
Abstract
Abstract
Introduction:
Surgical resection represents the only therapeutic action having a radical intent for the treatment of resectable esophageal neoplasms. Minimally invasive esophagectomy for esophageal cancer is being more and more frequently performed. Few cases of esophagectomy after pneumonectomy have been described in the literature, and, to our knowledge, none of them was performed by the minimally invasive technique.
Subject and Methods:
A 77-year-old woman, who had undergone left thoracotomic pneumonectomy due to squamous cell lung cancer 2 years before, underwent minimally invasive esophagectomy because of esophageal cancer at the authors' institution. The intervention was performed by right thoracoscopic esophageal mobilization with the patient in the prone position, followed by the laparoscopic and cervicotomic stages, with cervical anastomosis.
Results:
Total operative time was 230 minutes. Intensive care unit stay was 1 day, followed by a hospital stay of 13 days. We did not observe any major postoperative complication.
Conclusions:
Minimally invasive esophagectomy with thoracoscopic esophageal mobilization in the prone position is a valid option in the treatment of esophageal cancer and may be feasible in previously left pneumonectomized patients.
Introduction
Several minimally invasive approaches for esophagectomy have been described: laparoscopic transhiatal, thoracoscopic, thoracolaparoscopic, videomediastinoscopic, endoscopic Ivor Lewis, and laparoscopic esophagogastrectomy. 3 Some authors have already concluded that minimally invasive esophagectomy is feasible and safe and can produce better outcomes than those reported in most open series. 4
Thoracoscopic dissection and esophageal mobilization were first decribed by Cuschieri et al., 5 and Cuschieri 6 subsequently described the thoracoscopic mobilization of the esophagus with the patient in the prone position. Thoracoscopic esophageal mobilization in the prone position seems to be equivalent to that performed in the lateral decubitus position with regard to the number of dissected lymph nodes, blood loss, and complications, with reduction of the thoracoscopic surgical time. 7
Few cases of esophagectomy after pneumonectomy have been reported in the literature, and, to our knowledge, none of these was performed by the minimally invasive technique. In this report we present a case of minimally invasive esophagectomy by thoracoscopy in the prone position and laparoscopy, because of esophageal cancer, in a patient who had previously undergone pneumonectomy due to lung cancer. The surgical technique of esophagectomy was substantially similar to the one described by Cadière et al. 8 We had previously performed such a surgical technique in over 40 patients with esophageal cancer.
