
Abstract
Abstract
Background:
In recent years, day-case laparoscopic Nissen fundoplication (LNF) has became popular. Our study aims to evaluate the effect of patient factors and severity of gastroesophageal reflux disease measured by DeMeester score on the success of day-case LNF.
Subjects and Methods:
We conducted a retrospective case series review of patient demographics (age, gender, body mass index [BMI], and smoking status) and DeMeester score over a 5-year period. Between 2005 and 2010, 112 patients had day-case LNF. Same-day discharge was achieved in 80.3%. Twenty-two patients (19.7%) required postoperative admission (“failed day-case surgery”), with a resultant mean length of stay of 1.41 days. Univariate analysis showed that female gender had a significantly higher incidence of postsurgical admission (30.76% females versus 13.69% males, P=.03 by Mann–Whitney U test). Compared with the same-day discharge group, the failed day-case group has a higher mean DeMeester score (50.89 versus 36.03, P=.021 by t test) and BMI (28.71±0.778 kg/m2 versus 26.79±0.3737 kg/m2, P=.023). Age and smoking status were not significant determining factors in postoperative admission rates. Using multivariable analysis and logistical regression, we derived a model based on gender, BMI, and DeMeester score to predict the probability of admission following day-case LNF.
Conclusions:
We conclude that day-case LNF is a safe, feasible procedure in the appropriately selected patient population. Our novel finding of higher admission rates in females, high DeMeester score, and high BMI should be used in planning perioperative hospitalization in this cohort.
Introduction
Classically, GERD surgery involved open techniques that have long-lasting impacts on the patient's quality of life, earnings, and recovery period. However, within the last two decades, there has been a radical movement toward minimally invasive surgery and toward day-case laparoscopic surgery in recent years.
Laparoscopic Nissen fundoplication (LNF) has become the surgical treatment of choice for patients with clinically symptomatic GERD. It is generally a safe and well-tolerated procedure by patients. Several case series have shown LNF to be a feasible outpatient procedure; however, selection criteria are unclear.1,9–11 Within the last decade, there has been a three- to fivefold increase in LNF.12–14 At our institution, LNF has been the default protocol pathway for over 7 years. LNF effectively decreases acid reflux and associated symptoms. Pre- and postprandial lower esophageal sphinter pressures are increased postsurgery, 5 resulting in the reduction of total esophageal acid exposure.9–11
Our study aim is to evaluate the effect of patient factors (age, gender, body mass index [BMI], and smoking status) and severity of GERD measured by DeMeester score on the success of day-case LNF.
Subjects and Methods
Our retrospective review focuses on the preoperative assessment, patient demographics, intraoperative management, and postoperative follow-up of all LNFs carried out by two surgeons in our university teaching hospital. The studied parameters were DeMeester score and patient demographics, including age, gender, BMI (in kg/m2), and smoking status (current smokers versus never-smokers). Using our results we offer a scoring system to risk-stratify patients who are likely to have unplanned postoperative LNF admission.
All patients selected for day-case LNF undergo a standard work-up that includes trial of a proton pump inhibitor, esophogastroduodenoscopy, manometry, 24-hour pH study, and surgical consultation in the outpatient department. All potential day-case candidates were also assessed preoperatively by a consultant anesthetist at an outpatient setting. To qualify for day-case assessment, patients were required to have a BMI of <35 kg/m2 and an American Society of Anesthesiologists grade of 2 or less. Those patients who were not eligible for day-case LNF were not the subject of our investigation and therefore were not included in our analysis.
Day-case surgery is defined as “elective outpatient surgery” without formal admission to the hospital. Patients come to the hospital (day-ward) the morning of surgery (typically 6:30 a.m.) and are discharged the same day (typically 4 p.m.).
All patients had the same perioperative standard protocol for medications including analgesia and anti-emetics, and all were informed of the procedure including risk, benefits, postoperative care, and dietary advice (soft diet for 6 weeks). The proton-pump inhibitor is continued until 6 weeks postoperatively. The LNF was done with the patient under a standard general anesthetic. The patient was positioned in supine lithotomy, and four laparoscopic ports were placed. Full mobilization of the distal esophagus was done, with reduction of a hiatus hernia if present. The esophagophrenic ligament was divided with preservation of the vagi. Both surgeons have similar techniques with dividing the short gastric arteries to create a “floppy” short wrap over the lower end of the intra-abdominal esophagus. One surgeon (P.F.R.) excludes the vagus from the wrap, whereas the other (K.C.C.) includes the vagus in the wrap. A 52 French bougie was used in all cases, and both use the “shoe-shine” maneuver.
