
Abstract
Abstract
Introduction:
This study aimed to evaluate success and complications of laparoscopic transperitoneal ureterolithotomy at our center.
Patients and Methods:
From November 2008 until September 2011, 33 patients, including 22 men and 11 women, with a mean age of 45.3 years (range, 19–67 years), underwent laparoscopic ureterolithotomy at our center. Locations of stones were the upper, middle, and lower ureter in 29, 1, and 3 patients, respectively. Ten patients had a history of previous abdominal or pelvic surgery. Laparoscopic ureterolithotomy was performed via a transperitoneal approach. Complications and outcomes were evaluated.
Results:
Mean operation time was 85.48±15.11 minutes. Except for one stone migration and one conversion to open surgery, all the ureteral stones were extracted laparoscopically (94% success rate). A double J stent was inserted antegradely during the procedure and remained for about 1 month in all cases except in 1 patient in whom both antegrade insertion and ureteroscopic relocation were used. Postoperative hypercapnia was detected in a young patient, who recovered with conservative treatment. No visceral complication occurred. The mean hospital stay and the drain installation interval were 4.1 days (range, 3–9 days). The mean return to full activity was 11.91±4.65 days. Preoperative hydronephrosis resolved at follow-up ultrasonography (3 months later) in all patients except 2 cases, in whom intravenous pyelography showed no obstruction (memorial hydronephrosis).
Conclusions:
Laparoscopic transperitoneal ureterolithotomy is a safe and effective treatment modality for skilled surgeons and a convenient option for patients. Challenges, such as lower ureteral stones, redo cases, and antegrade double J stent insertion, can be overcome by experience.
Introduction
Patients and Methods
From November 2008 until September 2011, 33 patients, including 22 men and 11 women, with a mean age of 45.3 years (range, 19–67 years), underwent laparoscopic ureterolithotomy at our center. Indication for the procedure was SWL or transureteral lithotripsy failure or impacted and large stones.
Pre- and postoperative parameters, including history of previous abdominal or pelvic surgery, history of previous open ureteral and renal surgery, the operation time, hospital stay, complications, stone migration, return to full activity, and drain activity of more than 100 mL, were evaluated. Ultrasonography and intravenous pyelography had been performed prior to the procedure in all the patients to clearly define the ureter anatomy and to test the renal function.
Laparoscopy was performed via the transperitoneal approach in all the patients in the flank position. Classically, four trocars were inserted. The retroperitoneal course of the ureter became exposed once the colon or sigmoid was reflected medially. Once the stone was located, a longitudinal incision was made in the ureter using a monopolar laparoscopic diathermy hook. After stone removal with grasping and antegrade ureteral double J stent insertion, the ureterotomy was reapproximated over the ureteral catheter using a 4-0 Vicryl® (Ethicon, Somerville, NJ) suture. According to our center policy, we preferred to maintain a double J stent for about 1 month in laparoscopic ureteral surgery. An intraperitoneal drain was inserted in all the patients at the end of the procedure to prevent urinoma or blood collection.