Patient and Methods
A 77-year-old woman came to our observation because of dysphagia for solid food that she had had for about 2 months, regurgitation, mild retrosternal pain, and modest weight loss. The patient, a former smoker, had undergone left thoracotomic pneumonectomy because of squamous cell lung cancer (graded, according to the American Joint Committee on Cancer TNM classification for lung cancer, as pT2N0M0) 2 years before (Fig. 1). The patient had previously undergone appendectomy and bilateral inguinal hernioplasty, and she was hemiparetic due to a previous ischemic stroke.
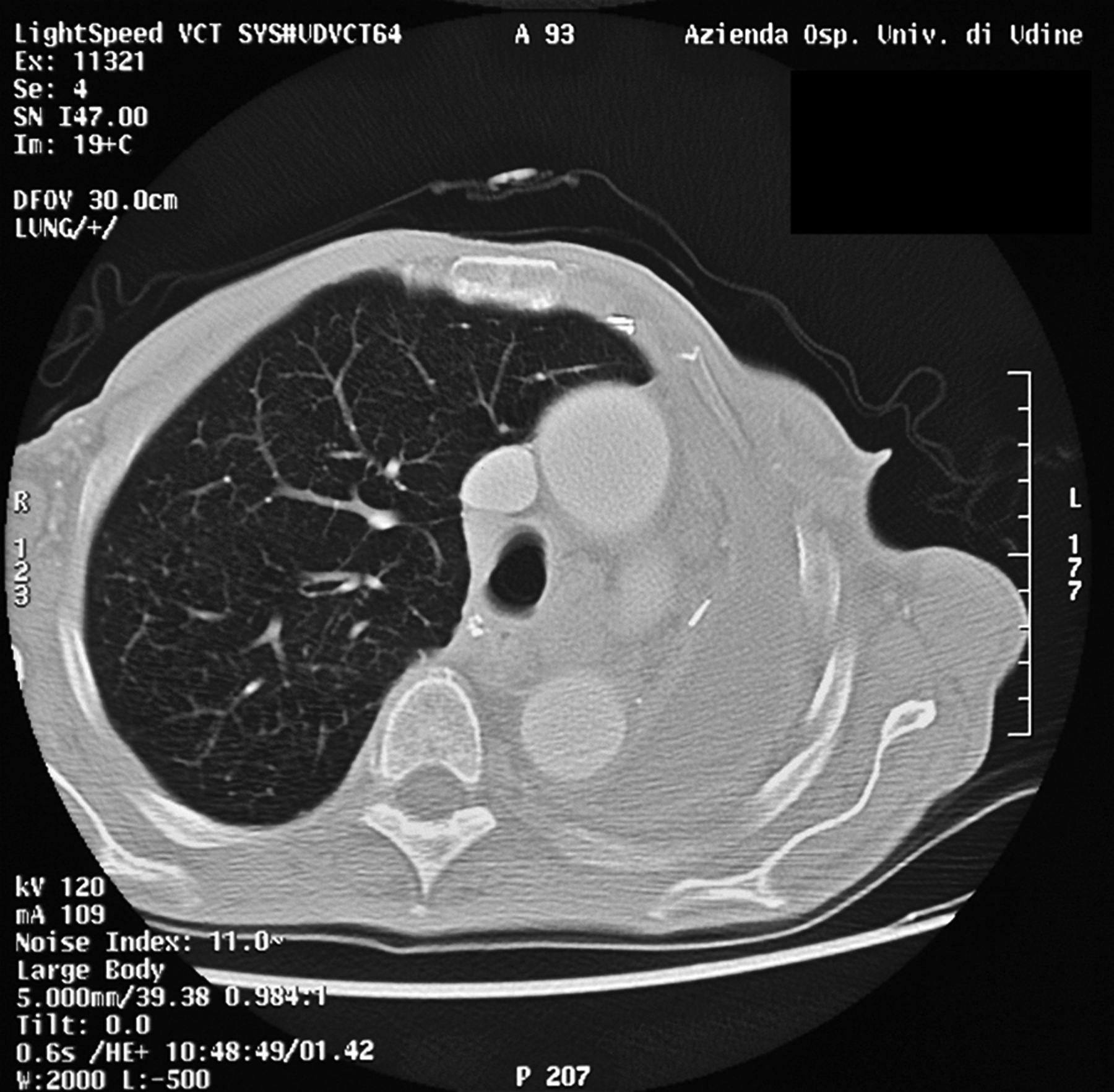
Preoperative computed tomography scan showing the results of the previous left pneumonectomy.
Because of the symptoms reported, esophagogastroduodenoscopy with biopsies was performed; it revealed the presence of an ulcerated neoplasm at the lower third of the esophagus with extension to the cardia (between 35 and 40 cm from the dental arches). The histological examination revealed a moderately differentiated squamous esophageal cancer. Computed tomography scan was subsequently performed; it confirmed the site of the esophageal tumor and showed the presence of some lymph nodes in the Barety space whose major diameter was about 13 mm. There was no evidence of metastatic disease.
The preoperative evaluation of the patient was completed with bronchoscopy. There was no evidence of pathological lesions. Respiratory function tests showed evidence of a mild degree of restrictive deficit associated with severe reduction of the capacity to transfer carbon monoxide. Otolaryngologic evaluation was also performed. The restaging of the lung cancer was negative. According to the physical status classification system of the American Society of Anesthesiologists, the preoperative evaluation resulted in stage 3.
Anesthetic management
The patient was premedicated with morphine sulfate (5 mg i.m.) and scopolamine (0.25 mg i.m.). An intravenous catheter was inserted into a peripheral vein, and a 20-gauge radial artery catheter was applied and connected to a FloTrac™ sensor system with a Vigileo™ monitor (Edwards LifeSciences, Irvine, CA) for measuring cardiac index, stroke volume, and systemic (arterial) blood pressure. A central venous catheter was inserted via the right jugular internal vein for monitoring central venous oxygen saturation (PreSep™ catheter; Edwards LifeSciences) and central venous pressure. Monitoring equipment for electrocardiogram and pulse oximetry was applied.
Anesthesia was induced by propofol and remifentanil. Tracheal intubation was performed with a 7.5-mm cuffed single-lumen standard tube after muscle relaxation was established by intravenous injection of cisatracurium. Anesthesia was maintained by desflurane and remifentanil.