Parametric data are expressed as mean±standard deviation values, with significance of differences calculated using the t test and nonparametric analysis using the Mann–Whitney U test. Statistical analysis was performed using GraphPad Prism version 5.03 for Windows (GraphPad Software, San Diego, CA). Multivariate analysis was performed using IBM SPSS version 19.0 software (www.spss.com; SPSS, Chicago, IL). The continuous variables gender, BMI, and DeMeester score were recoded as categorical variables. Using admission status as the outcome variable, stepwise logistic regression was performed using both forward and backward methods.
Results
One hundred twelve patients with symptoms of GERD, refractory to medical treatment and eligible for day-case surgery, underwent LNF between June 2005 and June 2010. Same-day discharge occurred for 90 patients (80.3%). Twenty-two patients (19.7%) were admitted postoperatively as “failed day-case.” The mean stay was 1.41 days (range, 1–4 days). There were also 2 patients (1.7%) admitted within 1 month postoperatively because of mild dysphagia. Both patients underwent normal esophogastroduodenoscopy and were discharged with no further intervention needed.
Factors mandating admission after LNF included pain (11 patients), nausea (5 patients), urinary retention (3 patients), postoperative oxygen requirements >4 hours (2 patients), and for postoperative observation (1 patient). There were no deaths or conversion to open procedures in the series.
The age range for the study period was 18–63 years, with a median age of 40 years. We found that age had no statistical significance in admission rates. The mean age for the day-case and failed day-case cohort was 40.18±1.237 years and 39.41±2.088 years, respectively, with a median of 38 years for both cohorts (P=.77 by t test) (Table 1).
