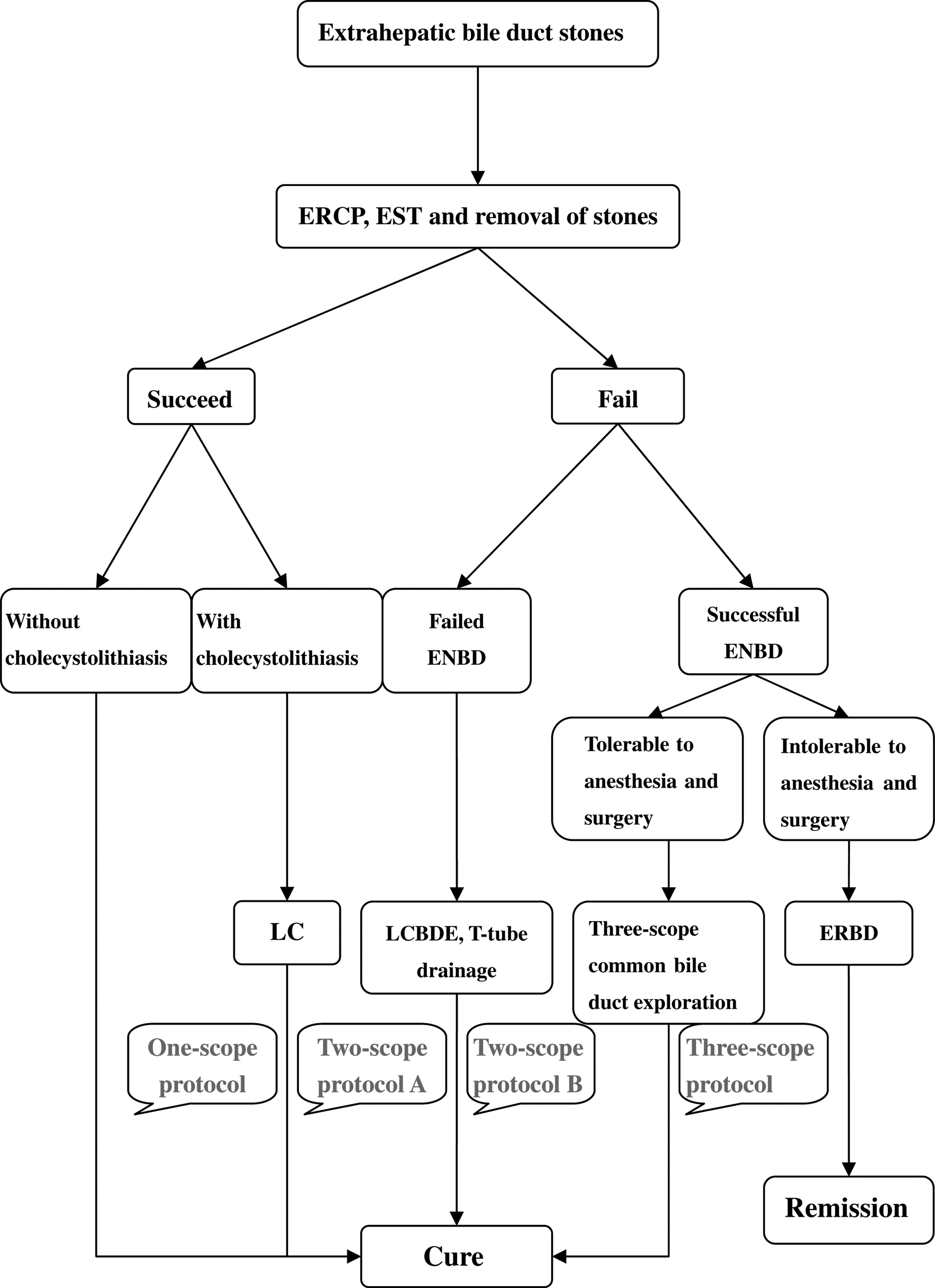
Flowchart of phasic minimally invasive treatment protocols for extrahepatic bile duct stones. ENBD, endoscopic nasobiliary drainage; ERBD, endoscopic retrograde biliary drainage; ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy; LC, laparoscopic cholecystectomy; LCBDE, laparoscopic common bile duct exploration.