The patient was ventilated with an air/oxygen mixture using a SERVO-i ventilator (Maquet, Solna, Sweden) set in a volume-controlled mode. Tidal volume (TV) of 4–5 mL/kg, breathing frequency of 14–16 breaths/minute, and positive end-expiratory pressure (PEEP) of 3–4 cm H2O were used. The fraction of inhaled oxygen was set between 50% and 70%, and low TV and low PEEP allowed a partial lung collapse and therefore a sufficient surgical view of the esophagus. Both respiratory rate and TV were continuously adjusted to obtain an end-tidal concentration of CO2 between 40 and 45 mm Hg.
Later, the patient was placed in the prone position upon a surgical bean bag, and all the rules to prevent bedsores or accidental injury (vascular and nerve) were applied: the arms were abducted to 90° with the flexed forearms an additional 90°.
During thoracoscopy the patient was ventilated using a respiratory rate of 16–18 breaths/minute, maximum TV of 5 mL/kg, and PEEP of 3–4 cm H2O. The arterial O2 pressure (PaO2) was not changed, whereas the CO2 pressure did not significantly increase. At the end of the thoracoscopic stage, recruitment maneuvers were performed to restore ventilation in dorsal atelectatic segments of the lung. PaO2 and CO2 pressure returned to baseline. After the thoracoscopic stage was concluded, the patient was placed in the supine position to continue the laparoscopic and the cervicotomic stages.