Data are mean±standard deviation values or percentages as indicated.
Significant difference.
Of the patients, 65.18% (n=73) were male, and 34.82% (n=39) were female. Females were more likely to have failed day-case (30.76% females admitted versus 13.69% males admitted, P=.03 by Mann–Whitney U test) (Fig. 1).
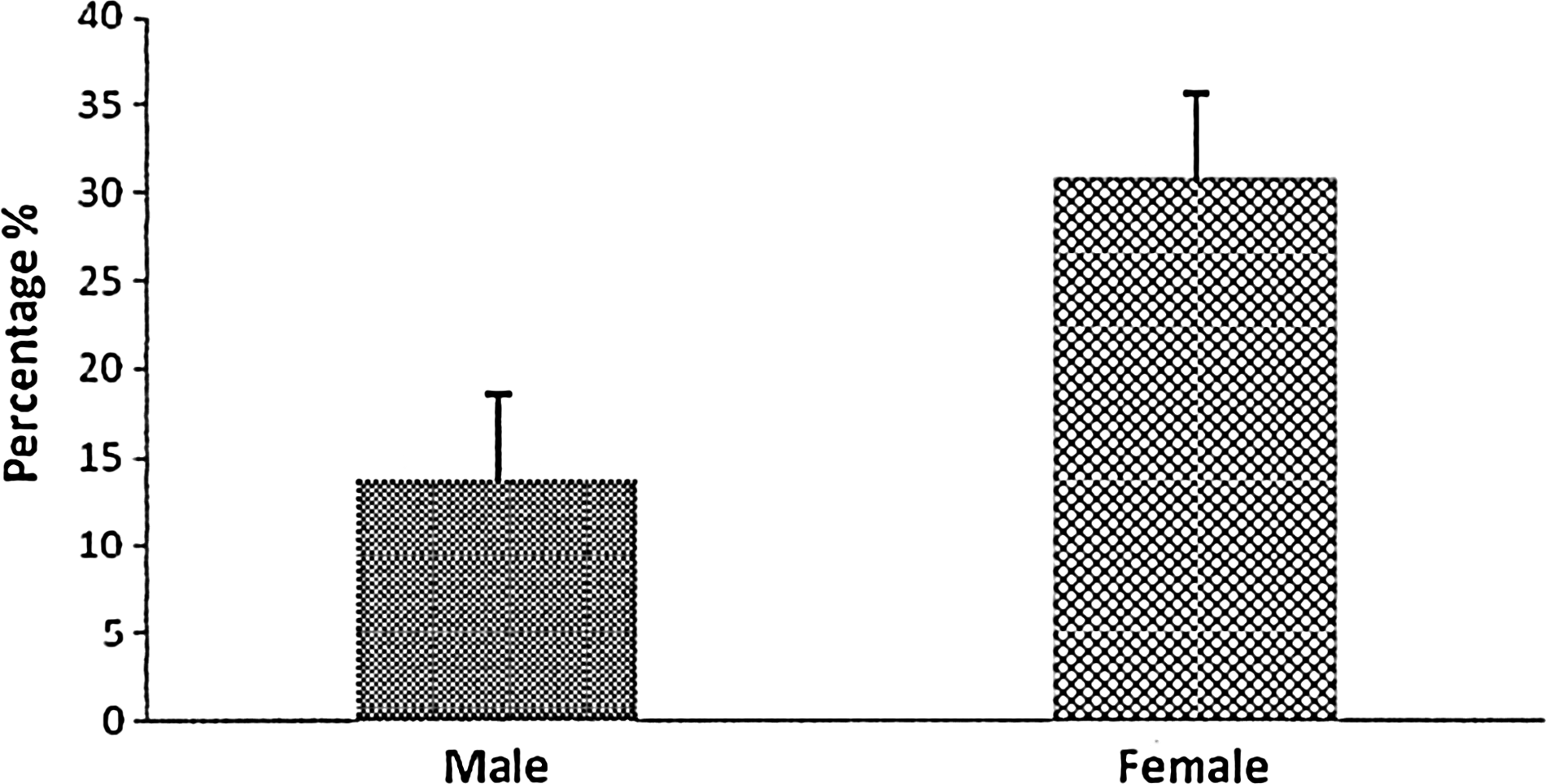
Gender comparison in the unplanned admission cohort (P=.03).
BMI of 108 patients was examined and was found to have an effect on failed day-case postoperative LNF. For the same-day discharge group, the mean BMI was 26.79±0.3737 kg/m2, whereas that of the failed day-case group was 28.71±0.7781 kg/m2 (P=.023 by t test) (Fig. 2). Our cohort BMI range was 18–38 kg/m2.
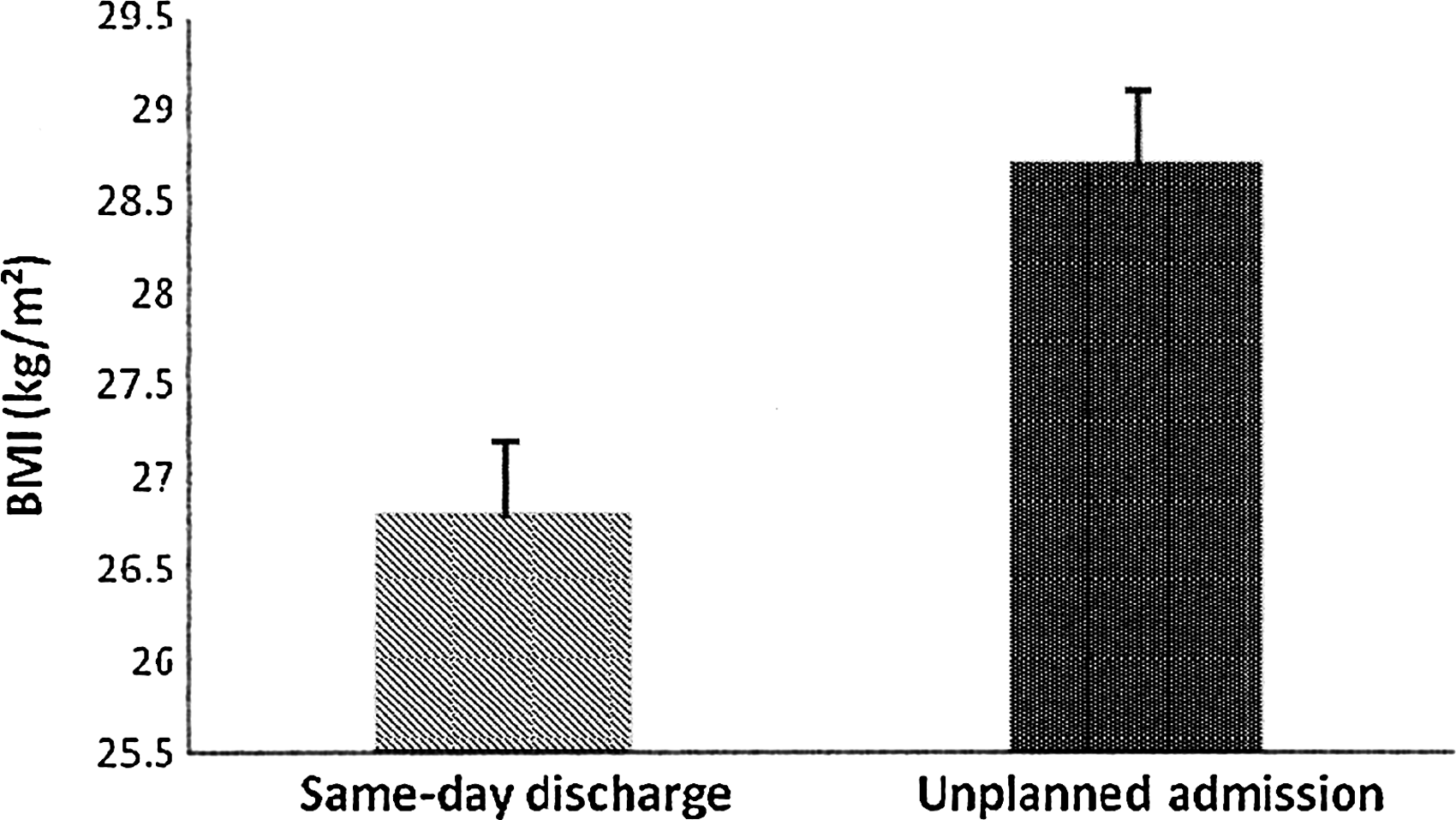
Mean body mass index (BMI) in same-day discharge and unplanned admission groups on postoperative laparoscopic Nissen fundoplication (P=.02).
DeMeester score was higher among the failed day-case group compared with the same-day discharge group (50.89±7.850 and 36.03±2.443, respectively; P=.020 by t test) (Fig. 3). Male patients' DeMeester score in the failed day-case group was 64.23±16.72, whereas that for the same-day discharge group was 41.14±3.261. Female patients' DeMeester score in the failed day-case group was 43.12±7.467, whereas that of the same-day discharge group was 25.31±2.276. The failed day-case groups for both male and females had statistically higher DeMeester scores (respectively, P=.0370 and P=.0055 by t test).

DeMeester score in same-day discharge and unplanned admission groups on postoperative laparoscopic Nissen fundoplication (P=.02).
Of those who had failed day-case LNF, 19.1% were current smokers, whereas 20.2% of the successful same-day discharged group were smokers. Smoking status did not have a significant impact on failed day-case admission rate postoperatively (P=.96 by Mann–Whitney U test).
