
Abstract
Abstract
Background:
The majority of current literature regarding laparoscopic inguinal hernia repair group all their pediatric patients together. This study aimed to evaluate the long-term outcomes of patients who underwent laparoscopic intracorporeal inguinal hernia ligation under the age of 1 year to ascertain if there were hidden advantages or limitations in this particular group.
Patients and Methods:
Patients under the age of 1 year at time of laparoscopic intracorporeal inguinal hernia ligation by a single pediatric surgeon were identified. Data were obtained from case notes, hospital electronic records, and parental telephone consultation.
Results:
One hundred fourteen patients under the age of 1 year underwent laparoscopic inguinal hernia repair from November 2003 to October 2010. The male:female ratio was 4:1. The mean corrected age at surgery was 15.5 (range, 3–42) weeks, and the mean weight at surgery was 5.3 (range, 1.9–9.8) kg. All patients' case notes and electronic records were accessed. Forty-two percent of parents were contactable (mean of 4 years following surgery). There was one recurrence on the asymptomatic side in a boy that presented 3 years later. Five patients required orchidopexy following laparoscopic hernia repair, although 3 cases were known to be undescended at the time of surgery. One patient had intermittent ipsilateral groin swelling that resolved spontaneously after 6 months.
Conclusions:
Laparoscopic intracorporeal inguinal hernia ligation in patients under the age of 1 year is safe and effective. Recurrence rates may be lower than those in patients under 1 year of age undergoing a traditional open repair. However, there may be a higher rate iatrogenic of cryptorchidism in this laparoscopic group.
Introduction
The laparoscopic approach for pediatric inguinal hernia repair remains controversial in the literature. A recent meta-analysis by Alzahem3 concluded that laparoscopic inguinal herniotomy is significantly associated with longer operating times and a reduction of metachronous hernia development. There was a trend also toward a higher rate of recurrence in laparoscopic repairs.
There is, however, a paucity of articles published specifically regarding infants under the age of 1 year at time of surgery4–6 with a mean follow-up of only 1 year 4 and 26 months.5,6 Many of the published articles on laparoscopic pediatric inguinal hernias group their patients together7,8 and therefore may mask benefits or shortfalls of this approach. The aim of our study was to determine the long-term outcomes of patients who underwent laparoscopic inguinal hernia repair when under the age of 1 year at the time of surgery.
Patients and Methods
Patients who underwent laparoscopic inguinal hernia repair under the age of 1 year at the time of surgery between November 2003 and October 2010 were identified from a single pediatric surgeon's prospectively collected database.
Surgical technique
All patients underwent general anesthesia and endotracheal intubation and were placed in the supine position. A 5-mm camera port was inserted under vision via a vertical transumbilical incision. Carbon dioxide was used to create the pneumoperitoneum with intra-abdominal pressures initially at 12 mm Hg for insertion of working ports and then lowered to 8 mm Hg for the hernia repair. Two 3-mm working ports were inserted in the flanks below the level of the umbilicus under direct vision. A three-port technique was used as this is a well-described method in the literature 9 that the lead consultant had been trained to perform. Initial laparoscopy with a 30° 5-mm camera was undertaken to assess the hernial orifices (Fig. 1). The hernial orifice was deemed open if there was palpable air within the ipsilateral scrotum or inguinal canal and if the tip of the laparoscopic needle holder could be passed into the orifice so that the jaws could no longer be seen. Before closure, any hernial contents were returned into the abdominal cavity. An Ethicon (Blue Ash, OH) 4/0 Prolene® suture (nonabsorbable, monofilament) on a 17-mm round-bodied needle was passed into the abdominal cavity through the anterior abdominal wall. The hernia was closed with a peritoneal purse-string (Fig. 2) that was tied intracorporeally (Fig. 3). Herniorraphy was not undertaken. If the contralateral hernia orifice was deemed to be open, it was closed at the same time with the same technique. The needle was removed with the working ports. The umbilical port site was closed with 4/0 Vicryl® (Ethicon) for the deep fascia and 5/0 Vicryl for subcuticular closure. The 3-mm working port sites were closed with a single 5/0 Vicryl subcuticular suture. Local anesthetic was infiltrated at the end of the operation (1 mg/kg of 0.25% levobupivacaine hydrochloride [Chirocaine®; Abbott, Abbott Park, IL]). If there were no anesthetic or postoperative concerns, patients older than 4 weeks if they were born at term or over a corrected age of 20 weeks if premature were discharged home the same day.