Operative procedure
Stage I: thoracoscopy
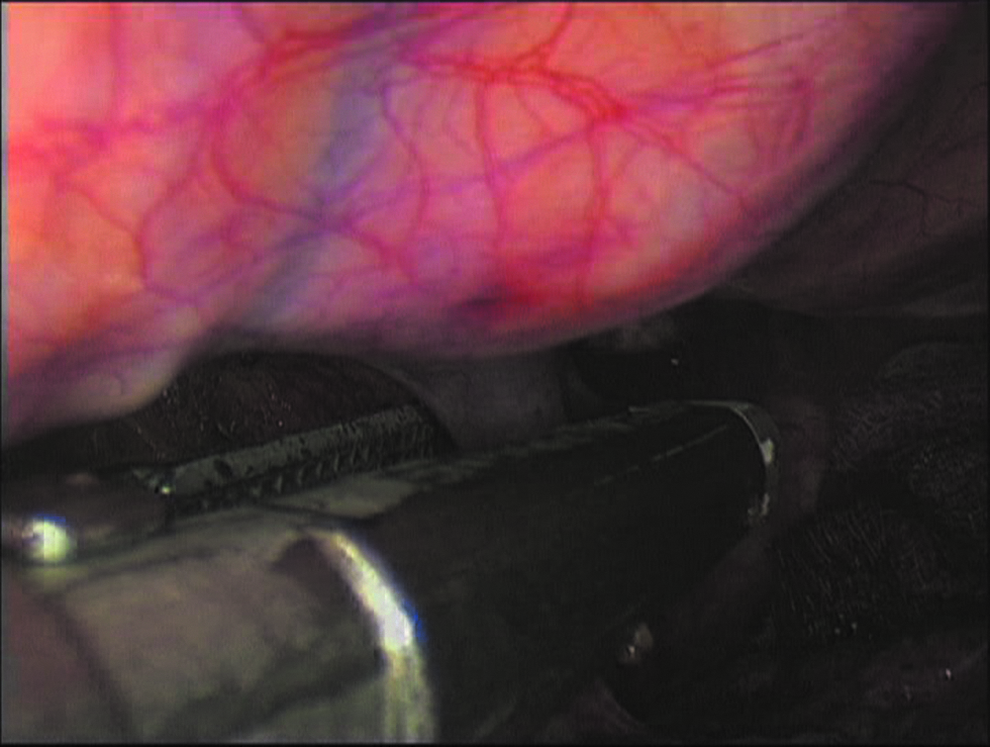
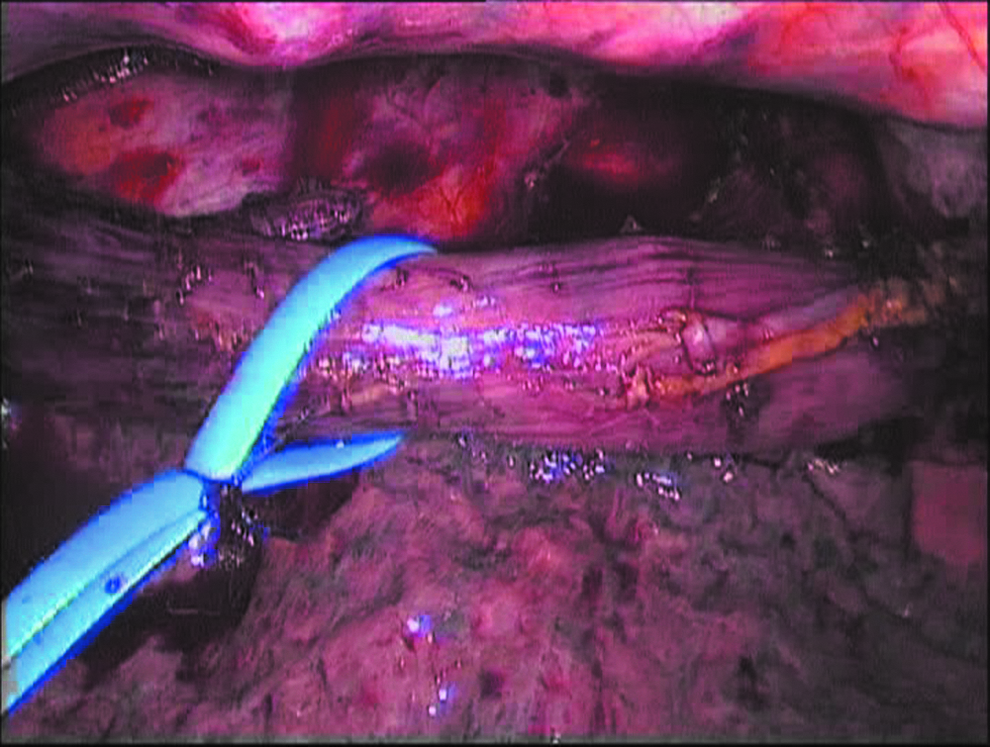
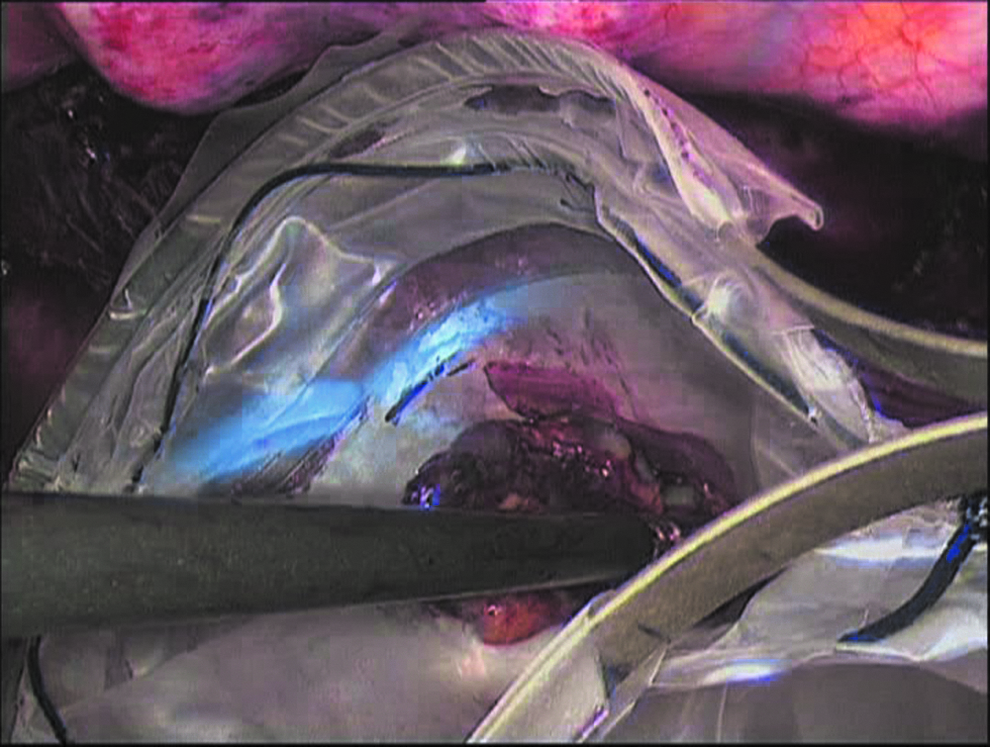
A right posterior thoracoscopic access in the prone position was performed using three trocars: a 10-mm trocar for a 30° angled scope in the seventh intercostal space near the apex of the scapula, a 5- or 10-mm trocar in the fifth space between the spinous process and the scapula as close as possible to the latter, and a 12-mm trocar in the ninth space on the posterior axillary line. A transitory pneumothorax using CO2 was performed, establishing a pressure of 7–8 mm Hg. The tumor, with a major diameter of 3 cm, was identified at the lower thoracic esophagus; no clinically suspicious neighboring lymphadenopathy was detected. After the pulmonary ligament and the mediastinal pleura were sectioned (Fig. 2), the azygos vein was isolated and divided at the level of its arc, using a vascular stapler (Fig. 3). Subsequently, the dissection of the esophagus en bloc with the periesophageal tissue was completed, caudally to the diaphragmatic hiatus and cranially to the pleural dome (Fig. 4); the inter-tracheobronchial nodal packet was separately removed (Figs. 5 and 6). A chest tube drain was placed through the port site of the ninth space.