After identifying independent variables associated with admission using 102 cases with complete data, we recoded gender, BMI, and DeMeester score as categorical variables and used logistic regression to build an equation predicting hospital admission probability. We found that these variables were significantly associated with failed day-case postoperative admission. Points for gender, BMI, and DeMeester score are assigned for each patient (Table 2).
The mathematical equation derived from logistic regression is:
where p=–5.184+(2.072a)+(1.007b)+(0.855c), a=gender points (where 1 is female and 0 is male), b=BMI points between 0 and 2, and c=DeMeester points between 0 and 4.
For example, a female patient with a BMI of 28 kg/m2 and a DeMeester score of 50 would have gender=1 point, BMI=2 points, and DeMeester score=3 points (Table 2). According to our equation, she would have an overall 81.3% probability of being admitted postoperatively as a failed day-case procedure.
Using this equation we generated a model called the Tallaght LNF Score to assist in identifying high-risk patients and to quickly predict the probability of postoperative admission as failed day-case LNF (Tables 3 and 4). For the same patient mentioned above, we would use the Female Tallaght LNF Score (Table 4). She has a total score of 5 points (2 points for BMI and 3 points for DeMeester score). Therefore her probability of being admitted postoperatively as a failed day-case procedure is 79%–81%. For male patients, we use the Male Tallaght LNF Score (Table 3).
BMI, body mass index; LNF, laparoscopic Nissen fundoplication.
BMI, body mass index; LNF, laparoscopic Nissen fundoplication.
Our model, the Tallaght LNF Score, is 83% accurate in predicting the probability of admission as failed day-case LNF (Cox and Snell R 2 of 0.198 and a Nagelkerke R 2 of 0.31).