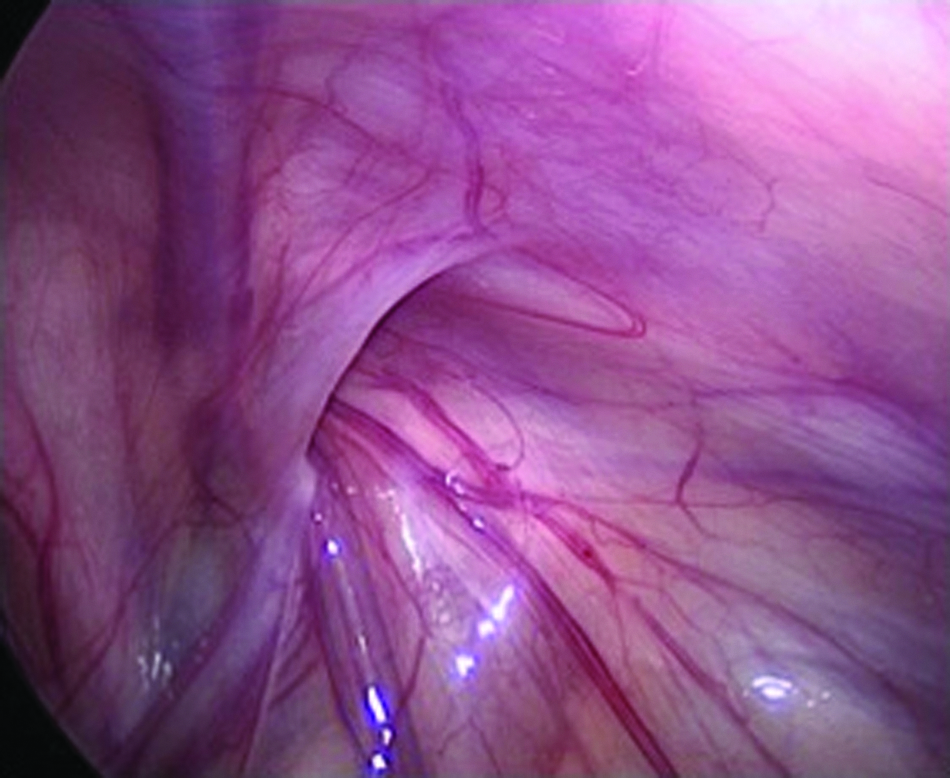
An open right deep inguinal ring.