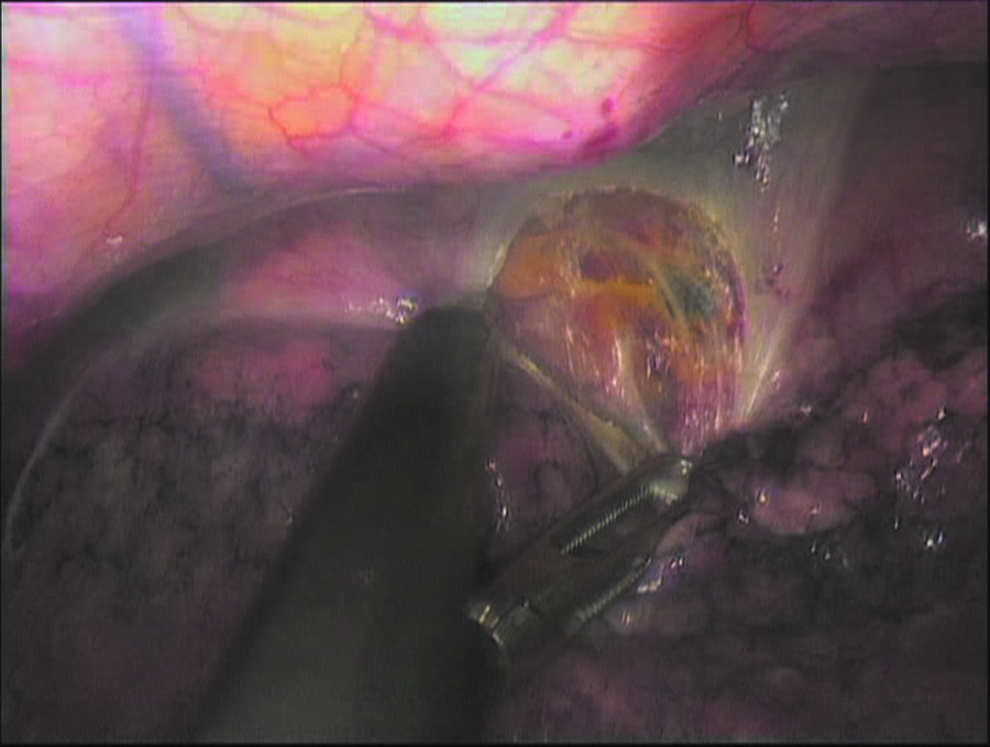
Section of the mediastinal pleura.
Section of the azygos vein using a stapler.
Isolation of the esophagus.

Separate removal of the inter-tracheobronchial nodal packet.
Removal of the inter-tracheobronchial nodal packet with an Endo Catch™ bag (Covidien, Norwalk, CT).