Discussion
Since the introduction of the laparoscopic approach to anti-reflux surgery and the publication of evidence supporting its long-term efficacy,15–18 there has been increasing demand by both patients and referring physicians. The 48-month follow-up has 91% approval satisfaction, and at 10 years there is 91%–98% satisfaction.15–18 Like all minimally invasive surgery, LNF shows benefits in reduction of hospital stay, early mobilization, less analgesia need, lower incisional hernia incidence, and notable cost savings.13,14 After 8 years, LNF has a cost-saving benefit when compared against medical treatment. Medical treatment of GERD in England has an annual cost in excess of £233 millions.19,20 In the United States, patients spend an estimated $5 billion on anti-reflux medicines. 21
At our institution, day-case LNF has been the default protocol pathway for the last 7 years. Twenty-two patients (19.7%) were admitted unplanned postoperatively as failed day-cases. The mean stay for these admitted patients was 1.41 days. In the REFLUX and LOTUS trials the mean stay was 2 days. 22 In our study, we had a lower mean stay than that reported in these trials, with a cost-saving effect.
On further univariate analysis, we note that patient demographics and disease status have considerable consequence in the success of same-day discharge. We report a statistical difference in BMIs of same-day discharge and failed day-case patients. The fact that most patients in the study were in the overweight category (BMI, 25–30 kg/m2) reflects on our increasing epidemic rate of obesity in society and on the patients seeking medical attention for this condition. Other studies have shown that preoperative BMI has a significant factor in the long-term outcome of anti-reflux surgery. 23 Patients with high BMI are the most common group for reported failure.23,24 In our institution, we only advocate day-case LNF in patients with a BMI<35 kg/m2. In those with BMI>35 kg/m2, inpatient LNF is the default pathway; however, patients are informed of the higher chance of conversion to open Nissen fundoplication. Furthermore, all patients with BMI>30 kg/m2 are encouraged to attempt weight loss as this has a significant impact on the 10-year success rate. From our review, we note that the mean BMI was 26.79±0.3737 kg/m2 for the same-day discharge group, whereas that of the failed day-case group was 28.71±0.7781 kg/m2 (P=.023). We do acknowledge that the difference of these BMIs is low, and this is a limitation of our Tallaght score. However, we have shown that BMI still has a statistically significant impact; thus we use this to encourage optimization of weight prior to surgery.
Age did not play a significant role in the number of unplanned admission postoperatively. It is interesting that females had higher unplanned admission rates. More female patients were admitted following day-case LNF for pain and nausea control (n=6 and n=5, respectively), despite being given the same analgesia and anti-emetics regimens as the male cohort.
The DeMeester scoring system is recognized as the gold standard in evaluating GERD. The significance of a higher score outside of the 95th percentile compared with another high score within this range has not been elucidated in the literature. However, the finding of a statistically significant difference between the mean values in our two groups suggests that this may be used in the future as a predictive instrument in selecting patients for day-case surgery.
Using a multivariable analysis of gender, BMI, and DeMeester score, we derived a model based on logistical regression calculating the probability of being admitted following day-case LNF. Our equation suggests that being female has about twice the risk of being admitted. With a BMI above 30 kg/m2, a patient's risk of failed day-case surgery also doubles. Furthermore, the risk of failed day-case surgery increases by 0.855 for every 15 points rise in DeMeester score. Our model, the Tallaght LNF Score, has 83% accuracy in predicting admission status.
Even though our study is novel, we acknowledged its limitations of being a small, retrospective study in a single center. Other factors such as 24-hour pH monitor, esophageal manometry, and symptom index are factors that could also affect the indication for surgery and postoperative outcomes. Further multicenter prospective studies are needed to confirm our model's validity and generalizability.
In times of economic reform and stricter hospital budget, there is a larger emphasis on day-case surgery. Our study shows that LNF is feasible as a day-case strategy in the appropriately selected patients. We believe that preoperative assessment using the Tallaght LNF Score can improve patient selection for day-case surgery suitability, thus providing cost-effective measure by saving bed-days.
Conclusions
LNF has been shown to be feasible as a day-case procedure. However, there are still patients who require unplanned admissions postoperatively. In the literature, a definite scoring system has yet to be developed to identify potential patients who are at increased risk of being admitted postoperatively as failed day-case surgery. We found that being female, higher DeMeester score, and increased BMI are associatied with unplanned overnight stay. We developed the Tallaght LNF Score to risk stratify patients who have higher probability to be admitted following day-case LNF.
Footnotes
Disclosure Statement
No competing financial interests exist.