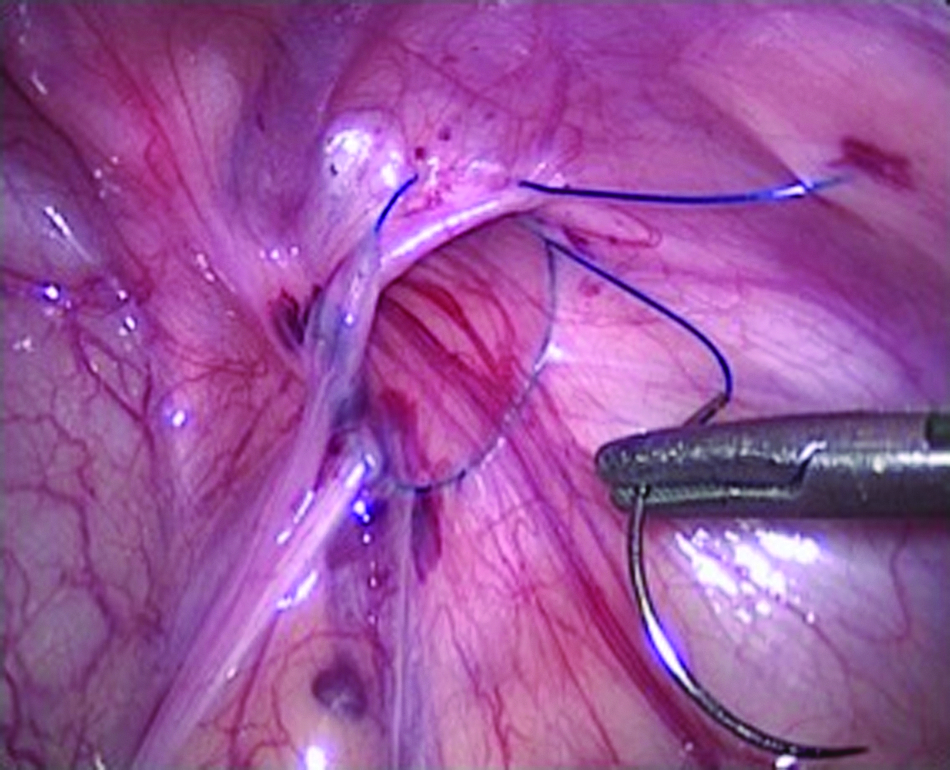
Peritoneal purse-string around the open right deep inguinal ring.
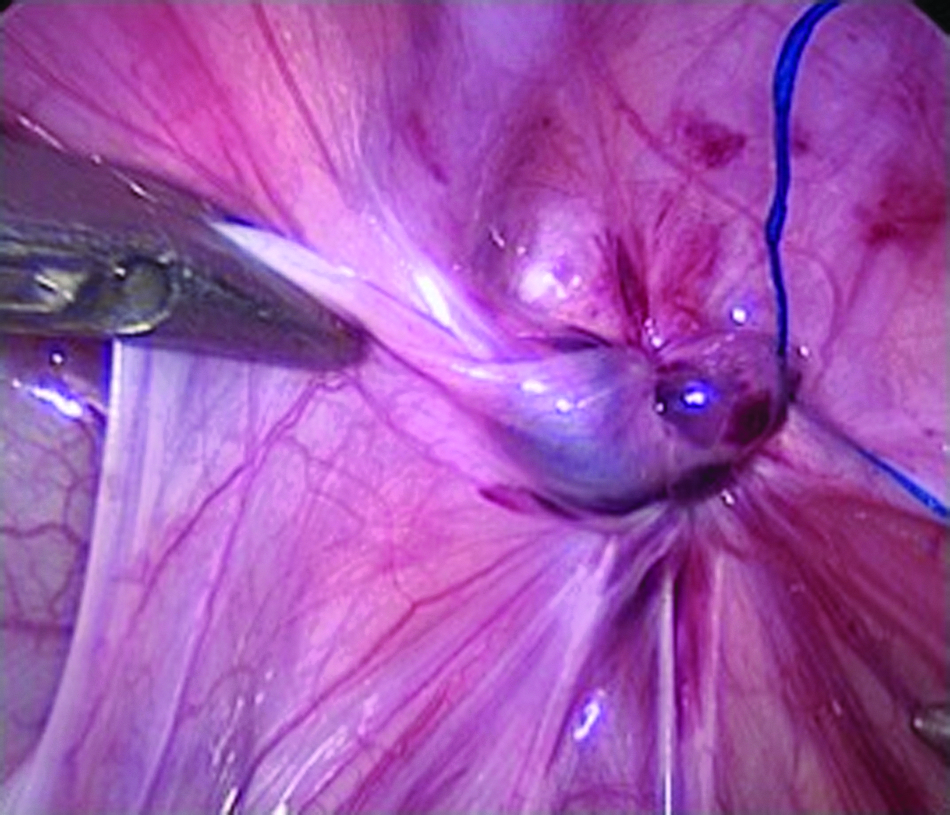
Right deep inguinal ring closed with a purse-string suture.