Stage II: laparoscopy
After the patient was positioned in the supine position with spread legs, open laparoscopy was performed with supraumbilical access, and three other trocars were placed: in the epigastrium and in the right and left upper quadrants. After Kocher's maneuver was performed, the stomach was mobilized, preserving the right vessels. The short gastric vessels and the posterior gastric artery were divided, and the preparation of the gastric fundus was completed to the left diaphragmatic pillar. Subsequently, the small omentum was sectioned to the right diaphragmatic pillar, and the terminal esophagus was dissected to the inferior mediastinum. The left gastric vessels were divided at their origin. Finally, a gastric tube was constructed by means of multiple firings of the endoscopic stapler. Pyloromyotomy was not performed. The celiac lymph nodes were dissected.
Stage III: cervicotomy
Left cervicotomy along the anterior border of sternocleidomastoid muscle was performed, and the cervical esophagus was isolated after the ipsilateral recurrent nerve was identified. Subsequently, the esophagus was divided, and its lower stump was connected to a 36 French silicone tube. The gastric tube and the esophagus connected to the silicone tube were exteriorized through a minilaparotomy in the epigastrium. The gastric tube was divided below the cardia. The gastric tube was brought up to the neck under laparoscopic control, without twisting, using the silicone tube as a guide. An end-to-side anastomosis between the esophageal stump and the gastric tube was performed with a 25-mm circular stapler. Subsequently, the lateral stump of the gastric tube was divided and sutured with a linear stapler. Finally, a suction drain was placed near the anastomosis.
Results
Total operative time was 230 minutes. There was no need of blood transfusions during surgery, and the patient remained hemodynamically stable with preserved gas exchange. After surgery, the patient was admitted to an intensive care unit. The patient was mobilized on postoperative Day 1, received regular chest physiotherapy, and was encouraged to use an incentive spirometry every hour while awake. Nasojejunal feeding was started on the first postoperative day at 30 mL/hour. On postoperative Day 1 the patient was transferred to the surgical department.
Postoperative pain therapy was conducted by administering intravenous tramadol (50 mg b.i.d.) and acetaminophen (500 mg t.i.d.), for 2 days; subsequently, acetaminophen (500 mg) was administered only as needed, until postoperative Day 15.
On postoperative Day 3, because of low-grade fever (temperature of 37.2°C) and increased leukocyte count, bronchoscopy was performed; a moderate quantity of endobronchial secretions was aspirated. For this reason intravenous antibiotic therapy (ciprofloxacin) was empirically set, followed by rapid normalization of the temperature curve and the value of the leukocyte count. Antibiotic therapy was maintained until postoperative Day 14.
During hospitalization, the patient maintained normal values of gas exchange and diuresis. Because of moderate anemia, without clinical evidence of blood loss, 2 units of packed red blood cells (one on postoperative Day 4 and another on Day 18) were transfused.
The aspiration of the chest drain was stopped on postoperative Day 4, and the drain was removed on Day 8.
On Day 8 the nasogastric tube was removed, after execution of upper gastrointestinal tract radiography with water-soluble contrast medium (diatrizoate meglumine and diatrizoate sodium solution [Gastrografin®; Bayer AG, Leverkusen, Germany]) to exclude the presence of anastomotic stenosis or leak. On postoperative Day 12 the patient began to take fluids by mouth and on Day 13 also solid food, with no problem. The patient was discharged on postoperative Day 30.
Histological examination of the specimen revealed a moderately differentiated (G2) squamous cell carcinoma of the lower third of the esophagus, with full-thickness infiltration of the esophageal wall; the resection margins were free of tumor. Endolymphatic carcinosis and metastatic invasion in 5 of 16 lymph nodes obtained were detected. According to the American Joint Committee on Cancer TNM classification for esophageal cancer, defined on the basis of the final histology, the stage of disease was pT3N1M0 (Stage III).
Under radiotherapic and oncological evaluations, the patient did not receive either neoadjuvant or adjuvant therapies.
Endoscopic dilatation was performed 8 months after surgery because of anastomotic stenosis. At the last observation, 1 year after surgery, the patient was in fairly good health, was eating regularly, and she was disease free.