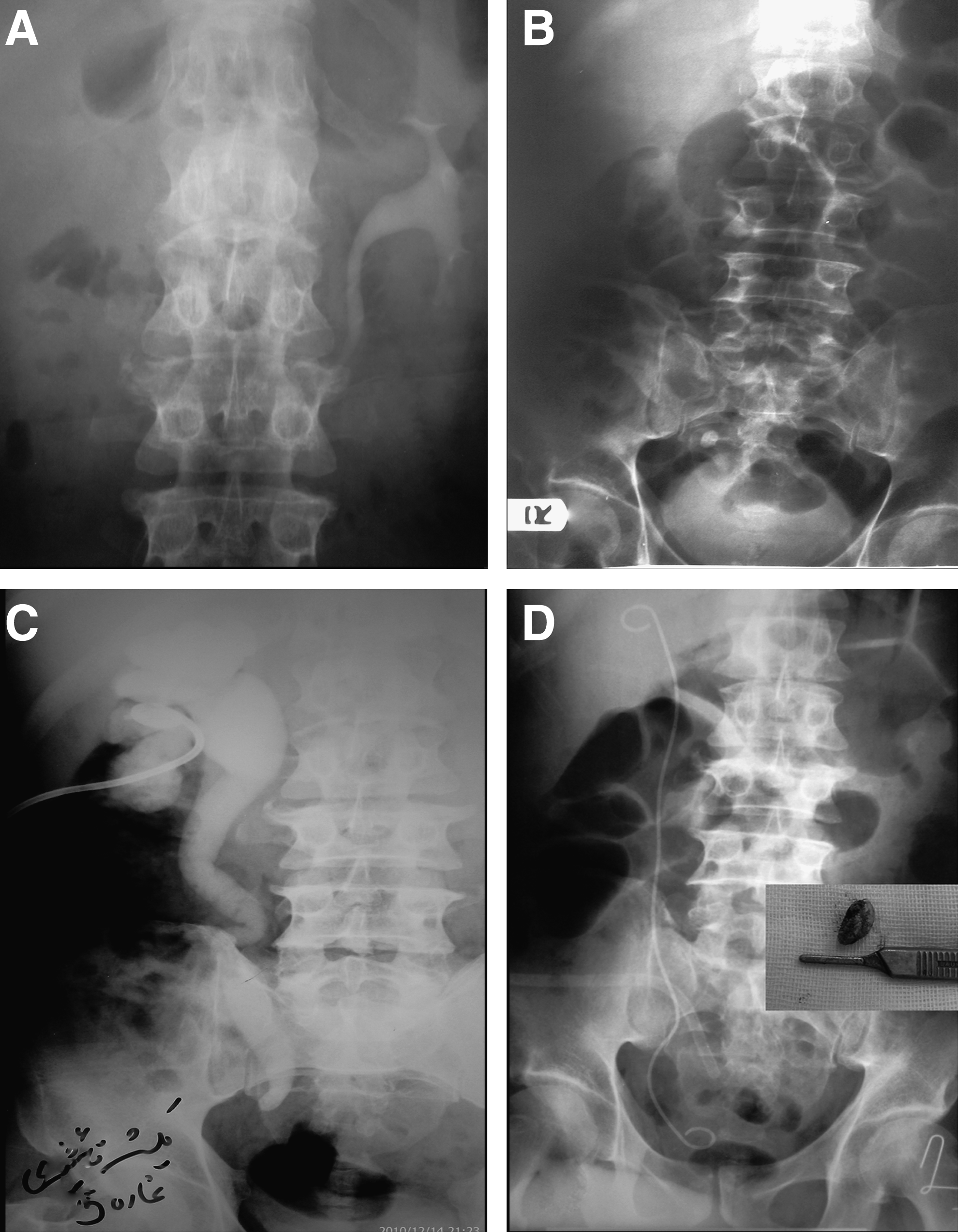
All the patients were followed up with a kidney, ureter, and bladder x-ray the day after the surgery (Fig. 1) and ultrasonography at least 3 months postoperatively. Pre- and postoperative ultrasonographs were then compared. The hospital and follow-up records of the patients were reviewed, and complications and outcomes were evaluated. For statistical analysis, the 95% confidence interval was used.
Results
Demographic characteristics and outcomes are presented in Table 1. Ten patients had a history of previous abdominal or pelvic surgery, including one obese woman with a history of hysterectomy and previous ipsilateral ureter surgery. History of SWL or transurethral lithotripsy was reported in 12 patients. Sizes of stones varied between 16 and 35 mm.
SD, standard deviation.
Except for one stone migration (in a patient with an upper ureteral stone who was referred for SWL) and one conversion to open surgery (due to obesity and severe adhesion in a man with lower ureteral stone), all the ureteral stones were extracted laparoscopically (94% success rate). A double J stent was inserted antegradely during the procedure and remained for about 1 month in all the cases except 1 patient, in whom both antegrade insertion and ureteroscopic relocation were used (97% success rate).
Complications occurred in 3 (9%) patients. Postoperative hypercapnia was detected in a young patient, who recovered with conservative treatment. Pyelonephritis was seen 20 days after the operation in 1 patient with diabetes mellitus and history of pyonephrosis drainage 1 month before laparoscopy, who needed rehospitalization and medical treatment (Table 1). No major postoperative complication occurred. All the complications were Grade II according to the Clavien–Dindo grading system. 9 There was no damage to the ureter and adjacent viscera. A decrease in hemoglobin necessitating blood transfusion did not occur in any patient. There was no residual fragment in any patient.