Operating surgeon
The seniority of the operating surgeon was recorded prospectively. The consultant surgeon was always in attendance throughout the operation. The operation was divided into three stages:
1. Entry into the peritoneum and insertion of the camera and working ports 2. Insertion of the needle and placement of a peritoneal purse-string around the hernial orifice 3. Closure of the hernial orifice by tying the purse-string with an intracorporeal knot
Follow-up evaluation
All patients were seen routinely in the outpatient clinic 4 months following surgery and subsequently discharged to the general practitioner if there were no concerns at the time of the clinic review.
Long-term outcomes were obtained by triangulating:
1. Retrospective case notes analysis. 2. Electronic hospital records. The patient identification number was also cross-referenced with the electronic hospital records. Therefore, if the patient was referred back to our Department under another pediatric surgeon, he or she could still be identified. Also, we could assess whether the same patient had been referred or been seen in our hospital for any condition since the hernia operation up until the search date of September 2011. 3. Telephone consultation. If there was a time interval of more than 1 year since the last clinic consultation, a telephone consultation in the form of a questionnaire with the parent was undertaken. Those who had concerns were offered a clinic appointment for a more formal review.
Parental questionnaire
Parents were asked to answer the following questions:
1. Has the lump returned since the last clinic review? (Yes/No) 2. (If boy) Any concerns about the size of the testes? (Yes/No) 3. (If boy) Any concerns about the position of the testes? (Yes/No) 4. Did your child have to have any more surgery? (Yes/No) 5. Appearance of port scars (on a scale of 1–5 where 1=Very unhappy and 5=Very happy). 6. Did your child have to see a doctor following the operation (not including the routine outpatient appointment) and why?
Results
Patient demographics
Over 7 years, 114 patients who underwent laparoscopic inguinal hernia repair when under 1 year of age were identified. There were 93 boys and 21 girls (male:female ratio=4:1). Mean corrected age at time of surgery was 15.5 (range, 3–42) weeks. Mean weight at surgery was 5.3 (range, 1.9–9.8) kg. Eighteen cases had a repair undertaken as an emergency due to current or recent (within 24 hours) hernia incarceration.
Operative data
Seventy-two patients presented with a right inguinal hernia, 36 presented with a left inguinal hernia, and 6 patients had bilateral inguinal hernias. An asymptomatic open contralateral deep inguinal ring was found in 32 patients, of whom 19 patients had an open contralateral deep ring on the left and 13 patients on the right. All were closed during the same operation.
Conversion to open procedures (1.8%) was needed in 2 patients. In 1 patient, there was a persisting failure to maintain the pneumoperitoneum; the other procedure showed failure to progress. Both these conversions occurred in the early period of this series.
There were no anesthetic concerns noted intra- or postoperatively. All patients were discharged home the same or following day except for 2 patients who had some ileus following reduction of incarcerated bowel.
Performing surgeon (Table 1)
Although the lead consultant was always in attendance and supervising, the performing surgeon was more likely to be a surgical trainee in the later years compared with the start of the series.
Length of surgery
Length of surgery was defined as the start of skin preparation until when the skin closure was completed. The mean operation time for single-side surgery was 57 (range, 34–80) minutes in boys and 54 (range, 34–71) minutes in girls. The mean operation time for bilateral repair was 72 (range, 48–110) minutes in boys and 54 (range, 46–69) minutes in girls.
Follow-up
The average clinic follow-up was 4 months with 92% attendance. As only patients operated on up to October 2010 were included, all required telephone consultation and electronic database review. All patients' case notes and electronic records were accessed. Forty-two percent of the parents were contactable over a 3-month period. Mean telephone postoperative follow-up was 4 (range, 1–7) years.