Discussion
Whereas esophagectomy was associated with high rates of morbidity and mortality in the past, death rates are less than 10% at present. The credit for this improvement has been mainly attributed to preoperative patient selection, improvements in anesthesia, surgical techniques, and postoperative care management. 9 Respiratory problems remain the major cause of both morbidity and mortality after esophagectomy for cancer. 10
Several minimally invasive approaches for esophagectomy have been described. They are aimed at reducing the morbidity rate related to the traditional open technique. A minimally invasive esophagectomy can be performed by laparoscopic transhiatal, thoracoscopic, thoracolaparoscopic, videomediastinoscopic, endoscopic Ivor Lewis, and laparoscopic esophagogastrectomy. 3 Cadière et al. 8 demonstrated that thoracoscopic and laparoscopic esophagectomy with extended lymphadenectomy is technically feasible and safe and that thoracoscopy in the prone position improves the quality of dissection. The main advantage of the prone position is that it is not necessary to recline or selectively deflate the lung to obtain good working conditions. 8 Because of its excellent ergonomics, this technique allows the operative time to be reduced and better respiratory results to be obtained. 3 Furthermore, the thoracoscopic intervention can be performed using only three trocars instead of the four necessary in the lateral decubitus position. 4
Some authors have demostrated that esophagectomy after lung lobectomy can be safely performed.11,12 Tokumitsu et al. 13 described a case of mediastinoscope-assisted transhiatal esophagectomy after pulmonary lobectomy. Few cases of esophagectomy after pneumonectomy have been described in the literature, and, to our knowledge, none of them was carried out by the minimally invasive technique.14,15
When a thoracic intervention is indicated in a pneumonectomized patient, it is essential to know the anatomic and physiologic changes in the postpneumonectomy state, such as the mediastinal shift toward the operated side, the elevation of the ipsilateral hemidiaphragm, and the hyperexpansion of the remaining lung.15,16 On the other hand, transhiatal esophagectomy may not be technically safe and feasible because of anatomic changes and adhesions after pneumonectomy and nodal dissection. 15
Our data show that the prone position approach provided good oxygenation and reduced bleeding. These findings indicate that esophagectomy in the prone position results in a useful technique also in left pneumonectomized patients, via the right side. The choice of the right pleural cavity has made the surgical dissection simpler for two reasons: the anatomical position of the esophagus in the mediastinum and the absence of scars and adhesions. On the other hand, the intervention performed through this approach was possible as the technique we used was compatible with the ventilation of the residual lung. The main consequences of that simplified dissection are the short operative time and the absence of such intraoperative complications as chylothorax, bleeding, and recurrent laryngeal nerve injury.
The lateral decubitus position reduces the functional residual capacity of the ventilated lung for several reasons, the most important of which is because the ventilated lung is pressed on by the mediastinum and the nonventilated lung, thereby leading to atelectasis. In our case only the mediastinum could be the cause of the decrease of functional residual capacity. Another cause is an increase of the intra-abdominal pressure that displaces the diaphragm cranially when the patient is in the lateral decubitus position. 17
The prone position offers several advantages in esophagectomy: first of all, lung injury is minimized because lung retraction is not necessary thanks to gravity; moreover, the anatomic esophageal exposition is excellent. 18 Nyrén et al. 19 concluded that, in anesthetized and mechanically ventilated healthy individuals, ventilation is not affected by posture, whereas it is gravity dependent. The prone position favors a more evenly distributed perfusion in the different lung regions. 20
The position of the patient is likely to be important when he or she is placed in the prone position. The one-lung ventilation causes a marked reduction in static compliance and a decrease in PaO2 with retention of CO2 and may induce some degree of alveolar damage because elevated airway pressure can cause barotrauma to a ventilated lung. This might cause significant lung damage and resultant hypoxemia if a patient has underlying lung disorders such as chronic obstructive pulmonary disease or if the procedure under one-lung ventilation is prolonged. We have overcome this problem because all the patients who undergo minimally invasive esophagectomy in the prone position are intubated with a single-lumen endotracheal tube and then the ventilation of both lungs is maintained. The ventilatory parameters are adjusted so that the excursion does not interfere with the lung surgery.
The fact that no condition referable to intra- or postoperative respiratory failure has occurred shows conclusively that, with the patient in the prone position, the ventilation of the lung of the side on which the surgeon operates is also substantially normal.
In this case we have demonstrated that minimally invasive esophagectomy with thoracoscopic esophageal mobilization with the patient in the prone position is feasible in previously left pneumonectomized patients. In our opinion, the patient could not be operated on in any other way, given the risks of conducting the intervention with a transhiatal approach in a previously pneumonectomized patient.
The postoperative hospital stay of our patient was longer than the median stay presented in the literature. 3 This can be explained by the important co-morbidities of the patient. On the other hand, we did not observe any major postoperative complication.
Footnotes
Disclosure Statement
No competing financial interests exist.