During the follow-up period, no ureteral stricture or ureteral obstruction occurred. Preoperative hydronephrosis resolved at the follow-up ultrasonography (3 months later) in all the patients except 2 cases, in whom intravenous pyelography revealed no evidence of obstruction or stricture (memorial hydronephrosis).
Discussion
Minimally invasive procedures, such as SWL, flexible ureteroscopy, and percutaneous surgery, have opened new horizons in management of urinary stone disease.1,2 However, open ureterolithotomy should be considered as the last resort just in complicated cases or when SWL or other less invasive endourologic approaches fail.3,5,6 In these situations, laparoscopic ureterolithotomy is used following a failed ureteroscopy or as a salvage procedure for SWL.1,7,10–12 Stones in the megaureter, large impacted ureteral stones, and need for laparoscopy for other purposes are more indications for the laparoscopic approach. 1
In developing countries, where endourologic facilities and SWL are not easily accessible,13,14 open surgery is common, 2 and laparoscopic ureterolithotomy has gained popularity as a less expensive procedure. 15 In contrast, in developed countries, indications for laparoscopic uretrolithotomy are limited because of improvement in endoscopic technology, especially the combination of flexible ureteroscopy and holmium laser lithotripsy, which facilitates treatment of large proximal ureteral stones.16–18
Because alternative techniques, such as ureteroscopy, percutaneous stone extraction, and SWL, have been very effective, urologists are reluctant to perform laparoscopic ureterolithotomy. 2 A success rate of almost 100% is reported in the literature for the treatment of ureteral calculi using ureteroscopy with a lithotripter and a basket. 2 Comparison of different minimally invasive modalities for the management of ureteral stones indicates that accessibility of devices and the urologist's expertise affect the treatment option.10,11,19 There are no flexible ureteroscopes or laser lithotripter at our center. Furthermore, most of the patients, especially those with socioeconomic problems, prefer that their stone be removed in a single procedure.
It is difficult to compare results of open surgery with laparoscopic ureterolithotomy because of restricted indications for open surgery and high successful rates of laparoscopic ureterolithotomy. 4 However, lesser requirement for analgesics, shorter hospitalization and convalescence, and better cosmetic results are reported for laparoscopy in comparison with open surgery.20–22
The first retroperitoneal and transperitoneal ureterolithotomies were carried out in 1979 23 and 1992, 24 respectively. The retroperitoneal technique was later popularized by Gaur and co-workers13,24 and has significantly developed in the field of urology over the past 20 years. No clear benefit has been reported in performing a transperitoneal versus an extraperitoneal approach for laparoscopic ureterolithotomy by experienced urologists20,25; however, significant differences were observed in favor of the transperitoneal procedure with regard to time interval for access to an operating field, time for suturing the ureter, and total operation time. It was concluded that novice urologists should perform laparoscopic ureterolithotomy using a transperitoneal approach, 26 which allows better identification of anatomical landmarks and more working space.27,28
Laparoscopic ureterolithotomy is specifically appropriate for a solitary large stone (>1.5 cm) in the proximal ureter between the lower border of the kidney and the common iliac vessels. In contrast, proximal stones are mostly approached percutaneously, and stones below the iliac vessels via ureteroscopy. Furthermore, only minimal dissection is needed to locate the ureter. 29 Another significant benefit of laparoscopic ureterolithitomy is the possibility of removing the entire large ureteral stone in a single procedure.2,12,29
A drawback to laparoscopic ureterolithotomy is prolonged urinary leakage, which may lead to small bowel adhesions, urinoma formation, risk of injury to adjacent tissues, and the probability of conversion to open surgery.1,4,12,15,29 In addition, a long learning curve and expertise are needed to perform the laparoscopy.2,4 Furthermore, because it is difficult to differentiate the ureter from the gonadal vein, locating the ureter may be problematic. 12 Moreover, intensive peri-ureteral fibrosis following infection, ureteritis, SWL, or ureteroscopy can cause hardship in locating the stone, particularly if the stones are small and not big enough to be visible. 21 Absence of sensible feedback is another disadvantage of laparoscopy. 2
In this study, we performed laparoscopic transperitoneal ureterolithotomy as the first-line procedure in cases with a large stone (>1.5 cm) in the proximal ureter or in patients who desired to have their stones removed in a single procedure or as a salvage procedure after SWL or failed ureteroscopy. Mean operation time in our study was 85.48±15.11 minutes, which is superior to that of many transperitoneal reports.8,12,27,29–32 This difference may be due to the fact that our procedures were performed by a single expert laparoscopist and not by a surgical team receiving training.