Outcomes
Recurrence
Excluding the 2 patients who were converted to open procedures, there were 150 deep inguinal rings that were closed laparoscopically. There was only one recurrence (0.7%), which was in a boy on the asymptomatic side that was closed 3 years previously at the same time the symptomatic side was closed. This recurrence was successfully closed laparoscopically with no recurrence after 2 years. One patient (0.7%) had intermittent groin swelling ipsilateral to the operated side, but this resolved spontaneously by 6 months without surgical intervention. No patient so far has presented with a metachronous hernia.
Umbilical hernia
Three patients (2.6%) were noted to have a small iatrogenic umbilical hernia at the 4-month clinic follow-up. None of these patients has subsequently required surgical closure.
Orchidopexy
Five boys (5.4%) required an orchidopexy 1–4 years following laparoscopic inguinal hernia repair. Three patients were known to have an undescended testis at the time of initial surgery, and these patients underwent a scrotal orchidopexy. Two patients (2.4%) had a combined total of three testes that initially were thought to be scrotal but following laparoscopic inguinal hernia repair later required orchidopexy. One patient was referred to and operated on by another pediatric surgeon who was identified through the electronic records.
Testicular atrophy
There were no documented cases of testicular atrophy at the 4-month clinic check. One of the 5 patients who underwent orchidopexy was noted to have a slightly smaller-volume testis 2 years following his orchidopexy.
Parental questionnaire
Forty-two percent of parents were contacted and completed the questionnaire:
1. Has the lump returned since the last clinic review? No (100%). 2. (If boy) Any concerns about the size of the testes? No (100%). 3. (If boy) Any concerns about the position of the testes? No (100%). 4. Have they had to have any more surgery? No (100%) (excluding further surgery mentioned previously). 5. Appearance of the port scars (on a scale of 1–5, where 1=Very unhappy and 5=Very happy) was a mean of 4.8 (range, 3–5). 6. Did your child have to see a doctor following the operation (not including the routine outpatient appointment) and why? Five parents took their child to see their general practitioner in the early postoperative period for a matter related to the surgical wound. No return to the general practitioner for other matters was reported.
Discussion
Inguinal hernia repair remains one of the most common surgical procedures in infancy. Reported advantages of the laparoscopic approach include a higher detection rate of a contralateral open deep inguinal ring, 2 improved visualization, less pain, earlier recovery, and better cosmesis. 10 There have been concerns regarding the higher rates of recurrence in laparoscopic surgery (4%) compared with 2% in open surgery, 3 and the articles referenced had patients ranging from 3 months to 18 years.10,11 Recent articles studying patients under the age of 1 year 4 and babies weighing 5 kg or less 6 have suggested that the recurrence rate may be lower in the subset of patients undergoing laparoscopic surgery under the age of 1 year than those quoted for open procedures. Their reasoning for this is related to the thin sac that needs to be dissected in open surgery and the advantage of a magnified field of view during laparoscopic surgery so that sutures can be positioned precisely.
We had only one recurrence on the asymptomatic side of a young boy that was subsequently closed laparoscopically with no recurrence after 2 years. Our rate of 0.7% compares favorably with 1.3% in the under 1 year of age population in the study by Esposito et al. 4 Baird et al. 12 have published their series of children under the age of 2 years who underwent a traditional high ligation of the sac following groin incision. Separating their 111 patients under the age of 1 year in their series, our recurrence rate is lower than theirs of 2.7% and also compares favorably with the meta-analysis by Alzahem3 with an open inguinal hernia repair recurrence rate of 0%–2%.
Testicular ascent
Esposito et al. 4 did not report any iatrogenic testicular ascent in their series, although their follow-up was on average only 1 year. However, Turial et al., 6 dealing with babies weighing under 5 kg, found that 4.1% of post-laparoscopic hernia repair required orchidopexy. Our series had a lower rate of 2.4% iatrogenic cryptorchidism, but our mean weight at time of surgery was 5.3 kg, which is higher than the mean weight of 3.9 kg in the cases of Turial et al. 6 They calculated a 65.5% increase in risk for secondary high testis for each 1 kg less in weight. The group studied by Baird et al. 12 of patients under 1 year of age undergoing an open procedure had a rate of iatrogenic cryptorchidism of 0.9% after a minimum of 1 year, but the researchers did not state the mean duration of follow-up.