Indications and treatment process
One-scope protocol
This protocol was applied to patients with only extrahepatic bile duct stones (primary, secondary, residual, or recurrent stones). In total, 414 patients were treated in this group.
After the extrahepatic bile duct stones were confirmed by endoscopic retrograde cholangiopancreatography (ERCP), endoscopic sphincterotomy (EST) was performed. According to the size, number, and hardness of the stones detected by the ERCP, appropriate methods were adopted to completely remove the stones. Common methods included removal of the stones by balloon catheter or basket or after lithotripsy (basket mechanical lithotripsy, electrohydraulic lithotripsy, and laser lithotripsy).
Two-scope protocol A
Extrahepatic bile duct stones complicated with cholecystolithiasis without biliary stricture were an absolute indication for this protocol. In total, 2254 patients were treated in this group.
The treatment was divided into two phases. First, ERCP and EST were performed via ERCP, and the bile duct stones were completely removed by basket or balloon. It is well known that, in order to be completely cured, patients without obvious surgical contraindications should undergo LC; thus the patients then underwent the LC procedure. 3 The interval between the two phases was 1–3 days, depending on the patient's condition.
Two-scope protocol B
This protocol was applicable to patients with failed choledocholith removal or failed ENBD or to those who had residual intra- and extrahepatic bile duct stones during surgery. In total, 49 patients were treated in this group, including 8 and 39 patients transferred from the one-scope protocol and two-scope protocol A, respectively, because of treatment failure. An additional 2 patients were transferred from the three-scope protocol because of potential residual intrahepatic bile duct stones, which would be removed later through a T-tube sinus tract.
During this procedure the LCBDE was performed, and four methods (direct stone removal by apparatus, stone removal by saline flushing, choledochoscope stone removal, and intraoperative laser lithotripsy) were used to completely remove the stones. A T-tube was inserted for drainage after use of the choledochoscope and was removed 3 weeks later, if no residual stones were detected by T-tube cholangiography 8–10 days after operation.
Three-scope protocol
This protocol was first proposed by our hospital in China and applied to patients with failed stone removal by the endoscopic stone extraction technique but with successful ENBD. In total, 285 patients were treated in this group, including 22 patients transferred from the one-scope protocol and 263 patients from two-scope protocol A, respectively, because of treatment failure.
The treatment process was as follows: (1) Endoscopic treatment phase: After successful ERCP, if endoscopic removal of the bile duct stones was difficult, effective ENBD was performed. (2) Laparoscopic treatment phase: 1–2 days after the condition became stable, LCBDE was performed, and primary suture of the bile duct incision was performed as long as no residual stones were detected by use of the choledochoscope. (3) Postoperative treatment phase: 4–5 days after operation, the ENBD tube could be removed if no abnormality was detected by cholangiography via the ENBD tube.
Palliative minimally invasive treatment protocol
For patients with failed endoscopic stone removal but successful ERCP or those with obvious surgical contraindications, endoscopic retrograde biliary drainage (ERBD) was performed to remove biliary obstruction and relieve symptoms. 4 In total, 21 patients were treated. No recurrent cholangitis was noted after a follow-up of more than 6 months.
Outcome measures
The success rate, complications, operation time, and hospital stay of the minimally invasive treatment group and control group (open surgery) were observed, and a comparative analysis of related indicators was carried out between each protocol.
Statistical methods
SPSS version 13.0 software was used in statistical analysis. The data were assessed by Student's t test, analysis of variance, and the chi square test.
Results
Minimally invasive treatment success rate
The success rate of each of the four minimally invasive treatment options was more than 85%, indicating the feasibility of the phasic protocols (Table 1). According to the statistical results, the total success rate of the minimally invasive treatment of extrahepatic bile duct stones was 97.79% (2609/2668).
Early postoperative complications
Although there was no significant difference in the postoperative complication rate between the two-scope group B and the open surgery control group (P>.05), the complication rates of the other three groups were significantly lower (P<.05) than that of the control group (Table 2). The most common complications at the endoscopic treatment phase were mild pancreatitis and post-EST bleeding; the major complications at the laparoscopic treatment stage were incision infection, bile leakage, and postoperative mild pancreatitis. All complications were cured by symptomatic treatment, and no surgery-related deaths occurred.