The stone-free rate of 83%–100% and a low conversion rate confirmed the safety and sufficiency of laparoscopic ureterolithotomy performed by skilled surgeons. 1 In the largest series of laparoscopic ureterolithotomy on 123 patients, the extraperitoneal versus intraperitoneal approach for laparoscopic proximal ureterolithotomy was compared. A stone-free rate of 96.7% was reported. The operation time was significantly different in favor of the intraperitoneal approach (137.3±52.2 minutes versus 171.3±91.3 minutes; P=.02). Minor complications occurred in 11.4% of patients. Conversion to open surgery was required in 1 patient because of migration of the calculus. 8
In our study, the stone-free rate was 95.8% due to one conversion and one migration. The operation time and rate of conversion to open ureterolithotomy are associated with difficulty in dissection and the surgeon's skills. 2 Furthermore, the stone migration can be prevented by holding the ureter with a Babcock forceps. 21
Although the technique of placing the stent via laparoscopy was considered difficult by some authors, 33 we succeeded in inserting a double J stent antegradely in 96% of patients. In contrast, because of mentioned difficulties, Goel and Hemal 21 only placed the stent in patients with stone impaction and poor renal function; hence, they did not place it in 20 of the last 26 patients of their series. In some studies, stent usage was infrequent.15,22,29 We believe that inserting a double J stent prior to the procedure does not have any extra advantage and may take away significant operating room time. Average hospital stay was 4.1 days (range, 3–9 days) in our laparoscopic surgeries, which is similar to that of other studies. 1
The most common complication of laparoscopic ureterolithotomy is prolonged urinary leakage, which is observed in those patients in whom the ureterotomy is not closed or a ureteral stent is not placed. 1 Gaur et al. 13 reported that postoperative urinary leakage is highly reduced if the ureter is both stented and sutured. Demirci et al. 34 concluded that suturing of the ureter is more effective than placement of the double J stent into the ureter to reduce urine extravasation. We used laparoscopic watertight suturing and inserted a double J stent in all of the cases of transperitoneal ureterolithotomy. Therefore, prolonged urine leakage or urinoma or delayed ureteral stricture did not occur. However, the ureter incision suturing was not performed in some studies. 35 Gaur et al. 15 reported that in retroperitoneal access, the ureteral catheterization is sufficient in cases with a tender, edematous, and inflamed ureter, and suturing is not recommended.
Ureteral stricture is the most serious late complication of laparoscopic ureterolithotomy with an incidence rate of up to 20%.20,29,30 Urinary leakage, periureteritis, stone impaction, and use of diathermy to incise the ureter are the leading factors that result in ureteral stricture. 1 Ureterotomy is mostly done with a cold knife; however, some surgeons use the diathermy hook 27 or a neodymium:yttrium-aluminum-garnet laser. 36 Because no ureteral fixation is needed and also an accurate incision is made with accompanying hemostasis, applying the diathermy is much easier than using a cold knife. Furthermore, the ureteral healing process is eventless with diathermy. 15 Although suturing of the ureterotomy too tightly may result in wall ischemia and subsequent stenosis,37,38 some recommend the watertight ureteral closure to decrease the urinary leakage, stricture formation, and postoperative ileus. 33
In this study, no major complications, such as rupture of the ureter, urinary leakage, or hemoperitoneum, occurred. After laparoscopic surgery, only 1 patient showed symptoms of dyspnea and hypercapnia, which were controlled with conservative management. One patient who showed pyelonephritis 2 weeks after the operation was rehospitalized and treated. As Table 1 shows, complications were not significant (Grade II according to the Clavien–Dindo grading system 9 ).
Conclusions
Laparoscopy is not a replacement for SWL or ureteroscopic techniques; however, it is a safe and effective treatment modality when other techniques fail or are unavailable. Challenges, such as lower ureteral stones, redo cases, and antegrade double J stent insertion, can be overcome by relevant experience.
Footnotes
Disclosure Statement
No competing financial interests exist.