
Abstract
Abstract
Background:
Natural orifice translumenal endoscopic surgery (NOTES) is an emerging concept in the recent literature that could lead to potential benefits in clinical applications. The present study describes the initial clinical application in 15 cases of hybrid transvaginal and transumbilical NOTES and discusses the feasibility, safety, and potential benefits of the method.
Patients and Methods:
We evaluated the records of 15 patients who underwent hybrid transvaginal and transumbilical laparoendoscopic adnexal surgery between January 2010 and September 2011.
Results:
Procedures included salpingo-oophorectomy (n=7) and cystectomy (n=3) for ovarian tumors and salpingectomy (n=5) for unruptured tubal pregnancy. The mean operative time was 79 minutes (range, 49–116 minutes). Blood loss was minimal in all cases. All procedures were successfully performed, and there were no conversions to conventional multiport laparoscopy or open surgery. Gynecologic examination after 3 months showed no negative findings, and the cosmetic result was ideal with no visible scar.
Conclusions:
Hybrid transvaginal and transumbilical NOTES is feasible and safe in select patients, and it provides no visible scar.
Introduction
NOTES, which is performed via a natural orifice (i.e., the mouth, anus, or vagina), is currently a very important topic for surgeons. With evolution of technological innovations in laparoscopy, robotics, and therapeutic endoscopy, the morbidity related to incision access is low. Nevertheless, the potential benefits of even less invasive access could completely avoid incision-related complications (wound infection, adhesions, hernia, and incision pain). NOTES is even less traumatic to the abdominal wall and might further improve minimally invasive surgery of patients, but might also increase surgical risk when used by a transgastric or transcolonic approach.
In contrast, transvaginal NOTES has the potential advantages of providing easy access and closure under direct vision with available equipment used via an infection-controllable access. The present study describes the initial clinical application of hybrid transvaginal and transumbilical NOTES in 10 patients with ovarian tumors and 5 women with unruptured tubal pregnancy.