Operation time
Local pharyngeal anesthesia with mild systemic effects was used in the one-scope protocol; its operation time was not used for statistical processing. Only LC was performed in the laparoscopic stage of the two-scope protocol, so there was no comparative significance. The statistical results revealed that the operation time of the three-scope group was shorter than that the open surgery group and the two-scope group B (P<.05). The difference between the two-scope group B and the open surgery group was not statistically significant (P>.05) (Table 3).
P<.05 for two-scope group B versus three-scope group; P>.05 for two-scope group B versus open surgery group; P<.05 for three-scope group versus two-scope group B and three-scope group versus open surgery group.
P<.05 for comparisons between the four minimally invasive treatment protocols and the open surgery group.
Hospital stay
The length of the hospital stay of the four minimally invasive treatment protocols was shorter than that of the open surgery. As shown in Table 3, a phasic increase was observed in the length of the hospital stay of the four minimally invasive treatment protocols, and the difference was significant (P<.05).
Discussion
The treatment of extrahepatic bile duct stones by laparoscopy and endoscopy has been well developed in many domestic and foreign medical centers.5–7 However, a complete, serial standardized, minimally invasive treatment protocol has not been established. Additionally, a single treatment protocol does not fit all patients.2,5,6 In recent years, based on the clinical experiences of using endoscopy and laparoscopy in our hospital, we have developed a complete phasic protocol through clinical studies on the minimally invasive treatment of 2668 cases of extrahepatic bile duct stones. The protocol has been applied according to the specific conditions of the patients, fully reflecting the standardization of the protocols and the superiority of minimally invasive treatment. 7
The phasic protocol complies with the principles of conventional treatment. ERCP is typically applied first to relieve the biliary obstruction. Various minimally invasive techniques have been combined to maximize their advantages. Compared with conventional open surgery, the phasic treatment protocol displayed less trauma, shorter hospital stays, and rapid postoperative recovery.8–13 It also avoids the enormous patient suffering caused by the conventional open operation.14–17 In addition, phasic application standardizes the treatment. According to the specific conditions of the extrahepatic bile duct stones, four minimally invasive protocols can be applied step by step to avoid the disadvantages of a single treatment mode.
The three-scope protocol was first proposed by our hospital. It is the best combination of three minimally invasive techniques to treat complex extrahepatic bile duct stones and attempts to minimize the trauma in the current treatment of this disease. This protocol further completes and standardizes the treatment scheme.
Some considerations do exist when using this phasic treatment protocol. The endoscopic treatment indications must be examined strictly. A middle incision should be made in EST, which cannot only prevent late postoperative cholangitis or stone recurrence, but also maintain the function of the sphincter to the greatest extent. For patients with severe acute cholangitis, ENBD should be performed first by duodenoscopy, followed by biliary decompression and drainage. In cases such as these, EST should not be used if possible. After the condition becomes stable, the feasibility of stone removal by duodenoscopy should be decided by ERCP. In addition, for patients with extrahepatic bile duct stones complicated with cholecystolithiasis, if endoscopic stone removal is difficult to perform, such patients should be switched to the three-scope protocol because of the need for the management of gallstones. In this way, the increase of complications caused by a large incision into the papillary sphincter or lithotripsy can be prevented. Both gallstones and extrahepatic bile duct stones can be removed in a one-step procedure, and the integrity of the biliary system can be safely maintained. Suture type is another consideration. Using 2-0 or 3-0 atraumatic absorbable sutures can reduce the damage caused by the suture on the bile duct wall and prevent the descent of the thread knot into the bile duct, which can become the core of a recurred stone. In order to prevent bile duct stricture and postoperative bile leakage after bile duct suturing, interrupted sutures should be adopted, and the distance of needles and edges should generally be controlled at 1.5–2.0 mm.
Combination of endoscopy and laparoscopic maximizes their respective strengths, further expands the range of minimally invasive treatment, and enables the patients with intrahepatic and extrahepatic bile duct stones to benefit from the minimally invasive treatment to the maximum extent. It fully reflects the advantages of the combination of two minimally invasive techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.