In our series, all patients who required an orchidopexy following laparoscopic inguinal hernia repair had the purse-string suture placed by the consultant but the intracorporeal knot tied by the trainee. Perhaps an explanation could be overzealous tightening of the purse-string by the trainee, to prevent recurrence, which could have caused the testicular ascent, but this is merely conjecture.
Telephone consultation
The telephone consultation did not highlight any further complications that were not identified from reviewing the case notes and cross-referencing of electronic databases. The majority of the parents were quite knowledgeable regarding possible long-term complications and the need for review if there were any concerns. Although only 42% of parents were contactable, this was not an insignificant proportion and allowed us to ascertain follow-up for up to 7 years in some of these patients with mean follow-up by telephone of 4 years. No parents had a concern such that they requested a clinic consultation.
Cosmesis is a reported advantage of laparoscopic surgery, and the parental feedback in our study supported this with an average score of 4.8, indicating a “good” to “very good” appearance of the port sites.
Training
This is one of the few articles to qualify the grade of the surgeon undertaking the steps of the procedure. We feel that it is vitally important to document this in publication as the seniority of the operating surgeon may affect the outcome. Also, this Department is a designated training center for pediatric surgical trainees, and so outcomes are analyzed methodically.
We have divided the operation into three broad steps: (1) entry into the peritoneum via the Hassan technique and insertion of the camera and working ports; (2) completion of a peritoneal purse-string; and (3) intracorporeal knot tying. The primary surgeon's grade was recorded immediately at the end of each operation. In the consultant's earlier years in this series (2003–2006), the majority of stages were undertaken by himself personally. The trainee only inserted the ports in 22% of cases, placed the purse-string in 7% of cases, and tied the knot in 29% of cases. In the later years (2007–2010), with consultant supervision, the trainee inserted ports in 91% of cases, placed the purse-string in 30% of cases, and tied the knot in 77% of cases.
Among the operations performed by the trainee, there were no recurrences. All 5 patients who subsequently required an orchidopexy whether known or unknown at the time of surgery had the knot tied by the trainee and the purse-string placed by the consultant. The only case that had intermittent swelling in the groin, which self-resolved, was performed by the trainee. Unfortunately, closure of the port sites was not recorded. These complication rates are still comparable to published series in the infant group as discussed earlier.
Cost-effectiveness
Although the average operating times are higher than in those reported in the literature, it must be noted that the times are recorded from skin preparation and therefore include equipment placement and preparation. Also, as mentioned, many of these cases are training cases, and so time is allocated for the trainee to perform the procedure competently. The overall costs were the same for both laparoscopic and open inguinal hernia repair.
Limitations
Limitations of this study include that not all parents could be contacted via telephone to complete the questionnaire. This was in part compensated for by cross-referencing the patient's identification number to check whether he or she had been referred back with a related complication to the hernia surgery. For those who did complete the questionnaire, our results are very much dependent on their observations of their child and their perception of normal.
The maximum length of follow-up was 7 years, making the oldest child in our series approximately 8 years of age. Even longer follow-up when these patients are postpuberty may be advisable to ensure adequate testicular growth and position.
Conclusions
Laparoscopic intracorporeal inguinal hernia ligation is feasible, safe, and effective in patients under the age of 1 year. The recurrence rate seems to be lower compared with those undergoing the traditional open approach in those under 1 year of age. If patients are asymptomatic at their 4-month review, they can be safely discharged back to the care of their general practitioner, but parents should be made aware of the low possibility of later orchidopexy even if not necessary at time of hernia surgery.
Disclosure Statement
No competing financial interests exist.