Patients and Methods
In this study, 15 patients underwent hybrid transvaginal and transumbilical laparoendoscopic adnexal surgery at Tokyo Medical and Dental University Hospital (Tokyo, Japan) between January 2010 and September 2011. All procedures were consecutively performed by a single surgeon (N.Y.) during the study period. Patient age and body mass index ranged from 32 to 50 years (mean, 41 years) and from 17.5 to 27.5 kg/m2 (mean, 22.1 kg/m2), respectively (Table 1). This study was approved by our institutional review board. All patients were informed about the intervention technique and provided written informed consent.
BMI, body mass index.
Surgical techniques
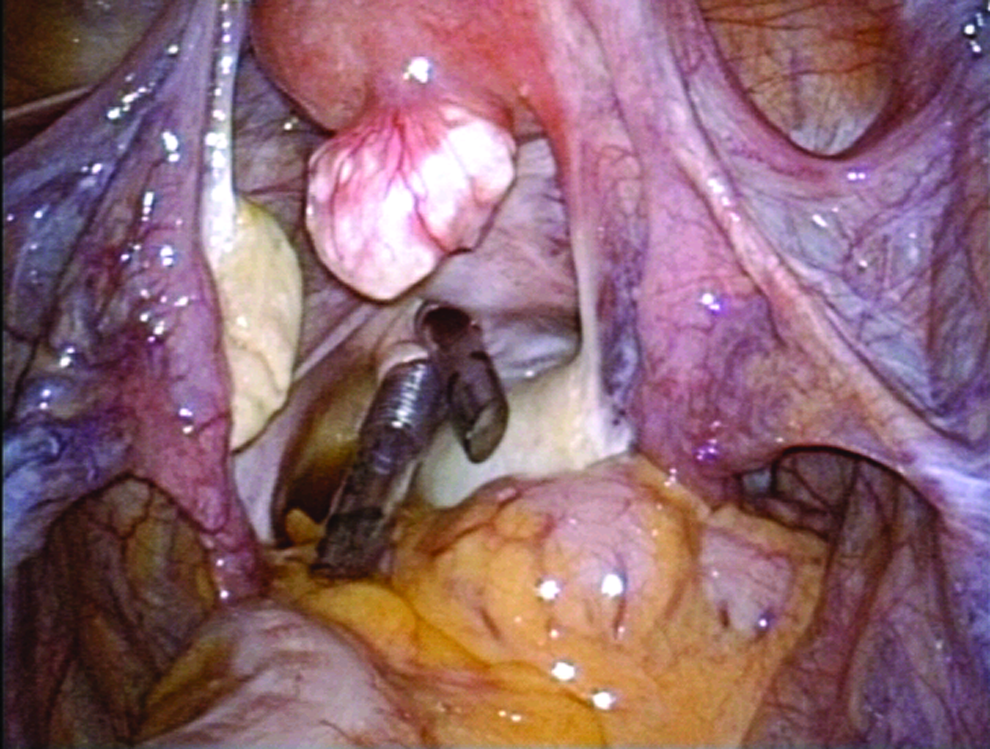
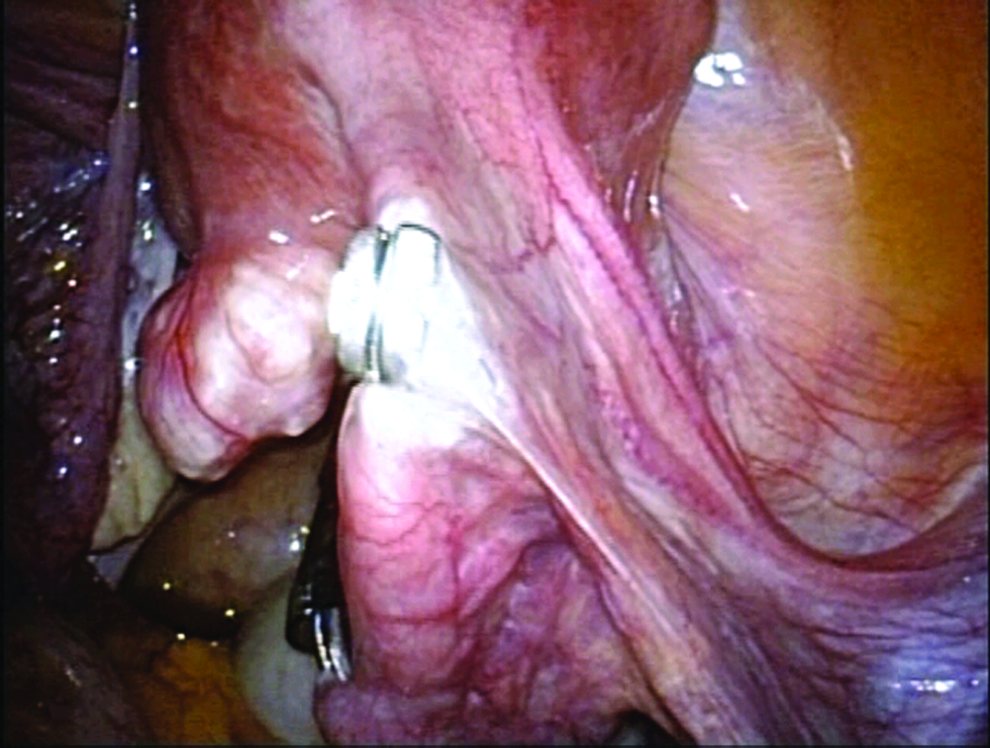
Once the patient was anesthetized, she was placed in the lithotomy position, and the abdomen and vagina were thoroughly sterilized and draped. A uterine manipulator was then inserted to provide adequate exposure of the pelvis. After creation of a <1-cm intraumbilical vertical skin incision, an adequate fasciotomy was made with the open technique. A 5-mm trocar was then introduced, and the pneumoperitoneum was inflated to 10 mm Hg. In the steep Trendelenburg position the pelvic cavity was explored with a 5-mm flexible videoscope (model LTF-VP; Olympus, Tokyo), and two 5-mm trocars were inserted through the posterior fornix of the vagina under laparoscopic control (Fig. 1). With use of a 5-mm flexible videoscope in the umbilicus, salpingo-oophorectomy, cystectomy, or salpingectomy was performed with either the conventional rigid or the more recent flexible grasper and a vessel-sealing device in the same fashion as single-incision laparoscopic surgery (SILS) (Fig. 2). After a transvaginal 5-mm trocar was exchanged for a 12-mm trocar, an EndoPouch® (Ethicon Endo-Surgery, Cincinnati, OH) was inserted transvaginally. With use of a 5-mm flexible videoscope through the vagina, adnexal specimens were retrieved in an EndoPouch and extracted transvaginally (Fig. 3). At the end of the procedure, the defects in the vagina were sutured with resorbable thread, and the fascial incision was closed, followed by skin closure (Fig. 4).
Inserting two 5-mm trocars through the posterior fornix of the vagina.
Dissection of the Fallopian tube using a vessel-sealing device.
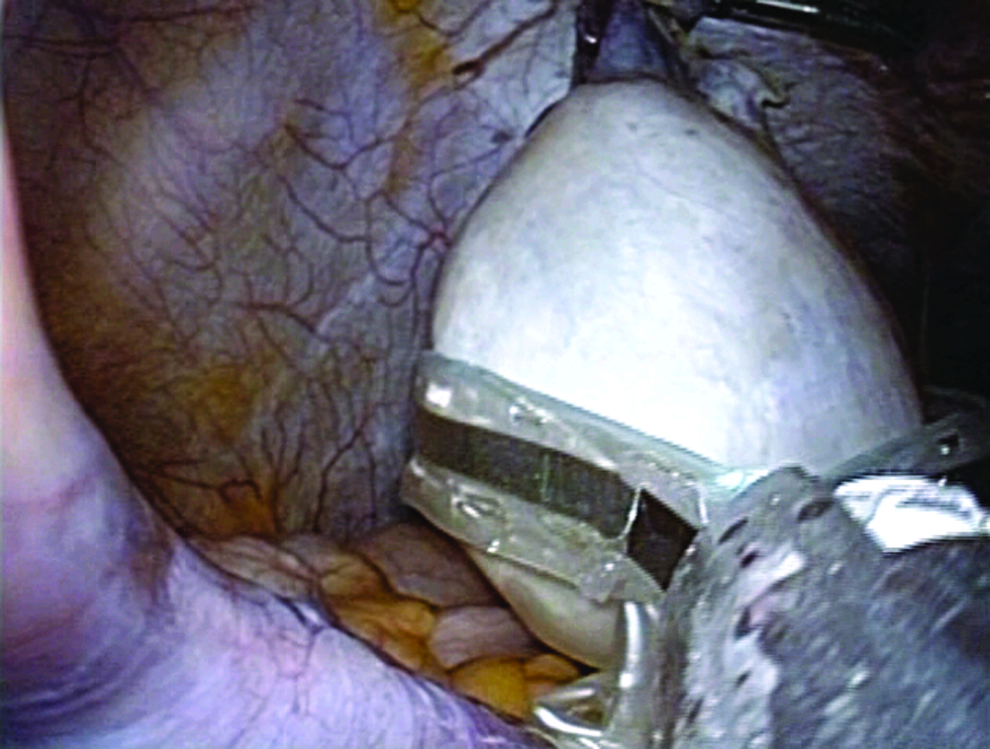
Retrieval of the adnexal tumor.

No visible scar after closure of the umbilical wound.
Results
Fifteen patients had hybrid transvaginal and transumbilical laparoendoscopic adnexal surgery performed during the study period. Table 1 presents the operative outcomes. Procedures included salpingo-oophorectomy (n=7) and cystectomy (n=3) for ovarian tumors and salpingectomy (n=5) for unruptured tubal pregnancy. The 7 patients with ovarian tumors who underwent salpingo-oophorectomy were older than 40 years of age, and the 3 patients with ovarian tumors who underwent cystectomy were under 40 years of age. The mean operative time was 79 minutes (range, 49–116 minutes). Blood loss was minimal in all cases. All procedures were successfully performed, and there were no conversions to conventional multiport laparoscopy or open surgery. Histologic findings of the adnexal tumors were as follows: mature cystic teratoma (n=6), mucinous cystadenoma (n=2), serous cystadenoma (n=1), and endometrioma (n=1). The postoperative course was uneventful in all patients. No postoperative complications were observed at follow-up in the outpatient clinic 3 months after surgery.
Discussion
The purpose of this study was to determine the feasibility, safety, and operative outcomes of hybrid transvaginal and transumbilical NOTES. Hybrid transvaginal and transumbilical NOTES was planned in a selected group of 15 patients and was successfully and safely completed in all patients without morbidity and with satisfactory and superior cosmetic results.
NOTES and SILS mark the beginning of a new era in the field of surgery. Endoscopic surgery via natural orifices is essentially surgery without a visible scar and marks a prominent evolutionary leap in medicine. Natural orifice endoscopic procedures are performed with a flexible endoscope, and at present most surgeons have little or more commonly no experience with its use in the abdominal cavity. In transgastric or transcolonic NOTES, the lack of sterilization and secure closure of the gastric or colonic wall remains the greatest challenge because the development of gastrointestinal leaks would represent a catastrophic complication that rarely follows routine laparoscopic surgery.
Transvaginal NOTES has many potential advantages over the transgastric approach. For example, the problem of effective and safe gastric closure has not yet been resolved. Furthermore, the use of the transgastric route can potentially lead to fistula formation and peritonitis, neither of which is an issue with vaginal access. Data in the literature prove that the vaginal approach has little risk,1,2 and our technique is even safer than these gynecologic operations as we control the insertion of transvaginal trocars laparoscopically.
Transvaginal access for NOTES has not been so extensively studied and published by researchers, perhaps because it could benefit only around 50% of the human population. Nevertheless, it could represent the safest and most easily applicable NOTES. The approach can be used relatively independent of new technology developments, with the potential benefit of controlled access and easy closure. In 1980, Reiner 3 presented his experience with 100 consecutive appendectomies done incidentally at the time of vaginal surgery. Transvaginal extraction after laparoscopy of the gallbladder and kidney was also previously described,4,5 and the route was also recently proposed for local dissection and anastomosis of rectal resection. 6 In 2003, Tsin et al. 7 used a transvaginal laparoscopic camera for cholecystectomy in patients with simultaneous hysterectomy, naming the procedure as “culdolaparoscopy.” Despite the availability of transvaginal access and the absence of the potential risks associated with other NOTES approaches, publications about transvaginal access for NOTES are still to come.
Recently, innovative techniques of NOTES and SILS have been applied in the field of general surgery as a step toward even more less-invasive procedures. As a bridge between conventional multiport laparoscopy and NOTES, recent focus has been on the development of SILS to further minimize the invasiveness of laparoscopy by reducing the number of incisions and, it is hoped, the pain and complications associated with them. In fact, it seems in our series that SILS can be performed in all cases. However, the potential advantage of hybrid transvaginal and transumbilical NOTES over SILS includes better cosmesis from no visible scar because only a 5-mm trocar is inserted within the umbilicus.
We performed hybrid transvaginal and transumbilical NOTES using common laparoscopic instruments. Transvaginal procedures were the same as SILS. The insertion of instruments through the posterior fornix of the vagina and the closure of these wounds were easy. Because the technical ease of the procedure and early outcome are satisfactory, transvaginal access for NOTES seems to be feasible and safe for clinical application.
In conclusion, we have successfully performed hybrid transvaginal and transumbilical laparoendoscopic adnexal surgery. Hybrid transvaginal and transumbilical NOTES is feasible and safe in select patients. Limitations of the present study include the small number of reported cases. Further study is necessary to better define surgical outcomes obtained from hybrid transvaginal and transumbilical NOTES and to assess the relative benefits of this novel surgical approach compared with SILS.
Footnotes
Disclosure Statement
No competing financial interests exist.